Immunopathology
advertisement

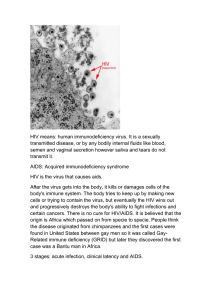
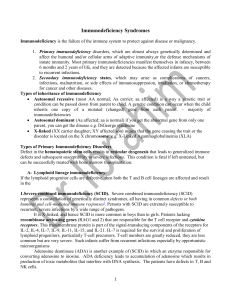
Section 5 Immunodeficiency 1. Primary immunodeficiency (1) Pure immunoglobulin deficiency ① Bruton-type gammaglobulinaemia ② Hypogammaglobulinaemia of late onset ③ Dysgammaglobulinaemia In these disorders these is susceptibility to bacterial and yeast infections, but viral infections are controlled normally. Cellmediated reactions are intact. (2) Pure T-cell deficiency ① Thymic agenesis ② Thymic alymphoplasia (dysplasia) ③ Thymic hypoplasia or aplasia Here the immunoglobulin levels are normal but there is a complete absence of cell-mediated reactions (3) Mixed deficiency 2. Secondary immunodeficiency Resulting from: (1) Excessive loss of immunoglobulins ① Protein-losing enteropathy ② Nephrotic syndrome (2) Depression of the immune system by ① Old age ② Malnutrition ③Viral infections such as acquired immunodeficiency syndrome. ④ Leprosy ⑤ Malaria ⑥ Sarcoidosis ⑦ Surgery ⑧ Uraemia (3) Immunosuppression by ① X-rays ② Corticosteroids ③ Cytotoxic drugs ④ Antilymphocyte serum ⑤ Anntimetabolits (4) Neoplasia ① Hodgkin’s disease ② Multiple myeloma ③ Waldenstrom’s macroglobulinaemia ④ Chronic lymphatic leukaemia (5) Splenectomy Acquired Immunodeficiency Syndrome (AIDS) In June 1981, the centers for disease control of the United States reported that five young homosexual men in the Los Angeles area had contracted the AIDS Etiology: human immunodeficiency virus (HIV) HIV (from Robbins Basic Pathology ,2003) Features: ① A long incubation period, followed by a slowly progressive fatal outcome. ② Tropism for hematopoietic and nervous systems ③ An ability to cause immunosuppression ④ Cytopathic effects in vitro. Epidemiology Worldwide: about 10 million people are infected. Five groups of adults at high risk for developing AIDS: ① Homosexual or bisexual males ② Intravenous drug abusers ③ Hemophiliacs ④ Recipients of blood and blood components ⑤ Heterosexual contacts Pathogenesis HIV→CD4+ cell→ CD4+ cell lysis → opportunistic infections and neoplasms Morphology Neither specific nor diagnostic. ① Widespread opportunistic infections ② Kaposi’s sarcoma ③ Lymphoid tumors The multiple effects of loss of CD4+ T cells as a result of HIV infection (From Robbins Basic Pathology ,2003) Slide 7.41 AIDS with Kaposi sarcoma Kaposi sarcoma in liver of AIDS patients AIDS with herpes Offered by Prof Song W Wong AIDS-related Marked follicular hyperplasia (early stages) HIV infection showing the formation of giant cells in the brain. (Dr. Dennis Burns) . (From Robbins Basic Pathology ,2003) Slide 7.40 Lymph nodes: Marked follicular hyperplasia (early stages)→ Lymphoid cells depletion (empty-looking lymph nodes or spleen and thymus in later stages). Mortality: 100%