Sex Offender Specific
Treatment
Howard Levine Ph.D., LCP
Coles County Mental Health Center
Mattoon, IL
hlevine@ccmhc.org
1
Grateful Acknowledgements
• Center for Sex Offender Management
(www.csom.org) For their expertise and
excellent training curricula used here.
• Kurt Bumby, Center for Effective Public Policy
(www.cepp.com) Work on shame/guilt and other
excellent slides used in this presentation.
• Donya Adkerson, Alternatives Counseling, Glen
Carbon, IL, 62034, (618) 288-8085
(donya2@aol.com) For dedication to the field
and her slides on PGE use in treatment.
2
The Goal of Sex Offender –
Specific Treatment
• Community protection through effective
treatment and management of sex offenders in
order to REDUCE THE LIKILIHOOD OF
FURTURE VICTIMIZATION
• MISSION: NO MORE VICTIMS
3
Not All Sex Offenders Are The
Same
• Majority, but not all, offenses are committed by males
• Sex offenders can be adolescents or adults, male or
female, rich or not, white or not, straight or not, bright or
not
• Offenders differ in preference of victim and offense, risk
to offend, supervision and treatment needed
• Odds are the offender is family, friend or acquaintance to
the victim; but not always
• This presentation will focus on adult male sex
offenders; however, “special populations’ will be
discussed
4
Why do most sex offenders
sexually abuse?
• They want to (deliberate,no accident)
• They are interested (suspend empathy and fear
of consequences)
• The option is unappealing
• Victimization is not a self esteem issue
5
Sexual abuse is the last step in
a long effort to manipulate
• Victim, wife, partner and other adults
• Environment and family
The purpose of all this is to
Feed his imagination, strengthen justifications
Co-opt other adults, and victim(s)
Create reliable source for ongoing victimization
Decrease chances of being caught or stopped
Without external intervention most offenders
behavior escalates and continues
6
Why would a sex offender
change?
• When dire consequences are about to ensue
• Severe consequences have already been experienced
• He is reliably and credibly managed by a system
(natural and official) that can intervene with personally
relevant consequences before reoffense
• The offender has become disgusted with himself
(herself) AND views his deviance as a liability,
intolerable and ‘too expensive’
7
The Problem of Motivation
• It takes a different set of motivation (internal and
external) to make initial change and to sustain
that change
• Offenders are asked to change NOT to a
previously more healthy state BUT to a never
known/unfamiliar responsible state
• Big difference between compliance and change
• Natural and official systems can assist in
compliance. Change is up to the offender
8
Two Facets of Sex Offender
Management: Addressing both
External and Internal Controls
External Controls:
• Probation/Parole
Supervision
• Polygraph
Testing
• Registration/
Notification
• Use of
Community
Networks
Internal Controls—
External
Controls
Internal
Controls
The Four Domains of
Treatment:
• Sexual Interests
• Distorted
Attitudes
• Interpersonal
Functioning
• Behavior
Management
9
Differences From Other Forms of
Mental Health Treatment
•
•
•
•
•
•
•
•
Involuntary clients (need leverage)
Victim and community focus
Limited confidentiality
Treatment goals set by provider
Collaboration with others essential
Length of treatment
SPECIALITY AREA
NO TREATMENT BETTER THAN BAD TX
10
Characteristics of Sex
Offender Specific Treatment
•
•
•
•
•
•
•
•
Published standards
Containment approach
Specialized providers
Specialized assessments
Group treatment is treatment of choice
Individual treatment alone is rare exception
Cognitive behavioral therapy
Judicious use of medicines
11
Characteristics of Sex OffenderSpecific Treatment (cont)
•
•
•
•
•
Explicit, empirically-based model of change
Expected to reduce, never eliminate, recidivism
Social learning theory-based
Addresses criminogenic needs
Targets factors closely linked to sex offending
(criminogenic needs)
12
What Methods are Effective?
•
•
•
•
Cognitive-behavioral techniques
Adult learning theory methods
Positive reinforcement rather than punishment
Respectful confrontation
13
Treatment is Skills Oriented
• Skills to avoid sex offending
• Skills to engage in legitimate activities
• “Skills oriented treatment” includes:
•
•
•
•
•
•
Defining the skill
Identifying the usefulness of the skill
Modeling the skill
Practicing the skill
Giving feedback
Practicing the skill again
14
How Long Should Sex Offender
Treatment Last?
• Until recently, answers to this question were based only
on opinion—there is now research that addresses this
question
• Different offenders require different lengths of treatment
• Higher levels of denial, sexual deviancy, and risk require
longer, more intense treatment
15
How Long Should Supervision
of Sex Offenders Last?
• Different offenders require different lengths of
supervision based on risk determined through
specialized SOS evaluations
• Typically, active supervision should continue
long after active treatment
• Offenders should have the burden to establish
that they no longer require official supervision
• Longer is usually better
16
Monitoring and Quality Control of
Treatment are a Must
• Monitoring of:
•
•
•
•
•
Program activities
Clients
Containment team members
Containment team protocol
Natural supervisors
17
Treatment of the Denying Sex
Offender
• Denial is common among sex offenders
• But, admitting is vital to treatment
• Sex offenders who do not admit at some point can’t be
treated
• Therefore, treatment of denial is usually necessary to
make a client ready for sex offender treatment
18
Various Forms of Denial
•
•
•
•
•
•
•
Complete denial
Victim or other blaming
Denial of personal intent
Minimize extent or impact
Denial of planning
Denial of risk to reoffend
Family, community, system denial
19
Tools for Addressing Denial
• The polygraph—aimed at specific deceptions
• Physiological indications of deception
• Offenders often abandon denial
• Group treatment—targets four issues
•
•
•
•
Eliminating cognitive distortions
Facilitating engagement in treatment
Challenge offenders need to protect himself
Developing victim awareness
20
Treating Denial Focuses on its
Complexity
• Many purposes—why offenders are often in denial
• Multiple pressures to deny
• Denial in various phases of the offense (before, during,
and after)
21
Methods to Address Cognitive
Distortions
• Role play explaining to a victim all the information he
would need to give “informed consent” to sexual activity
22
Methods to Address Cognitive
Distortions (cont.)
