Best Practices and Resources in
School Mental Health
Mark D. Weist & Dana Cunningham
University of Maryland
Center for School Mental Health
April 28, May 21, 2008
Center for School Mental Health*
University of Maryland School of Medicine
http://csmh.umaryland.edu
*Supported by the Maternal and Child Health Bureau of HRSA
and numerous Maryland agencies
Referrals from Schools
to Other Settings
96% referred to school-based
program received services
13% referred to other community
agency did
Catron, T., Harris, V., & Weiss, B. (1998)
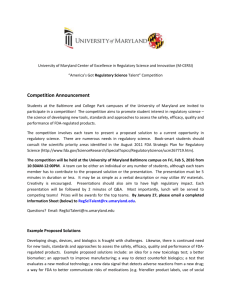
Treatment as Usual Show Rates
Percent of Youth Remaining in Services
(McKay et al., 2005) from Kimberly Hoagwood
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
72%
49%
26%
9%
Number of Sessions
Other Concerning Facts
Around 1 in 5 youth will present an
emotional/behavioral disorder (5 students in a
classroom of 25)
Between 1/6th and 1/3rd receive any services
Modal number of specialty mental health visits
is 2
Major lack of systematic quality assessment
and improvement in traditional settings
Silos
“The various systems do not talk to each other,
resulting in many children falling through the
cracks and not receiving care, receiving
duplication of services, or families needing to
negotiate a confusing, fragmented array of
services” (Family Advocate, Louisiana)
“Shame” and “Strain” on Families
“Youth and families experience blame; have
widespread distrust of professionals; have
concerns about losing custody; are often
unable to pay for care…have to glue services
together”
– Kimberly Hoagwood (Congressional Briefing, October,
2007)
April 16, 2007
“Rather than falling through the
cracks, Cho crawled into the cracks
and hid there”
-Chris Fynn- director of VA Tech’s
counseling center
Shuchman, M. (2007)
Growing Focus on School Mental Health
Schools as the “defacto” sites for mental health care
U.S. Surgeon General Reports (1999, 2000)
President’s New Freedom Commission on Mental Health
Report (2003; www.mentalhealthcommission.gov)
Educational Mandates, e.g., Response to Intervention
A range of federal grant programs
Strong international interest
Advantages
ACCESS
Promotion and Prevention
Efficiency and Cost Effectiveness
Systems Collaboration/ Economies of Scale
Natural/ Ecological Approach
Reduced Stigma
A Cogent Rationale
Integrated approaches to reduce academic and
non-academic barriers to learning are the most
effective in achieving the outcomes families,
schools and communities care about
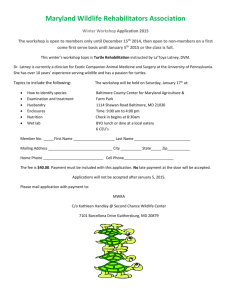
The Public Health Approach
Academic Systems
Behavioral Systems
Intensive, Individual Interventions
•Individual Students
•Assessment-based
•High Intensity
1-5%
Targeted Group Interventions
•Some students (at-risk)
•High efficiency
•Rapid response
Universal Interventions
•All students
•Preventive, proactive
5-10%
80-90%
1-5%
Intensive, Individual Interventions
•Individual Students
•Assessment-based
•Intense, durable procedures
5-10%
Targeted Group Interventions
•Some students (at-risk)
•High efficiency
•Rapid response
80-90%
Universal Interventions
•All settings, all students
•Preventive, proactive
A Vision for School Mental Health
Strong stakeholder involvement and a shared
family-school-community system agenda
Full continuum of effective supports and
services for all students in general and special
education
The right staff with the right training,
supervision, coaching and support
Vision (cont.)
