Yamamoto, Janet Ph.D.
advertisement

RETROVIROLOGY
ONCONOVIRUSES & LENTIVIRUSES
Retrovirus Family / Taxonomy
Retrovirus Structure & Morphology
Retrovirus Genomic Organization
Retrovirus Replication Cycle
HIV-1 EPIDEMIOLOGY & THERAPY
FAMILY: RETROVIRIDAE
(SUBFAMILY)
Oncovirinae
GENUS
Alpharetrovirus
PROTOTYPE
ALV, RSV
(Avian type C)
Betaretrovirus
(type B)
(type D)
Gammaretrovirus
MMTV
MPMV, SMRV, SRV-1
MLV, FeLV, GALV
(type C)
Deltaretrovirus
(type C)
Lentivirinae
Spumavirinae
HTLV-1, HTLV-2, STLV, BLV
HTLV-3, HTLV-4
Lentivirus
HIV-1, HIV-2, SIV, FIV
EIAV, CAEV, MVV
Spumavirus
HSRV, SFV, FeSFV, BFV
DISEASE
Lymphoma,
Sarcoma
Mammary Carcinoma,
Lymphoma
None; SAIDS
Leukemia,
Lymphoma
Leukemia, Lymphoma
AIDS, Neurol. Dis.
Pneumonia
None known
RETROVIRUS MORPHOLOGY
RT
RETROVIRUS CATION
ONCOVIRUS
SIZE
(nm)
INTRACYTOPLASMIC
A-TYPE PARTICLE
BUDDING
MORPHOLOGY
( ICA )
MATURE VIRION
CORE
80-100
Mn+2
-
Crescent NC
Icosahedral
Type B
Mg+2
ICA budding
Icosahedral
Type D
Mg+2
+
+
-
Crescent NC
Alpha/Gamma
Type C
Betaretrovirus
Deltaretrovirus Mg+2
Type C
ICA budding
LENTIVIRUS
Mg+2
100-120
-
Crescent NC
SPUMAVIRUS
Mg+2
100-140
-
ICA-like budding
Cylindrical/Conical
Icosahedral
Cylindrical/Conical
Icosahedral
LENTIVIRUS
ONCOVIRUS
SPUMAVIRUS
FIV
FeLV
FeSFV
HIV
SIV
MVV
Budding
VIRUS
LENTIVIRUS:
BUDDING
VIRUS
MATURE
VIRUS
Yamamoto JK, et al. AJVR 49:1246-1258, 1988
MATURE
VIRUS
LENTIVIRINAE
Caprine Arthritis-Encephalitis Virus
(1980) arthritis, encephalitis
Maedi-Visna Virus
(1953) pneumonia, encephalitis
Bovine Immunodeficiency Virus
(1972) lymphocytosis
Feline Immunodeficiency Virus
(1987) FAIDS: encephalitis, anemia
Human Immunodeficiency Virus
(1983) AIDS: arthritis, encephalitis,
anemia
Simian Immunodeficiency Virus
(1985) SAIDS: encephalitis, anemia
Equine Infectious Anemia Virus
(1905) fever, anemia
HTLV & HIV VIROLOGY
HTLV
HIV
MORPHOLOGY
Oncovirus (deltaretrov.)/ no A particle
Lentivirus
GENOME SIZE (kb)
8.5 (lacks accessory genes)
9.8
GENETIC VARIATION
90-99% w/in geographic location
Low between dif. Isolates
Moderately high w/ in person (5%)
High in & between subtypes
VIRAL RECEPTOR
GLUT1 (glucose transporter)
on many species (xenotropic)
CD4; CXCR4 (T cell); CCR5 (Mac)
CELL TROPISM
T cells ( CD4 / HTLV-1 )
T cells ( CD8 / HTLV-2 )
B cells; Many cell types
T cells ( CD4 )
Macrophages, Glial cells,
& Endothelial cells
TRANSFORMATION
T cells (Tax – viral promoter)
None
VIRAL REPLICATION
Very low to negligible titers
High titers
TRANSMISSION
Cell-associated; Milk; Sex (male to female)
Blood transfusion (IV drug user, IDU)
Body fluids; Cells; Blood;
Milk; Sex; IDU.
PATHOGENESIS
VERY SLOW (>20 years)
CD4 / CD8 normal or
CD4 high w/ malignancy
HIV-2 slow; HIV-1: Pediatric - acute
Adult AIDS - acute to slow
CD4 / CD8 & CD4 decrease
DISEASES
Adult T-cell Leukemia (CD4)-HTLV-1
CNS diseases; AIDS
Tropical Spastic Paraparesis- HTLV-1
Kaposi’s sarcoma
T-cell variant hairy-cell leukemia (CD8)HTLV-2
ACUTE ATL
Adult T-cell Leukemia
Skin lesions due to
infiltration of leukemia
cells
(skin and/or lung infiltration)
Polylobulated nucleus of two CD4+ T leukemic cells
GLOBAL DISTRIBUTION OF HTLV INFECTIONS
STLV-1
STLV-2
STLV-3
?