• Articulating the thinking errors and cognitive distortions
offenders use to excuse their behavior
23
Increasing Victimization
Awareness
If sex offenders come to understand the harm they
cause, they will be more reluctant to commit future sex
offenses because they will find it more difficult to
disregard the consequences of their actions to their
victims and others
24
Methods to Address Victimization
Awareness
• Videotaped programs of sexual assault victims
• Visits by victims to the treatment group
25
Involving Sex Offenders Formerly
in Denial
• Often graduates of the “deniers’ group”
• Emphasis on the positive benefits of abandoning
denial
• “If I can do it, so can you”
26
The Culmination of Denier’s
Treatment
• The denier is at last permitted to discuss his own
offense—many are now quite willing to do so
• Some therapists report that 80% of deniers admit to the
offense when this approach is used
27
Bottom Line for Denial
• Admitting to a sex crime is a necessary
condition for successful treatment
• Offenders are to be given a specified period of
time to resolve their denial or risk removal from
treatment
• Denial is inversely related to treatment progress
and engagement in treatment
28
Sex Offender Treatment Goals
and Plans
• Accepting personal responsibility for a complete sexual
assault history
• Improving social, relationship, and assertiveness skills
• Appropriately managing anger
• Learning about the traumatic effects of victimization and
developing empathy
• Learning to separate anger and power from sexual
behavior
• Developing pro-social support networks
29
Sex Offender Treatment Goals
and Plans (cont.)
• Recognizing and changing cognitive distortions
• Identifying and modifying sexual arousal patterns
as appropriate via
• Behavioral interventions and/or
• Medication
• Developing and using interventions to interrupt the
offense cycle
• Adopting non-exploitative, responsible lifestyle
30
Conditions for Community
Supervision
• NO CONTACT WITH CHILDREN UNDER 18,
unless approved in advance and in writing by
supervising officer and provider
• No contact with victim(s)
• Not to date or befriend anyone who has children
or lives with children
• No access or loitering near places used
primarily by children
31
Conditions for Community
Supervision, continued
• No employment or volunteering that includes
contact with children
• Not possess or use any pornographic, sexually
oriented or stimulating material
• No internet use
• No alcohol or illegal drug use
• Residence pre-approved
• ‘Successfully complete’ all conditions of TX
32
Why No Contact Orders?
• Sex offenders are not purists, ‘victim profile’ is a
myth. Anyone weaker than an offender is a
potential victim.
• It is more a matter of opportunity than
preference.
• The “official record” is always wrong.
• Realigns incentive to cooperate in treatment.
• NO MORE VICTIMS. Community safety first.
33
‘Crossover effect’
Gene Abel et. al, (1983) landmark study on the
frequency and variety of sexual offending
behavior offenders commit. The 411 offenders in
the study on average over a 12 year period had
attempted 581 crimes, completed 533 crimes,
had 366 victims and completed an average of
44 crimes a year. These crimes included ‘hands
off’ offenses. 73%+ had two or more types of
deviant sexual interest.
34
More on crossover
Freeman-Longo, 1985
23 ‘rapists’
5090 incidents of sex offending
319 child molestations
178 rapes
30 ‘child molesters’
20667 offenses
5891 assaults on children
213 rapes on women
35
More still; this time with
polygraph
Colorado DOC, 1998
36 sex offenders on average
2 victims by official records
165 victims after first polygraph
185 victims after second polygraph
36
More yet
Ahlmeyer et. al., (2000)
Incarcerated sex offenders (average)
Official records
2 victims 5 offenses
After second polygraph
110 victims 318 offenses
37
Crossover; gender, age and
relationship
• Emerich and Dutton (1993, JSO) 55%
assaulted both boys and girls, 47%
acknowledged multiple victim relationships
• O’Connell (1998, community based ASO) 64%
of ‘rapists’ had assaulted a child, 59% of ‘incest
fathers’ admitted to victims outside of home.
38
Ahlmeyer, 1999. 143 ASO
Inmates, Polygraph and TX
• 89% crossover by relationship, gender or age
• 82% child molesters and 50% of rapists
crossover by age
• 58% ‘male victim ASO’ and 22% ‘female victim
ASO’ crossover by gender
• 86% of sample had victims in 2+ relationship
classes
39
Contact with children: high
risk behavior increased
• Davis et al, (1993) Of 143 incarcerated child
molesters studied only 3% of those not allowed
contact masturbated about a known child as
compared to 60% offenders permitted contact.
• 66-99% of incarcerated ASO with permission to
visit kids in DOC waiting room masturbated
about those kids. (Colorado DOC, 1999).