Emphasis on quality assessment and
improvement and evidence-based practice
Strong focus on achieving valued outcomes
Outcome findings feed back into program
improvement and into policy and advocacy
agendas
Another Triangle
Desired Outcomes
Effective mental health promotion and intervention
Outstanding staff and program qualities
Ongoing training, technical assistance & support
School and community buy-in and investment
Resources
Awareness raising, advocacy, policy improvement
But in most communities…
The vision is not a reality as staff and
programs are not adequately supported and
often contending with tremendous need, and
In an environment of low support and high
needs, positive outcomes will most likely not
be achieved and efforts will stall
Prince George’s County School Mental
Health Initiative
Intensive, evidence-based mental health
intervention for students in special education
in two schools
Training and support to 11 schools with
specialized programs for youth presenting
emotional problems
Broader training and support county wide (e.g.,
for all school psychologists)
Partners
University of Maryland CSMH
Prince George’s County Public Schools (PGCPS)
Maryland State Department of Education (MSDE)
Staffing for Two Schools
One PGCPS liaison
Two therapists
One case manager
Parent Liaison
Psychiatric consultation
Student Criteria
At-risk for non-public placement
Social-emotional goals on IEP
Behavioral intervention plans
Acting out problems
Multiple risks
Family interest
Program Framework
Build supportive relationships with the youth and
family
Decrease risk factors
Enhance strengths and protective factors
Enhance development of key cognitive behavioral
skills
Program Framework (cont.)
Improve problem solving
Improve anger management skills
Address trauma history
FOCUS ON QUALITY CONSTANTLY
Key Processes in Working with
Families
Engagement
Empowerment
Support
Collaboration
Family Needs Addressed
Food, health insurance, medical needs,
clothing, transportation, utilities, substance
abuse services, mental health services,
tutoring, mentoring, recreational programs
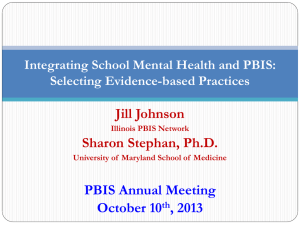
Anxiety: Practice Components
97
Exposure
44
Modeling
% of EBP w/
Practice
Component
39
Cognitive/Coping
31
Relaxation
0
20
40
60
80
100
Use of Evidence-Based Programs
Anger Management Group
–
–
–
–
–
–
–
Identifying anger early
Understanding short- and long-term consequences
Recognizing and managing emotions
Understanding cognitive processes
Developing coping skills
Learning to problem solve
Communicating effectively
Qualitative Evaluation - Families
“The therapists are always available when we
need them”
“My granddaughter is less angry now than she
used to be”
“The case manager helped me get back on my
feet after I lost my job”
Student Feedback
They liked having a therapist at school for the following
reasons:
“They give you good advice.”
“If you have a problem, they are right there.”
“You can get stuff off
your chest.”
“It’s free.”
“They are on your side.”
“You get out of class and don’t have to do work.”
Absences by Quarter
10
9
8
7
6
5
4
3
2
1
0
1st Qtr
2nd Qtr
3rd Qtr
4th Qtr
INV
4.24
6
6.06
5.35
Non INV
2.69
5.25
10
9.88
Suspensions by Quarter
2.5
2
1.5
1
0.5
0
INV
Non INV
1st Qtr
2nd Qtr
3rd Qtr
4th Qtr
1.24
0.94
0.94
1.12
1
2.06
1.31
1.19
Data on Non-Public Placements
Between September, 2006 and March, 2008,
43 students were seen for more intensive
services in the two schools
All met multiple criteria for placement in nonpublic programs
3/43 students were placed in a non-public
program
Data (cont.)
Preliminary economic analyses indicate:
– For 1.6 years of services (as of 3/14/08), 25
placement years were diverted
– For a savings of between $800,000 and $1,000,000
for Prince Georges County alone
Agendas
The Prescriptive Agenda (e.g., implementing
evidence-based services in schools,
documenting outcomes, building advocacy,
growing into more schools) is dependent on
The Collaborative Agenda (i.e., building
relationships, promoting dialogue and
developing true collaboration and partnerships)