Cameroon
HTLV-3
(2005; 4 cases)
HTLV-4
(2005; 1 case)
(Discovered 1980; 15-20M cases in 2009)
(Discovered 1982)
HTLV-1
HTLV-2
HTLV-3
HTLV-4
33 MILLION LIVING WITH HIV-1 IN 2007
Haiti 1966
Subtype B
HIV origin 1884-1924
Origin of Group M:
Kinsasha 1959
(1959, subtype D; 1960, subtype A)
Brazzaville 1983
Figure 1.
RETROVIRUS STRUCTURE
VIRAL CORE &
CORE ASSOC. PROTEINS
Matrix
Protein Capsid
MA
CA
VIRAL ENZYMES
Protease
Nucleoprotein
PR
Reverse
Transcriptase
RT
Integrase
IN
NC p6
ACCESSORY
PROTEINS (HIV)
Vif
Vpr
Nef
Cellular
Plasma Membrane
SU
Surface
Envelope
TM
Transmembrane
VIRAL ENVELOPE PROTEINS
Viral RNA Genome
HIV, SIV, FIV
TAR
5’ CAP
y
PB
SD
gag-pol
FSR
gag
pro
RRE
SA
SA
pol
Viral mRNA
PAS
env
AAA 3’
PB = Primer Binding site
FSR = Frame Shift Region
SD = Splice Donor site
SA = Splice Acceptor site
REGULATORY / ACCESSORY PROTEINS (genes)
Tat - binds to TAR (trans-activating response element) on viral transcripts to enhance transcribing
polymerase activity.
Rev - binds to RRE (Rev response element) on viral transcripts to export unspliced mRNA out of
nucleus. Rev rich in NES (nuclear export signal) which allows it to shuttle between nucleus
& cytoplasm via interaction with nucleoporin-like protein (hRip/Rab) on nuclear pore.
Nef - 1) Down regulate CD4 & MHC-I which affects immune response
2) Facilitate routing of CD4 from cell surface & golgi aparatus to lysosome; causes increase in Env
incorporation into virion & promote particle release.
3) Enhance viral infectivity by binding to Src-family proteins & regulating their tyrosine kinase activities.
Vif
- 1) Functions before or during viral DNA synthesis hence affect viral production (block APOBEC).
2) Production of highly infectious mature virions by affecting assembly and/or maturation.
Vpr - 1) Mediate transport of nucleoprotein complexes (RT, IN, MA, vRNA, partially reverse-transcribed DNA)
to nucleus.
2) Has NLS that directs transport even in absence of mitotic nuclear envelop breakdown & therefore
important for nuclear localization in nondividing cells (macrophages)
3) Cause G2 cell cycle arrests & kill T cells by apoptosis.
4) Influence mutation rates during viral DNA synthesis
Vpu - 1) Down regulate CD4 & MHC-1 expression & affects immune response
2) Increase virion release
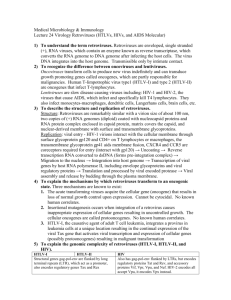
COMPARISON OF RETROVIRAL GENOMES
( kilobases )
0
1
2
3
4
5
6
7
8
9
10
RETROVIRUS REPLICATION CYCLE
1.
Virus attachment to specific cell-surface receptor.
2.
Viral core penetration into cell.
3.
Reverse transcription within core structure (RNA to DNA).
4.
Viral DNA transit into nucleus.
5.
Viral DNA integration into cell DNA to become provirus.
6.
Viral RNA synthesis by cell RNA polymerase.
7.
Processing viral transcripts to genome and mRNAs.
8.
Viral protein synthesis.
9.
Assembly and budding of virions.
10.
Processing of capsid proteins.