40
Sex offenders, even in
treatment, are dangerous
Tanner (1998) 128 ASO in first year of community
based treatment and supervision
31% had sexual contact with child
25% had unauthorized contact with a child
12% had forced someone to have sex
86% was participating in new high risk behavior
and/or new crimes
41
When to Increase Intensity of
Supervision
•
•
•
•
•
•
Offender in stress or crisis
Offender in high risk situation
Offender will have contact with potential victims
Offender shows high or increased denial
Offender works with internet
Active treatment or probation ending soon
42
The Four Domains of Treatment
• Sexual Interests
• Distorted Attitudes
• Interpersonal Functioning
• Behavior Management
43
Sexual Interests—The First Domain
of Treatment
• Deviant sexual arousal is sexual arousal to:
• Non-consenting partners
• Non-age-appropriate partners
• Acts that are abusive in nature
• For many sex offenders, a strong motivation to commit
sexual assaults is deviant sexual arousal
• Not all offenders have deviant sexual arousal
• AROUSAL DOES NOT EXPLAIN BEHAVIOR
44
For Offenders with Deviant
Sexual Arousal
If such arousal can be decreased, the likelihood of future
sex offending will be decreased
Treatment goals include:
• Reduce deviant sexual arousal while
increasing non-deviant sexual arousal
• Increase reactions to the offender’s deviant
behavior as non-offenders react—with
disinterest or revulsion
45
Behavioral Intervention to Reduce
Deviant Sexual Arousal
• Based on the idea that deviant sexual arousal is
“learned” behavior and can be unlearned
• Substitutes non-deviant thoughts for deviant thoughts
• Connects deviant thoughts with non-arousal
46
Types of Behavioral
Interventions
• Covert Sensitization
• Ammonia (aversive) conditioning
• Masturbatory reconditioning
47
Common Questions about
Behavioral Interventions
• Can offenders sabotage this?
• Who is this best suited for?
• Is this technique essential?
• Can this technique be used
exclusive of others?
• Yes—but they’re only
hurting themselves
• Offenders with significant
deviant sexual arousal
• No—but some
intervention must
address deviant sexual
arousal
• No
48
Goals of Covert Sensitization
• To reduce the attractiveness of sexual assault by having
the offender focus on the negative social consequences
he faces
• To have offenders explore all of the consequences of
their actions—in particular the negative consequences
which offenders so often refuse to recognize
49
Methods of Covert Sensitization
• Offenders identify the chain of thoughts that
lead them to offense behavior
• Offenders are taught to deliberately interject
vivid scenes of the negative consequences they
will face during that chain of thoughts
• Audiotape homework provides structured
practice sessions for this technique that can be
reviewed by the treatment provider
50
Goals of Ammonia (aversive)
Conditioning
• To reduce the strength of a deviant sexual
fantasy by association with unpleasant stimuli
• To reduce the strength of sexual response to the
deviant fantasy
• To facilitate offenders likelihood to
escape/terminate deviant sexual fantasy
51
Methods of Ammonia
(aversive) Conditioning
• Offenders identify and audiotape a powerful
deviant sexual fantasy.
• Offenders listen to their deviant fantasy and
deeply inhale ammonia at the first sign of sexual
stimulation.
• Last step is repeated frequently across days
until offender has eliminated arousal to fantasy.
52
More Methods of Ammonia
(aversive) Conditioning
• Homework sessions are reviewed by treatment
provider
• Offender eventually may carry small vial of
ammonia, or smelling salts, to use in real life
situations to escape/terminate deviant sexual
fantasy
• After inhaling the ammonia the offender is to
focus on non sexual thoughts and/or coping
skills
53
Goals of Masturbatory
Reconditioning
• Increase sexual arousal to appropriate sexual
fantasies with consensual adults
• Weaken arousal to deviant sexual fantasies by
association with boredom/non-arousal
54
Methods of Masturbatory
Reconditioning
• Offender verbalizes appropriate sexual fantasy
while masturbating to orgasm
• Immediately after orgasm to appropriate fantasy,
the offender continues to masturbate to
verbalized deviant sexual fantasy for 45 or more
minutes
• Audiotape homework is reviewed with treatment
provider
55
Pharmacological Interventions to
Address Deviant Sexual Arousal
There are two primary types of medications used in the
treatment of sex offenders:
• Selective Serotonin Reuptake Inhibitors
(SSRIs)
• Antiandrogens—used for what some call
“chemical castration”
56
Selective Serotonin Reuptake
Inhibitors
• Commonly prescribed for depression
• Reduce libido (sexual interest)
• They can also reduce aggression, decrease
deviant fantasies, empower people to better
manage their behavior, and reduce the intensity
of compulsive aspects of sexual offending
• Many physicians are knowledgeable of and
comfortable with prescribing such medications
57
Antiandrogen Medications
•
•
•
•
•
Drastically reduce testosterone
Reduce sex drive and the ability to have an erection
“Sexual appetite suppressants”
Examples include Provera and Lupron
Doctors reluctant to prescribe
58
Incidence of Side Effects of
Antiandrogen Medications
•
•
•
•
•
•
•
•
Decreased sperm count—100%
Increased body temperature—100%
Decreased sex drive—95%
Erectile dysfunction—95%
Decreased amount of ejaculate—95%
Weight gain—58%
Increased blood pressure—50%
Fatigue—30%
59
Side Effects of Antiandrogen
Medications (cont.)
•
•
•
•
•
Nervousness and/or depression—30%
Hot/cold flashes—29%
Headaches—20%
Nausea—14%
Gall bladder disease (sometimes necessitating
surgery)—13%
• Diabetes—4%
• Phlebitis (can lead to life-threatening pulmonary
emboli)—2%
60
Some Physicians are Reluctant to
Prescribe Antiandrogens
• They are not approved by the FDA for the treatment of
sex offenders
• It is outside of normal, clinical practice to prescribe to
men for reduction in sexual arousal
61
Methods of Administration and
Costs: Antiandrogens
• Depo-Provera
• Injected weekly
• $40 per week
• Provera
• Administered orally
• Depo-Lupron
• Injected monthly
• $400 per month
62
Is Medication Alone an Effective
Treatment Method?