A National Community of Practice
CSMH and IDEA Partnership
(www.ideapartnership.org) providing support
30 professional organizations and 12 states
10 practice groups
Providing mutual support, opportunities for
dialogue and collaboration
Advancing multiscale learning systems
Sign up at www.sharedwork.org
10 Practice Groups
Mental Health-Education Integration
Developing a Common Language
Connecting Education and Systems of Care
Connecting SMH and Positive Behavior
Support
Improving SMH for Youth with Disabilities
10 Practice Groups (cont.)
SMH, Juvenile Justice and Dropout Prevention
Family Partnerships
Youth Involvement and Leadership
SMH – Child Welfare Connections
Quality and Evidence-Based Practice
Twelve States
Hawaii
Illinois
New Hampshire
North Carolina
Maryland
Missouri
New Mexico
Ohio
Pennsylvania
South Carolina
South Dakota
Vermont
Maryland is the National SMH Leader
UMBC Dissertation, April, 2007
Lisa Sadzewicz
“Diffusion of Innovation: State Factors that
Influence the Spread of School Mental Health
Policies and Programs”
Survey of State Children’s Mental
Health Directors on SMH Innovation
Nominations:
–
–
–
–
1. Maryland (9)
2. California (6)
3. Ohio (5)
4. North Carolina (4)
Policy/Funding Mechanisms used
to Support SMH
Number:
–
–
–
–
1. Massachusetts (16)
2. Maryland (15)
3. North Carolina (14)
4. Californian (13)
School Mental Health Workgroup
Established in 2002 as part of MHA’s
Blueprint strategic planning process
Promoting a coordinated SMH agenda for MD
Two statewide surveys of SMH
Providing assistance to federal grant proposals
Developing SMH outreach and services for
youth in foster care
CSMH Training Events
13th Annual Conference on Advancing School
Mental Health. Phoenix, Arizona, Florida.
September 25-27, 2008
School Health Interdisciplinary Program
(SHIP). Ellicott City, Maryland. August 4-7,
2008
See http://csmha.umaryland.edu or call 410706-0980 (or 888-706-0980 toll free)
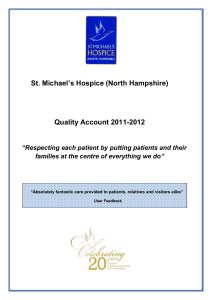
www.schoolmentalhealth.org
Website developed and maintained by the
CSMH with funding from the Baltimore City
Health Department
User-friendly mental health related
information and resources for caregivers,
teachers, clinicians, and youth
Home
About Us
Resources for
Clinicians
Resources for
Educators
Resources for
Families
Resources for
Students
FAQ
Baltimore City
Resource Directory
Welcome to the School Mental Health Connection!
This site offers school mental health resources not only for clinicians, but
also for educators, administrators, parents/caregivers, families, and
students. To efficiently find resources that fit your needs, just click the link to
the left that corresponds to your role in the school community. However,
since you may benefit from resources in numerous domains within this site,
we encourage you to explore many areas.
The resources on this site emphasize practical information and skills based
on current research, including prominent evidence-based practices, as well
as lessons learned from local, state, and national initiatives.
The School Mental Health Connection is designed for use by anyone who is
interested in school mental health. It is also a central feature of the
Baltimore School Mental Health Technical Assistance and Training Initiative.
What's New
View the newly-released Directory of Community Services for
Baltimore City.
Educators: Check out the user-friendly Mental Health Fact Sheets for
the Classroom, provided by the Minnesota Association for Children's
Mental Health.
Consultation &
Support Line
© 2006 The School Mental Health Connection. All Rights Reserved.
Other Helpful
School Mental Health Websites
Center for the Advancement of Mental Health Practices
in Schools
http://schoolmentalhealth.missouri.edu/about.htm
Center for School-Based Mental Health Programs
http://www.units.muohio.edu/csbmhp/
UCLA Center for Mental Health in Schools
http://smhp.psych.ucla.edu
INTERCAMHS
International Alliance for Child and
Adolescent Mental Health and Schools
www.intercamhs.org
Two Books
Handbook of School Mental Health (2003,
paperback – 2007)
– www.springer.com
Advances in School-Based Mental Health
Interventions (2007)
– www.civicresearchinstitute.com/sbmh.htm
Two New Journals
Advances in School Mental Health
Promotion
– The Clifford Beers Foundation and the University
of Maryland
– www.schoolmentalhealth.co.uk
School Mental Health
– www.springer.com
Contact Information
Center for School Mental Health,
Department of Psychiatry
University of Maryland
737 W. Lombard Street, 4th Floor
Baltimore, MD 21201
PH: 410-706-0980
FX: 410-706-0984
mweist@psych.umaryland.edu
http://csmh.umaryland.edu