Reverse Transcriptase
Heterodimer - p66 & p51
VIRAL DNA SYNTHESIS
( Stage 1 - Cell Cytoplasm )
VIRAL DNA SYNTHESIS
( Stage 2 - Cell Nucleus )
Vpr –( RT / IN / MA / vDNA )
Vpr Transport to Nucleus
Stage 2
Cell Nucleus
ACTIVATION SIGNAL
INTEGRASE
0
Tat
1
2
3
4
5
6
7
8
9
10
0
1
2
3
4
5
in
6
7
8
9
10
Vpr
Viral mRNA
transit to
cytoplasm
Rev
Enhance
release of
virion
Nef & Vpu
A CURE FOR HIV-1 USING
HIGHLY ACTIVE ANTIRETROVIRAL THERAPY ( HAART )
IN COMBINATION WITH
TOTAL BODY IRRADIATION ( TBI ) AND
PERIPHERAL-BLOOD STEM - CELL TRANSPLANTATION ( PSCT )
WITH HOMOZYGOUS CCR5-Δ32 /Δ32 STEM CELLS
THE NEW
ENGLAND JOURNAL o f MEDICINE
692 N ENGL J MED 360;7 NEJM.ORG FEBRUARY 12, 2009
BRIEF REPORT
Long-Term Control of HIV by CCR5 Delta32/
Delta32 Stem-Cell Transplantation
Gero Hütter, M.D., Daniel Nowak, M.D., Maximilian Mossner, B.S.,
Susanne Ganepola, M.D., Arne Müßig, M.D., Kristina Allers, Ph.D.,
Thomas Schneider, M.D., Ph.D., Jörg Hofmann, Ph.D., Claudia Kücherer, M.D.,
Olga Blau, M.D., Igor W. Blau, M.D., Wolf K. Hofmann, M.D.,
and Eckhard Thiel, M.D.
Prepublished online Dec 8, 2010;
doi:10.1182/blood-2010-09-309591
Evidence for the cure of HIV infection by CCR5{Delta}32/{Delta}32 stem cell
transplantation
Kristina Allers, Gero Hütter, Jörg Hofmann, Christoph Loddenkemper, Kathrin Rieger, Eckhard Thiel and
Thomas Schneider
QUESTIONS ( RETROVIROLOGY ) :
1)
Name the three Retroviridae subfamilies and their major disease manifestations.
2)
What is a provirus?
3)
Can a retrovirus replicate in a cell using cellular reverse transcriptase (RT) and
without the use of viral RT? Describe how RT functions in HIV replication?
4)
Is immune activation important in HIV replication?
5)
What are the regulatory genes and their function(s)?
NEXT SECTION IS ON :
HIV-1 THERAPY
HIV-1 AND AIDS
HIV THERAPY
HIV EPIDEMIOLOGY & PHYLOGENY
HIV PATHOGENESIS & HIV VACCINE
HIV REPLICATION CYCLE
STAGES TARGETED FOR THERAPY
THERAPY
1)
Anti-gp120 Abs
Anti-gp41 Abs
Anti-CD4 Abs
Soluble CD4
1A)
1B)
CCR5 Inhibitor
Fusion Inhibitor
3)
AZT, ddI, 3TC, dT4
5)
Integrase Inhibitor
8A)
Protease Inhibitors
9)
Interferon-Alpha
1 Virus adsorption to CD4 receptor
Fusion Inhibitor
1B HIV gp41 fuses
viral & cellular membranes
CCR5 Inhibitor
1A CD4 binds to gp120
then CCR5 binds to gp120
CD4 CCR5
Nucleoside Analogs
Non-nucleoside RT
Inhibitors
Integrase Inhibitor
Protease Inhibitors
9-10) DIBA
(Zinc-finger Inhibitor)
FDA APPROVED ANTI-HIV-1 DRUGS
FDA APPROVED ANTI-HIV-1 DRUGS
GENERIC NAME/
NOMENCLATURE
TRADE NAME
GENERIC NAME/
NOMENCLATURE
FDA
APPROVAL
(Company)
NUCLEOSIDE ANALOGS ( NRTI ) :
Retrovir / AZT
Retrovir
Zidovudine
/ ZDV / AZT
Hivid
June 19, 1992
( Hoffmann-La Roche)
Zerit
June 24, 1994
(Bristol-Myers Squibb)
Lamivudine / 3TC
Epivir
Nov. 17, 1995
(Glaxo Wellcome)
Ziagen
Abacavir / ABC
Dec. 17, 1998
(Glaxo SmithKline)
Oct. 26, 2001
Viread
Emtricitabine / FTC
Emtriva
July 2, 2003
(Gilead Sciences)
NON-NUCLEOSIDE RT INHIBITORS ( NNRTI ) :
X Nevirapine / NVP
Viramune
June 24, 1996
(Roxane Laboratories)
X Delavirdine / DLV
Rescriptor
April 4, 1997
(Pharmacia & Upjohn)
X Efavirenz / EFV
Sustiva
Intelence
Jan. 18, 2008
(Tibotec Therapuetics, J&J)
Ritonavir/ ABT-538/ RTV
Indinavir / IDV
X
Mar. 1, 1996
Crixivan
Mar. 13, 1996
(Merck & Co.)