• Medication that complements the cognitive-behavioral
center of treatment can be very helpful in facilitating
treatment—5 to 30% can benefit
• If our goal is to reduce recidivism, and medication will help
maintain an individual long enough to help him assimilate
the cognitive-behavioral response, it is irresponsible not to
use it
• Conversely, given the current body of evidence, it would
be irresponsible to only medicate and not include a
cognitive-behavioral treatment component
63
Distorted Attitudes—The Second
Domain of Treatment
• Purpose—to identify and alter offenders’
justifications for sex offending
• One approach is through cognitive restructuring
• By examining and exposing these thoughts,
justifications, rationalizations, and excuses, the
offender is challenged to understand his faulty
thinking and recognize its distorted, self-serving
nature
64
Cognitive Restructuring
Assists offenders to:
• Examine rationalizations, excuses, and
cognitive distortions
• Obtain candid feedback on these distortions
from others
• Heighten awareness of victimization issues
• Recognize the faultiness of his thinking
• Confound his ability to justify future offending
65
Thinking Errors of Sex
Offenders: SOBS
Offenders, in order to sexually abuse another
person, have changed their way of thinking so
that molesting another is not the same as others
believe. Offenders think in ways that have
made their sexual assault harmless, ‘OK’ or
deserved. SOBS is also used to justify the
behavior after the fact and support the offenders
self-centered approach to meeting his needs.
Offenders fight hard to justify and maintain their
SOBS.
66
Some Examples of SOBS
• Excuses; anything to avoid accepting personal
responsibility
• Blaming; excuses with a bad attitude
• Seeking sympathy; feel sorry for me
• Justifying; Yes, but…..
• Re-defining; shifting the focus of an issue to
avoid solving a problem
• Pet Me; notice me, cuddle me, applaud me
67
More Examples of SOBS
• Lying; complete, partial, phoniness
• Uniqueness; I am not like the others, this can’t
apply to me
• Minimizing; At least I didn’t…..
• Anger; to manipulate or distract others
• Victim stance; so others will rescue or forgive
him
• Helpless; I can’t … so don’t ask
• Arrogance and what is in it for me; bottom line
68
Methods of Cognitive Restructuring
• Examine role of distortions in non-sexual
situations
• Offenders anonymously relate the distortions
they have used in the past
• Role playing of victim, victim’s parent, long-time
friend of offender, probation/parole agent
• Debrief role plays
• The power of the group
69
Rationale for Victimization
Awareness/Empathy Training
• Most offenders victimize for selfish gratification
• If sex offenders learn about the true consequences of
their actions for victims, this confounds their ability to
discount the trauma that their actions create and
maintain their SOBS
• Many offenders do not have a generalized empathy
deficit
• However, most sex offenders have little empathy for
their victims
• If they learn, they will be less able to ignore/discount the
trauma their victims suffer
70
Goals of Victimization
Awareness/Empathy Training
• To understand the pervasive negative effects of
sexual assault on victims and others
• To know the consequences of his assaults (past
and future) on his victims and others
• To learn empathy skills, especially the ability to
empathize with his victims
• To make re-offending more complicated, less
enjoyable
71
Practice Implications
• SOS treatment programs should assess and
target the specific empathy deficits of each
offender
• Important to ensure that the offender does not
harbor hostility toward their victim before
providing training in victim awareness. Such
awareness is valuable only in a caring or benign
relationship
• Contraindicated for sociopath/psychopaths
72
Practice Implications (cont)
• Providers should carefully consider the value of
their existing empathy training program.
• Misdirected interventions would be expected to
have no effects, or detrimental effects, on the
offenders sympathetic, compassionate,
responses to victims.
73
Methods of Victimization
Awareness/Empathy Training
• Presentation of information on the typical trauma to
sexual assault victims
• Use of audiovisual materials
• Written assignments
• Group education and confrontation by adult sexual
assault survivors
• Role play
74
Methods of Victimization
Awareness/Empathy Training (cont.)
• Each offender describes his worst offense from the
victim’s perspective
• Introduces his victim by first name and age
• Describes how he accessed and groomed the
victim
• Describes what he did to influence the victim not to
report
• Discusses how the victim is doing now
• Postulates what the victim would like to say to him
or ask him now
75
Interpersonal Functioning—The
Third Domain of Treatment
• Why is this important?
• Persons with poor social skills may, out of
frustration:
• Overpower victims, or
• Retreat to the lower stress environment
of children
• Improved social skills and success can reduce
the need to resort to abusive behavior to interact
with others or meet emotional needs
76
The Goals of Increasing
Interpersonal Functioning
To increase social skills in:
•
•
•
•
•
Meeting strangers
Initiating and maintaining conversations
Correctly interpreting non-verbal communication
Developing appropriate non-verbal skills
Understanding appropriate methods of indicating
interest and disinterest
• Managing anxiety
77
The Goals of Increasing
Interpersonal Functioning (cont.)