Nelfinavir / NFV
Viracept
Mar. 14, 1997
(Agouron Pharmaceuticals)
Х Saquinavir / SQV-(SGC)
Fortovase
Nov. 7, 1997
(Roche Pharmaceuticals)
XХ Amprenavir / APV / AMP
Agenerase
April 15, 1999
(Glaxo SmithKline)
Kaletra
Sept. 15, 2000
(Abbott Laboratories)
Reyataz
June 20, 2003
(Bristol-Myers Squibb)
Oct. 20, 2003
Lexiva
Fosamprenavir / FPV
(Glaxo SmithKline)
X Tipranavir / TPV
Aptivus
June 22, 2005
(Boehringer Ingelheim)
Darunavir / DRV
Prezista
June 23, 2006
(Tibotec Therapeutics, J&J)
FUSION INHIBITOR:
Enfuvirtide / T20
Fuzeon
(Roche + Trimeris)
Mar. 13, 2003
Selzentry
(Pfizer Inc.)
Aug. 6, 2007
Isentress
(Merck & Co.)
Oct. 12, 2007
CCR5 INHIBITOR:
Maraviroc / MVC
HIV-2
Effective
Low effect
No effect
Norvir
(Abbott Laboratories)
X Atazanavir / ATV / ATZ
Sept. 17, 1998
(DuPont Pharm. Co., Bristol-Myers Squibb)
Etravirine / ETR
Dec. 6, 1995
Ritonavir+Lopinavir
/ RTV+LPV
Atripla ( July 12, 2006 )
(Gilead Sciences)
Truvada
(Aug. 2, 2004)
Tenofovir / TDF / PMPA
Trizivir ( Nov. 14, 2000 )
Oct. 9, 1991
(Bristol-Myers Squibb)
Stavudine / d4T
PROTEASE INHIBITORS ( PI ) :
Saquinavir / SQV-(HGC)
Inverase
(Roche Pharmaceuticals)
Combinavir
Epizicom
(Sept. 27, 1997) (Aug. 2, 2004)
Videx
Х Zalcitabine / ddC
(Company)
FDA
APPROVAL
Mar. 19, 1987
(Glaxo Wellcome)
Didanosine / ddI
TRADE NAME
INTEGRASE INHIBTOR:
Raltegravir / RAL / MK-0518
DURATION OF DRUG EFFICACY:
DEVELOPMENT OF RESISTANT MUTANTS
Time for resistant strains or mutants (also cross-resistant strains) to develop:
NNRTIs
<
days - weeks
<
PIs
2-3 months
NRTIs
6 - 12 months
Cross-resistance occurs with many drugs that have similar mechanism(s)
of drug action (i.e., within drug class).
Highest frequency
of cross-resistance
NNRTIs
Lowest frequency
of cross-resistance
>
PIs
>
NRTIs
( d4T )
( 3TC )
( PMPA )
( ABC )
deoxyguanosine
INHIBITION OF
HIV Reverse Transcriptase
Heterodimer - p66 & p51
Functional Activities & Sites
Polymerase – RdDp & DdDp
RNase H
Nevirapine
(NNRTI)
AZT
( NRTI )
HIV PROTEASE
INHIBITORS
RT
IN
NEW ANTIRETROVIRAL DRUGS
FUNCTION AT CELL SURFACE
F F
H3C
NH
N
36 amino acid peptide
C204 H301 O64
N
N
N
H3C
CH3
Enfuvirtide or Fuzeon or T-20
( Fusion Inhibitor )
Maraviroc or Selzentry
( CCR5 Inhibitor )
gp41
Prevents viral gp41
from fusing the
viral membrane to
the cell plasma membrane
CD4
CCR5
Blocks
Blocks CCR5
CCR5 co-receptor
co-receptor
binding
binding to
to gp120
gp120
DRUG STRUCTURES
& USA PRICING
in 2007
NRTI PMPA C19H30N5O10P· C4H4O4
($5,733 / year)
PI Ritonavir C37H48N6O5S2
($13,128 / year)
Diester hydrolysis in
intestine lumin & plasma
NRTI 3TC C8H11N3O3S
($3,801 / year)
Tenofovir
diphosphate PMPAPP in cell
CH3CO-Tyr-Thr-Ser-Leu-Ile-His-Ser-Leu-Ile-Glu-Glu-Ser-Gln-Asn-Gln-Gln-Glu-Lys
-Asn-Glu-Gln-Glu-Leu-Leu-Glu-Leu-Asp-Lys-Trp-Ala-Ser-Leu-Trp-Asn-Trp-Phe-NH2
Fusion-I Enfuvirtide C204H301N51O64
($23,919 / year) SC injection
NNRTI Nevarapine
C15H14N4O
($4,796 / year)
CCR5-I Maraviroc C29H41F2N5O
($10,585 / year)
INI Raltegravir C20H20FKN6O5
($9,850 / year)
PARAMETERS FOR ASSESSING THERAPEUTIC EFFICACY
GOALS OF HIV THERAPY
CLINICAL OUTCOME:
Delay in symptoms ( i.e., delay in AIDS manifestations )
Extended survival time - Reduction of HIV-related morbidity & mortality
IMMUNOLOGIC OUTCOME:
Preserve & restore immune functions ( increase CD4 counts & CD4 / CD8)
X Enhancement of protective immune functions
VIROLOGIC OUTCOME:
Decrease viral load for a long duration
PBMC viral load ( HIV RNA, proviral DNA )
Plasma viral load ( HIV RNA by PCR; HIV p24 level )
Delay in viral evolution ( i.e., mutant emergence ) Important in determining when to switch therapeutic regimen
QUALITY OF LIFE - SAFETY & TOLERANCE:
Improve quality of life - minimal-to-no drug toxicity and clinical AIDS
Terotogenic effect (especially multiple drug combination)
MAJOR REASONS FOR TREATMENT FAILURE
IN HIV PATIENTS
RESISTANCE TO DRUG ( 70% ):
Cause of high mutation is due to the fact that the REVERSE TRANSCRIPTASE
is error-prone (i.e., makes a lot of mistakes & these mistakes lead to new mutants).
LOW DRUG CONCENTRATIONS AT THE VIRAL REPLICATION SITE (>25%):
1) Low Drug Potency due to Patient Factors:
a) Noncompliance
b) Interpatient variability
2) Low Drug Potency due to Pharmacologic Factors:
a) Drug-drug interactions
b) Inefficient drug absorption
c) Accelerated metabolism
PROGRESSIVE DECLINE OF THE IMMUNE SYSTEM:
CD4+ T cell loss
CD8+ T cell loss
Other immune cell loss
Immune Network Destroyed
QUESTIONS ( HIV THERAPY ) :
1) What is HAART or ART?
2) An unsuccessful treatment with a protease inhibitor will often cause
the subsequent therapy with another protease inhibitor to be less
effective. Why?
Would a therapy with nucleoside analogs be more successful
in this patient?
HIV-1 AND AIDS
HIV EPIDEMIOLOGY & PHYLOGENY
HIV PATHOGENESIS
ANTIRETROVIRAL (ARV) TREATMENT COVERAGE AS OF DECEMBER 2007
Estimated no. of
people receiving
ARV therapy
Estimated no. of
people needing
ARV therapy
ARV therapy
coverage
2.1 M
7M
30%
Latin America & Caribbean
390,000
630,000
62%
East, South & SE Asia
420,000
1.7 M
25%
54,000
320,000
17%
7,000
100,000
7%
2.9 M
9.7 M
31%
Geographical Region
Sub-Saharan Africa
Europe, Central Asia
Middle east, North Africa
Total
HAART / TBI / PSCT WITH CCR5-Δ32/Δ32 STEM CELLS
AS A CURE FOR HIV-1 ?
HIV-1+ MAN with Acute Myeloid Leukemia
(AML) (40 years of age; 415 CD4+ T cells):
HAART
Allogeneic Stem Cells - important for AML
CCR5-deletion
Tissue-matched
Chemo-ablation (4X)
TBI (low dose, 1X)
HAART until few weeks post-SCT
600mg/d Efavirenz (EFV; NNRTI)
200mg/d Emtricitabine (ETC; NRTI)
300mg/d Tonofovir (PMPA; NRTI)
Anti-rejection drugs
1st: rabbit anti-thymocyte globulin
1st & 2nd: cyclosporine
1st & 2nd: mycophenolate mofetil
PSCT ( 2.3x106
11mo
No HIV-1 RNA
in blood & BM
HAART CHEMO-ABLATION and/or TBI PSCT
Control or treat HIV-1 infection
Stem cells from HLA-matched subject
Stem cells with homozygous CCR5 deletion (Δ32bp)
85-90% of HIV-1 uses CCR5 coreceptor
10-15% of HIV-1 uses CXCR4 coreceptor
1% of European population has CCR5-Δ32/ Δ32
AML relapse
HIV-1 DNA+ in blood
Chemo-ablation (1X)
TBI (200 cGy, 1X)
2.9% of his HIV-1 species was X4- or dual-tropic
Treat leukemia w/o increasing HIV-1 infection
SC / kg )
3.5 YEARS
PSCT ( 2.1x106
SC / kg )
20mo - free of AML
No HIV-1 RNA in blood
and tissues
Proviral DNA+ in tissues
HIV-1 CURE ???????