•
•
•
•
•
Appropriate personal disclosure
Transitioning from social to social-sexual interactions
Maintaining friendships
Respecting women and children
Understanding the importance of addressing attention to
others beyond one’s self
78
Methods of Social Skills Training
• Presentations on relevant topics
• Role play various types of social settings/interactions
• Behavioral assignments with reports back to the group
79
Rationale for Assertiveness
Training
• Assertiveness increases self-esteem, reduces
shame and anger, and increases satisfaction in
interpersonal interactions
• Sex offenders often suffer from shame and/or
anger when they assert themselves
• They often store up slights, humiliations, and
react with inappropriate anger—sometimes
contributing to violent sexual abuse
80
Goals of Assertiveness Training
• Learn that the primary purpose of assertiveness
is not to change others’ behavior but rather to
increase self-respect
• Reduce fear, shame and anger in interpersonal
interactions
• Increase appropriate self-respect and selfesteem
• Improve effective interpersonal interactions
• Teach specific assertiveness skills
81
Methods of Assertiveness
Training
• Presentation on relevant topics
• Clarify differences between assertiveness,
passivity and aggression
• Role play various social situations or settings
• Behavioral assignments with reports back to the
group
82
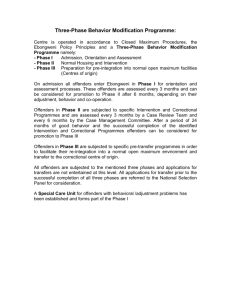
Shame vs. Guilt
• Shame
Focus on ‘bad self’
Self as unchangeable
Self-focus reduces empathy
Feel exposed and scrutinized
Defensive externalization
Hostility, low esteem,
hopelessness
Cripples coping response
Leads to entitlement
(Kurt Bumby, 2003)
• Guilt
Focus on ‘bad behavior”
Views behavior as changeable
Promotes sense of
responsibility
Discomfort from impact of
behavior on others
Optimism and self efficacy
increases
Motivates commitment to
make amends and personal
change
83
Rationale for Sexual Values
Clarification Training
• Many sex offenders have deficits in sexual knowledge
• They may commit offenses in part because they have
unreasonable expectations of their sexual functioning,
have high anxiety in sexual situations, or have had
negative experiences with consenting sexual partners
84
Goals of Sexual Values
Clarification Training
• Increase knowledge about basic, healthy sexual
functioning
• Promote positive, respectful attitudes toward
women and children
• Educate about normal sexual attitudes,
behavior, and performance
• Reduce anxiety about sexual matters
• Increase information about sexually transmitted
diseases
85
Behavior Management—The Fourth
Domain of Treatment
Sex offending is a choice made by the offender.
Relapse prevention is also a choice. Both
require commitment, consistently reaffirmed, to
the goal. Effective treatment and supervision
can assist and encourage the offender to
behave in responsible and non-victimizing ways.
86
Relapse Prevention
• First used in the treatment of alcohol and other drug
abuse
• If behavior could be managed to avoid certain
situations, then relapse was less likely
• Applied now in the treatment of sex offenders
87
Rationale for Relapse Prevention
• Sex offenders who believe that treatment will
eliminate their risk for reoffense are more likely
to recidivate
• Offenders who understand that they are never
“cured,” recognize offense precursors, and
avoid high risk thoughts, feelings, and behaviors
are more likely to remain offense free
• Others must also accept this risk to reoffend
88
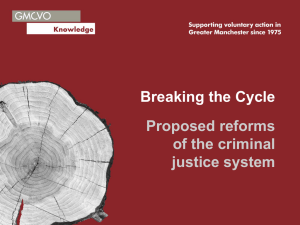
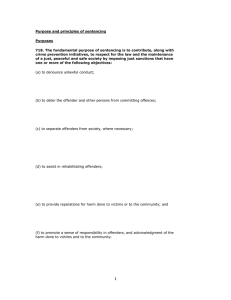
Relapse Prevention Cycle
Abstinence
(sense of control, continued success expected)
Seemingly Unimportant Decision?
Yes
No: Prevention
High-Risk Situation
(Sense of control threatened)
Adequate Coping Response
No
Yes: Prevention
Lapse
Abstinence Violation Effect (giving up)
Adequate Coping Response?
No
Yes: Prevention
Relapse (Reoffense)
89
Goals of Relapse Prevention
The sex offender must learn:
• That prevention of new offenses is a life-long process
and daily choice
• That certain situations, thoughts, or chains of events
pose high risk for re-offense and must be avoided or
managed
• That seemingly unimportant decisions can lead to reoffense
• That risk to re-offend is not static
• To respect/fear his risk to reoffend
90
Goals of Relapse Prevention (cont.)
The sex offender must learn the typical sequence
of events that lead to relapse:
•
•
•
•
•
•
Perception of control
Introduction of a negative mood state
Engaging in fantasies of reoffending
Development of a plan to commit the offense
(Often) use of disinhibiting substance
RELAPSE
91
Goals of Relapse Prevention (cont.)
The sex offender must learn that:
• If he interrupts this sequence with positive coping, he
can reduce the likelihood of reoffending
• A lapse is the occurrence of any step in the sequence
short of reoffending
• Interrupting the pre-offense behavior cycle is easiest to
do in its early stages
92
Methods of Relapse Prevention
• Dispel offenders’ misconceptions about their reoffense
risk—IT’S STILL THERE
• Identify and share high risk factors and relapse
indicators
• Refine avoidance and coping skills and strategies
• Design plan to avoid first lapse and how to prevent a
lapse from becoming a relapse
• Learn self-monitoring of moods and behaviors
• Inform, motivate and empower supervisors
93
Methods of Relapse Prevention
(cont.)
• Write an autobiography to understand life
patterns that result in offending
• Teach problem-focused coping responses
• Control stimuli that might promote relapse
• Teach the relapse process
• Teach that urges subside with time
• Teach avoidance and escape strategies
94
Methods of Relapse Prevention
(cont.)
• Teach relapse rehearsal
• Promote lifestyle changes
• Identify prosocial methods to express power
95
Examples of High Risk Factors
•
•
•
•
•
•
•
•
•
Angry
Lonely
Tired
Bored
Frustrated
Rejected
Confused
Unhappy
Pressured
•
•
•
•
•
•
•
•
•
Potential victims
Alcohol and/or drugs
Some TV or movies
Pornography
Alone, unsupervised
Money problems
Relationship problems
New freedom
Pain or poor health
96
Examples of Relapse
Indicators
• Absence of appropriate sexual activity
• Denial of risk to reoffend
• Distance from supervisors, associating with those who
don’t know or don’t care
• Using alcohol or drugs
• SOBS
• Testing oneself
• Unstructured or unmonitored time
• Change in routine, appearance or demeanor
• Access to potential victims
97
Ethical Practice Standards
• Balancing the safety of the community with the
offender’s privacy
• Informed consent
• Association for the Treatment of Sexual Abusers
(ATSA) is the major professional organization that
speaks to ethical practice standards in this field
• ATSA has issued a “Code of Ethics” as well as practice
standards and guidelines
• www.atsa.com
98
A Major Ethical Issue: Informed
Consent
At a minimum, sex offenders entering treatment should
have spelled out to them—preferably in writing:
•
•
•
•
The purpose and nature of treatment
Its expected duration
Its anticipated benefits, costs, and risks
Limitations of confidentiality
99
Adjunctive Therapies
•
•
•
•
•
•
•
Marital and family therapy
Family education seminars and couples’ groups
‘Non-offending spouse’ groups
‘Approved supervisor’ groups
Substance abuse treatment
Educational/vocational supports
Individual therapy (usually for other issues)
100
Mental Illness and Sex
Offenders
•
•
•
•
Most sex offenders are not mentally ill
Some sex offenders are mentally ill
Most persons with a mental illness never offend
Persons with a mental illness are more likely to
be victims than offenders
• Mental illness does not cause or explain sex
offending
101
Paraphilias
• Category of mental illness sometimes
diagnosed in sex offenders
• Essential feature is a ‘recurrent, intense sexually
arousing fantasies, sexual urges, or behaviors
(at least 6 months) generally involving:
• Nonhuman objects
• Suffering or humiliation of self or other
• Children or nonconsenting adults’
102
Paraphilias (cont)
• ‘The behavior, sexual urges, or fantasies cause
clinically significant distress or impairment in
social, occupational, or other important areas of
functioning.’
• For some individuals, these paraphiliac
fantasizes or stimuli are essential for sexual
arousal.
• For others, paraphiliac preference is episodic
only.
103
Types of Paraphilias
• Exhibitionism; exposure of genitals
• Fetishism; use of non living objects
• Frotteurism; touching/rubbing against
nonconsenting person
• Pedophilia; focus on prepubescent children
• Sexual Masochism or Sadism; receiving or
inflicting humiliation or suffering
• Transvestic Fetishism; cross-dressing
• Voyeurism; observing sexual activity
104
Paraphilias and Sex Offending
• Exhibitionism, voyeurism and pedophilia are the
most frequent paraphiliac diagnosis among
identified sex offenders
• These behaviors are by their nature unlawful
105
Exhibitionism
•
•
•
•
With or without public masturbation,
Usually not physically assaultive,
Often begins in adolescence,
Frequency of arrests decrease after 40
106
Voyeurism
• Usually not physically assualtive
• Often begins before 15
• Often chronic in nature
107
Pedophilia
• Prepubescent children, 13 y/o and younger
• Offender 16 y/o or older, 5 year plus age
difference between offender and victim
• Specify
• Exclusive vs. Non exclusive
• Males, Females, Both
• Limited to incest
108
Sexual Dysfunctions
•
•
•
•
•
•
Premature Ejaculation
Male Erectile Dysfunction
Hypoactive Sexual Desire Disorder
Male Orgasmic Disorder
Dyspareunia
Subtypes
• Lifelong vs. acquired
• Generalized vs. situational
• Psychological vs. combined factors
109
Personality Disorders
• Enduring pattern of inner experience and
behavior that markedly deviates from cultural
expectations. Two or more; cognition, emotions,
interpersonal functioning, impulse control
• Inflexible and pervasive across situations
• Clinically significant distress or impairment
• Stable, long duration (adolescence)
• NOT another MI, substance abuse, medical
110
Antisocial Personality Disorder
• Pervasive pattern of disregard for and violation of rights
of others. Since 15 y/o, 3 or more of
• Repeated criminal acts
• Deceitfulness, lying, aliases, conning
• Impulsivity, failure to plan ahead
• Irritability/aggressiveness, fights/assaults
• Reckless disregard for safety (self/other)
• Consistent irresponsibility, work history
• Lack of remorse or indifference to harm caused
111
Antisocial Personality Disorder
(cont)
• Over 18 y/o
• Conduct Disorder by 15 y/o
• Sociopathic/psychopathic as extreme version
112
Other Mental Illness
•
•
•
•
•
Major Depressive Disorder
Bipolar Disorder
Posttraumatic Stress Disorder
Psychotic or Delusional Disorders
Other Anxiety Disorders
• Social Phobia
• Generalized Anxiety
• Agoraphobia
113
Mental Illness and Offending
• Mental Illness is often used as excuse,
justification, or a description of criminal acts
• Many MI complaints follow or increase after
arrest
• Most MI complaints decrease dramatically with
SOS treatment
114
Mental Illness and Insanity
• Insanity is a legal concept regards culpability or
diminished capacity
• All criminally insane individuals are MI, very few
individuals with a MI are insane
• Criminally insane individuals are not able
appreciate their behavior as unlawful or conform
their behavior to the law
115
Substance Abuse and Sex
Offending
• Some addicts/alcoholics are sex offenders, most
are not
• Alcohol/drug use can increase risk
• Sobriety increases safety
• Most offenders are sober at time of abuse
• Some recovering addicts/alcoholics continue to
sexually abuse
• Successfully drug/alcohol treatment is essential
but not sufficient
116
Treatment Progress and
Provider Characteristics
• Treatment has been found to reduce recidivism
(Hanson et al 2002)
• Treatment failure increases recidivism (Hanson
& Bussiere 1998)
• High risk offenders are less compliant with
treatment and supervision (Hanson & Harris
1998)
117
Treatment Progress and
Provider Characteristics (cont)
• Denial and engagement together significantly
correlated with treatment progress
• In combination, engagement and denial
explained close to 60% of the variance in
treatment progress
• Engagement was a stronger predictor then
denial (Beta .52 & -.37, respectively)
Levenson, 2003
118
Treatment Provider Characteristics
• In the past, sex offender treatment has often involved a
punitive treatment style characterized by aggressive verbal
confrontation between offender and therapist (therapeutic
reaming)
Studies have examined how therapist styles affect the
success of treatment:
• Marshall et al., Clinical Psychology and
Psychotherapy (In Press)
• Marshall et al., Journal of Sexual Aggression (In
Press)
• Jill Levenson, ATSA 2003
119
Treatment Provider
Characteristics (cont.)