WHO GLOBAL DISTRIBUTION OF HIV INFECTION
Adults & Children Estimated to be Living
2008)
( Estimation as of End of Year 2005
EASTERN EUROPE & CENTRAL ASIA
1.4 million
1.5 million
WESTERN & CENTRAL
EUROPE
850,000
GLOBAL TOTAL ALIVE
33.4 million
NORTH AFRICA
& MIDDLE EAST
310,000
510,000
EAST ASIA
850,000
SOUTHEAST &
SOUTH ASIA
3.8 million
CARIBBEAN
240,000
300,000
LATIN AMERICA
1.8 million
2.0
million
SUB-SAHARAN AFRICA
22.4 million
AUSTRAL ASIA
59,000
WHO GLOBAL DISTRIBUTION OF HIV INFECTION
Estimated Adults & Child Deaths
( Estimation as of End of Year 2008
2005 )
EASTERN EUROPE & CENTRAL ASIA
62,000
87,000
25,000
WESTERN & CENTRAL
EUROPE
13,000
GLOBAL TOTAL DEATHS
2.0 million / Year ( 5,495 DEATH / DAY )
NORTH AFRICA
& MIDDLE EAST
58,000
20,000
EAST ASIA
41,000
59,000
SOUTHEAST &
SOUTH ASIA
480,0000
270,000
CARIBBEAN
24,000
12,000
LATIN AMERICA
66,000
77,000
SUB-SAHARAN AFRICA
2.4
1.4 million
million
AUSTRAL ASIA
3,600
2,000
WHO GLOBAL DISTRIBUTION OF HIV INFECTION
Estimated Adults & Children Newly Infected
( Estimation as of End of Year 2005
2008 )
EASTERN EUROPE & CENTRAL ASIA
270,000
110,000
55,000
WESTERN & CENTRAL
EUROPE
30,000
GLOBAL TOTAL NEWLY INFECTED
2.7 million / Year ( 7,418 NEWLY INFECTED /EAST
DAY
ASIA )
140,000
East Asia
75,000
NORTH AFRICA
& MIDDLE EAST
67,000
35,000
SOUTHEAST &
SOUTH ASIA
990,0000
280,000
CARIBBEAN
30,000
20,000
LATIN AMERICA
200,000
170,000
SUB-SAHARAN AFRICA
3.2 million
million
1.9
AUSTRAL ASIA
8,200
3,900
Reported AIDS Cases ( 2007 )
State
1. New York
2. California
3. Florida
4. Texas
5. New Jersey
“Top 5 Total”
TOTAL U.S.
Cumulative*
# of Cases
% of Total
181,461
18 %
148,949
15 %
109,524
11 %
72,828
7%
50,694
5%
563,456
998,255
56 %
100%
Reported 2007
Rate/100,000**
24.9 (2nd)
13.5 (11th)
21.7 (4th)
12.4 (14th)
13.4 (12th)
.
12.4
*Cumulative data are through 2007.
Lowest cumulative number of cases in North Dakota with 153.
**Reported AIDS cases in annual rates (per 100,000 population) in 2007:
(1) District of Columbia 148.1; (3) Maryland 24.8; (5) Louisiana 20.5;
(6) Delaware 19.8; (7) Georgia 19.7; (8) South Carolina 16.8; (9) Connecticut 15.1
Lowest rate in Vermont with 1.0.
Persons Newly Diagnosed with HIV-1
U.S.A. in 2007 and Florida in 2008*
U.S.
Subgroup
N=101,614
Male
76%
Female
24%
White
35%
Black
44%
Hispanic
19%
Other
2%
MSM
44%
IDU
10%
MSM/IDU
4%
Heterosexual
17%
Other
25%
Florida
N=4,613
68%
32%
21%
57%
20%
2%
40%
5%
3%
34%
18%
*Source: CDC, HIV/AIDS Surveillance Report, 2007; Estimate for Florida.
M:F ratio:
U.S.A., 3.2:1
Fla., 2.1:1
PERSONS TESTED NEWLY POSITIVE (PTP)
FOR HIV IN 2008
90,968 Estimated Living HIV/AIDS Cases in Florida (2008)
or 11% of Total USA Cases
( 822,055 Estimated Living HIV/AIDS Cases in USA, 2008 )
54
2
1
5
Florida State Univ.
12
2
2
19
N = 4,613
Univ. of Florida
7
32
43
0
0
0
1
2
1
1
4
4
1
4
0
0
1
287
4
8
8
4
78
14
14
3
0
Univ. of Central Florida
45
47
PTP Cases
0 to 10
11 to 50
51 to 100
> 101
13
5
8
31
16
Univ. of South Florida
H. Lee Moffitt Cancer Center
423
29
161
375
32
36
71
Saint Lucie
13
18
2
1
6
19
2
67
8
0
3
460
42
HIV/AIDS has spread out from 6 major
urban epicenters into smaller cities,
suburban and rural areas.
12
31
698
9
9
1312
HIV ORIGIN LINKED TO SIV
SIVcolCGU1
HIV-1 Group O
SIVCPZ
HIV-1 Group N
HIV-1 Group M
SIVSYK173
SIVMND2
SIVRCMNg411
SIVGSN99CM166
HIV-2 Group A
SIVHOEST
HIV-2 Group F
HIV-2 Group G
HIV-2 Group B
SIVSUN
SIVMND1
SIVAGM
SIVSMM
HIV-1
GROUPS
&
LBV271
BUK3A
92RU131 HIV-1 SUBTYPES
V1536
ANT70
G
G98
H
VAU
CA13
92UG975
V1557
MPV5180
CAR4067
SE7022
SE7887
CARSAS
A
J
V1686
CA9
KENYA
92UG0378
O
92W0205
M
U455
K
92BR025
DJ373A
UC268A2
C
93MW965
CPZgab
CAR4026
2UG021
SE364A
NDK
MN
Z2Z6
D
YBF-30
ELI
JRFL
ALA1
B
SF2 NY5
NL34
YBF-160
N
SIV
CPZant
93BR029
BZ163A
BZ126A
F
93BR020
Former subtypes E (Ae) and I (A, G, H, K) were found to be subtype recombinants.
M = Major Group
N = Non-M, Non-O Group
O = Outlier Group
GLOBAL DISTRIBUTION OF HIV-1 SUBTYPES
90% of
Global
Infections
B, a, Ab, c, d, g, h
B
HIV-2
B, a, c, d, f, o
HIV-2
B, a, d, o
B
B, C
B, c, Ae, Bc
B
C
A
B
HIV-2
A, O, Ag, d, g, h
f, g, h, j, k
b
recombinants
A, D, Ae
B
B
B
B
B, f, Bf, c
B, Ae
HIV-2
C, a, b, Ae
B, Ae
C, Ae
C, Ae, b
CC
Ae,b
C, a, d
C
As much as 4 subtype recombinants have been observe
in a single isolate ( former subtype I, A/G/H/K ).
10-35% of circulating forms are recombinants.
Recombinations are more common in gag & env.
B
B
B
C
A
Ae
Ag
d
HIV-1 TRANSMISSION
(76% ♂ & 24% ♀, 101,614 cases in USA 2007)
SEXUAL CONTACT
HIV enters via mucosal linings (61,461 cases / yr, 60%, USA 2007).
( vagina, vulva, penis, rectum, rarely via mouth )
Mucosal dendritic cells (MDC) & macrophages are first to be
infected. Infected MDC & replicated HIV travel to germinal centers
of the lymphoid organs where FDCs & T cells become exposed.
RECEIPT OF INFECTED BLOOD, BLOOD PRODUCTS, OR TISSUES
Contaminated needles shared by IV drug users (10,430/ yr, 10%, USA 2007).
Use of infected blood, blood products, or tissues (374 / yr, 0.4%, USA 2007).
40 cases in 14 million blood units per year in USA.
Since 1989, 4 cases infected with HIV-antibody negative blood.
New HIV-p24 capture test detects HIV-1 earlier by 1 week.
MOTHER-TO-CHILD TRANSMISSION (610 cases / yr, 0.6%, USA 2007)
75-93% of cases occur in utero or during childbirth.
Transmission also by nursing infected breast milk. Breast feeding
strongly not recommended for HIV-positive mothers.
ART during pregnancy decreases infection of the fetus and newborns.