Some treatment targets seem to be better achieved with
the use of treatment delivered with a motivational
approach based on empathic understanding, mutual
trust and acceptance.
• Reduction in sense of entitlement to sexual gratification
• Reduction of mistrust of women
• Reduction in impulsivity
• Client engagement
120
Practice Implications
• Providers should consider a positive, invitational and
motivational style that supports offender engagement in
group
• Setting expectations for mutual aid and modeling
effective communication and helpfulness will foster
engagement
• Group members can take a major role in confrontation
which may reduce shame and fears of judgment or
rejection.
• This approach may reduce the salience of the protective
function of SOBS and denial
121
Choosing SOS Evaluators and
Treatment Providers
• Lack of standardized certification or other
credentialing in most jurisdictions presents a
major difficulty in promoting common standards
of practice
122
However, in Illinois…
• The Illinois Sex Offender Management Board
(www.ag.state.il.us/communities/somb/index.html) has
published standards for the evaluation,
treatment and supervision of adult sex
offenders.
• Also, there is an interim list of individuals that
have met SOMB qualifications for SOS
evaluators and/or providers
123
SOMB Interim Qualifications
for SOS Providers
• Bachelor’s degree or higher in relevant field
• 400+ hours of supervised experience in last 4
years, at least 200 face-to-face
• Completed 10+ SOS evaluations in last 4 years
• 40+ hours documented training in the specialty
of sex offender specific assessment, treatment
or management
• Provide SOS evaluations and/or treatment in
accordance with SOMB standards of practice
124
SOS Providers as
Collaborative Partners
• A willingness to collaborate and cooperate work
with other professionals, including:
• Probation and parole officers
• Victim Advocates
• Polygraph examiners
• Other evaluators and treatment providers
• Attorneys, prosecutors, and other criminal
justice representatives
125
Special Populations
• Juvenile sex offenders
• Female sex offenders
• MR/DD sex offenders
126
Juvenile Sex Offenders
• Similarities to Adult Offenders
• Victimize others
• SOBS
• Empathy deficits
• Impaired interpersonal functioning
• Not all alike, don’t all need the same thing
127
Juvenile Sex Offenders
• Differences from Adult Sex Offenders
• Don’t belong in ASO treatment program
• Psychopathy less common
• Deviant arousal less common
• Interpersonal competency and esteem
problems more significant
• Juveniles may be more amenable to and
benefit more from appropriate SOS treatment
128
From Juvenile to Adult Sex
Offender
• Not all juvenile sex offenders will become adult
sex offenders
• Long term risk for competently treated juvenile
sex offenders is encouraging
• High value on identifying and properly managing
juvenile sex offenders
• Not all adult sex offenders were juvenile sex
offenders
129
What about children?
• Children can and do behave in sexually
aggressive ways that hurt others
• However, it is not usually appropriate or helpful
to label them as Sex Offenders
• Specialized assessment, intervention and
management is indicated
• Sexually aggressive/reactive children should not
be placed or treated with Juvenile Sex
Offenders
130
Female Sex Offenders
• Adult females
• Account for 10-20% of
sexual abuse of
children
• Care-giving context
• Socially isolated
• Attachment issues
• History of PTSD,
addiction and MI
• Victimized 2X male
ASO
• Adolescent females
• Much more likely
victimized sexually
• Emotional abuse and
neglect victims
• Physical and domestic
abuse
• Use less force or
coercion
• Abuse in care-giving
context
131
Female Sex Offenders
• Don’t typically belong in male sex offender
programs
• Not all alike, don’t all need the same treatment
program
• More research and programs needed
• Hurt people
• Often overlooked by community,courts and
providers
132
MR/DD Sex Offenders
• Offenders with significant functioning deficits
need specialized treatment from specialized
providers
• Inappropriate to place in program that doesn’t fit
their needs or to forego treatment all together
• Environmental management important
• Increase premium on the commitment and
dedication of supervisors, natural and official
133
Use of Polygraph Examination
in SOS Treatment; Why?