SEXUAL TRANSMISSION
HETEROSEXUAL TRANSMISSION:
2X - 5X Risk: male-to-female >> female-to-male
HOMOSEXUAL TRANSMISSION:
Receptive Partner >> Active Partner
[ Infected insertive partner - to - Uninfected receptive partner > >
Uninfected insertive partner - to - Infected receptive partner ]
HIV TRANSMISSION RATE POST-SINGLE EXPOSURE vs
% TOTAL WITH CORRESPONDING EXPOSURE ( GLOBAL vs USA )
EXPOSURE TYPE
LIKELIHOOD OF INFECTION
GLOBAL
AFTER SINGLE EXPOSURE (%) TOTAL (%)*
USA
TOTAL (%)*
Sexual Transmission
Receptive vaginal
MSM
MSM + IDU
0.01 - 1.0
0.01 - 0.32
1.0
NA
70 - 80
60 - 70
5 - 10
NA
78
19
46
5
Contaminated Needle
( IV drug users, IDU )
0.5 - 1.0
5 - 10
18
12 - 50
12
5 - 10
NA
1.1
NA
>90
3-5
1.2**
0.1 - 1.0
<0.01
<0.005
Maternal Transmission
Pregnancy/delivery
Breast milk
(Continuous breast feeding)
Blood (Product) Transfusion
Health Care Workers
(needlestick, etc.)
* Global cumulative data were before 2000. USA cumulative data were through end of 2007.
** USA data include infection from contaminated blood, blood products, and tissues.
HIV VACCINES IN CLINICAL TRIALS
Preclinical Testing –
In vitro & In vivo animal trials
Clinical Phase I
Clinical Phase II
Clinical Phase III
Dose-escalation, safety, & toxicity tests
Expanded safety & dose optimization & some immunogenicity
Efficacy trials
-
VACCINE(S)
rgp120
Adenovirus 5-gag/pol/nef
ALVAC (vCP gag/pol/env); rgp120
HIV SUBTYPE
(other / env)
SPONSOR(S)
CLINICAL
PHASE LOCATION OF TRIAL(S)
BB
VaxGen
III
USA
B
Merck, HVTN
IIb
USA, Canada, Peru, Haiti, Porto Rico,
Dominican Republic, Australia
III
Thailand
B / Be
Aventis Pasteur, VaxGen
Lipopeptide antigens (Gag, Pol, Nef)
B
ANRS
II
France
AAV-HIV (gag/PR/ΔRT)
C
IAVI, Targeted Genetics
II
South Africa, Uganda, Zambia
DNA-HIV (B gag/pol/nef, ABC env);
ADV5-HIV (B gag/pol, ABC env)
B / ABC
HVTN, Vical
II
UNSW
I-II
Thailand
DNA-HIV (AB gag, B RT/rev, ABC env) AB / ABCe
MUCHS, SMI, USMHRP,
I-II
MVA-HIV (A gag, B pol, E env)
Karolinska Institute, Vecura
Tanzania
Thirty other vaccine trials
USA, France, Thailand, Brazil, Haiti, etc
DNA-HIV; Fowlpox (gag/po/tat/rev/env) A / Ae
ABCe
Many Companies
I
USA, Brazil, South Africa (Haiti, Jamaica)
VaxGen (Brisbane,CA); Aventis Pasteur (Lyon, France); HVTN (HIV Vaccine Trials Network, DAIDS); ANRS (National Agency for
AIDS Research, France); IAVI (Intl AIDS Vaccine Initiative); UNSW (University of New South Wales); MUCHS (Muhimbili University
College of Health Sciences); SML (Swedish Institute of Infectious Dis Control); USMHRP (US Military HIV Research Program);
ALVAC (canarypox vector); ADV5 (Adenovirus-5 vector); Lipopeptide antigens (LP5, LP6); AAV (Adeno-associated virus vector);
DNA (plasmid DNA vaccine); MVA (modified vaccinia Ankara vector)
FAILED TRIALS
FAILED TRIALS
HIV VACCINE CANDIDATES IN CLINICAL TRIAL
WHY IS HIV-1 VACCINE DIFFICULT TO DEVELOP ?
1) Multiple subtypes (error-prone RT)
2) Many recombinants (superinfection)
3) Multiple transmission routes
Mucosal - sexual transmission
IV IVD (IV drug users); infected blood transfusion
Utero / birth canal / colostrum-milk - vertical transmission
4) HIV-1 proteins needed for vaccine immungen?
5) Infects immune cells
CD4+ T cells
Macrophages
Stem cells ?
6) Infects glial cells, microglial cells, & astrocytes in CNS
7) Need many anti-HIV immune mechanisms for protection
IL-2 production & polyfunctional responses
QUESTION ( HIV EPIDEMIOLOGY & PHYLOGENY ) :
1)
Which continent will be a major source of all HIV-1 subtypes?
2)
What are the origins of HIV-1 and HIV-2?
3)
Are the origins of HIV-1 and HIV-2 similar to HITLV-1, -2, -3 and -4?
4)
Why is it so difficult to develop an HIV-1 vaccine? (State at least 3 reasons)
5)
What is the most effective mode of HIV transmission?