• Very few people (therapists, judges/lawyers or
probation officers included) are much better
than chance at telling when they are being lied
to
• Most people think they are an exception to this
rule
• Sex Offenders lie
• Polygraph Examination (PGE) is better than
chance and we don’t have anything better
134
Utility of PGE in Treatment
• Encourages offenders to disclose earlier and more
completely
• Improves detail and accuracy of risk assessment
• Improves safety planning and decision making
• Motivates offenders to avoid high risk behavior
• Improves safety for community and victim
• PGE improves community safety and enhances
treatment efficacy by increasing amount of accurate
and timely information
135
Concerns About PGE in SOS
Treatment
•
•
•
•
PGE is not 100% accurate
PGE accuracy is affected by skill of examiner
PGE cost money
Not appropriate to base important decisions on
PGE results alone. All information available
must be considered
136
Response to Concerns About
PGE Use
• NO test is 100% accurate, most test are more easily
faked, accuracy is much higher than human detection of
deception
• SOMB standards demand specialized training and
experience for examiners
• Costs are offset by faster movement in treatment and
better success rates for programs using PGE
• It is not responsible practice to ignore any reliable
source of information in making important decisions
137
Accuracy of PGE
• Computerized equipment and scoring have improved
accuracy
• Strength of motivation in the offender examined
improves accuracy (If the offender believes the results of
the exam matter the results are more accurate)
• 52 lab studies; median accuracy of .86, range of .70 to
.95
• Field studies, although more difficult, show higher
accuracy, median of .89
138
Factors Affecting PGE
Accuracy
• No significant differences in accuracy found in
exam subjects based on;
• Personality disorder
• Intelligence (assuming at least 12 y/o level)
• Ethnicity
• Number of PGE taken already
• History of anxiety disorder or high levels of
anxiety at time of test
139
Who Should Be Excluded From
PGE?
• Actively psychotic or out of contact with reality
• Physically illness or medication that renders
PGE unreadable
• Presence of acute pain or illness
• Presence of acute, severe, distress
• Adjusting to recent (last 2-3 weeks) medication
change
140
Types of PGE Used in
Treatment
• History disclosure
• Maintenance/monitoring
• Specific issue
All include pre and post exam interviews
All PGE are limited to only a few (3-5) specific
questions, chosen in consultation between
provider and examiner. Offenders are informed
of these questions prior to the exam.
141
History Disclosure PGE
• Purpose is to obtain complete history of
offending. Essential for risk assessment, safety
planning, treatment planning.
• Offender, with provider, completes a history
booklet before PGE
• PGE tests the accuracy and completeness of
previous disclosures
• Sometime additional exams are required
142
Maintenance and Monitoring
PGE
• Purpose is to improve compliance with
supervision and safety planning, and to identify
any problems (non-compliance) with same
• PGE covers specific behaviors of the offender
within a specific time frame
• Important for identifying current risk behaviors
before new offense occurs
• Serves to motivate offenders to avoid high risk
as they fear detection of the behavior
143
Specific Issue PGE
• Purpose is to detect deception/truthfulness
regarding a specific incident
• This narrow focus allows for the highest level of
accuracy among the types of PGE discussed
144
Assessing Treatment Progress
• Accurate information and consistent observation
across time are essential in assessing an
offenders progress in treatment
• Since offenders lie it makes no sense to use
their report as the sole source of information in
assessing progress
• Rather, the offenders behavioral change across
time and situations, confirmed by PGE, is the
standard
145
Tools for Assessing Progress
•
•
•
•
Critical and cynical observation across time
Consultation with containment team and others
PGE
Various instruments may be of use
• Sex Offender Treatment Needs and Progress Scale (McGrath &
Cumming, 2003)
• Facets of Sex Offender Denial (Schneider & Wright, 2001)
• Group Engagement Measure (Macgowan, 1997)
• Sex Offender Rating Scale (Anderson et al, 1995)
146
Change in Behavioral
Restrictions
•
•
•
•
•
Only after sufficient progress in treatment
Only with collaboration with team
Only with specific safety plan
Only with increased supervision
Only with monitoring PGE
147
Completion of Treatment
• Completion of treatment does not imply the end
of supervision or elimination of risk to the
community
• Treatment should be viewed as ranging from
intensive to aftercare
• If risk increases, treatment should be re-instated
148
Completion of Treatment (cont)
• The containment team should consult about the
completion of treatment
• The decision should come after the evaluation,
treatment plan, course of treatment sequence,
and a minimum of a non-deceptive disclosure
PGE and two or more non-deceptive
maintenance PGE regarding compliance with
probation/parole orders, treatment contract and
avoidance of high risk situations
149
Unsuccessful Termination from
Treatment
• Increase in risk such that continued placement
in the community is not safe
• Reoffense
• Repeated refusal to comply or engage in
treatment process despite sanctions
• Refusal to accept identity as sex offender
150
Personally Relevant
Circumstances
• Strict adherence to letter and spirit of probation
order and SOS treatment contract
• Initiate consequences early and hard
• Range of consequences
• Keep court/judge informed of progress or lack of
• Consider PTR with jail time plus new term of
probation for significant violations that no not
necessitate termination
151
Contact with Children or
Family Reunification
•
•
•
•
•
ONLY IN BEST INTEREST OF CHILD
Only after sufficient progress in treatment
Only with “approved supervision”
Only with increased monitoring and PGE
Only with strict and specific rules and
restrictions
• Only with regular and ongoing coordination with
victim advocate or family therapist
152