HCOASC Delirium Care Pathways Project Advisory Committee
advertisement

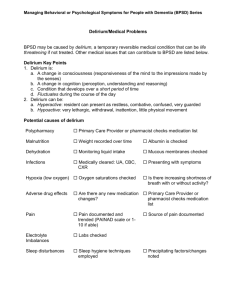
Developing and Implementing “Delirium Care Pathways” Associate Professor Victoria Traynor School of Nursing, Midwifery & Indigenous Health and NSW/ ACT Dementia Training Study Centre, University of Wollongong & Nicole Britten Agedcare Services Emergency Team (ASET) Wollongong Hospital, Illawarra and Shoalhaven Local Health Network Best Practice Delirium Care in Australia • Department of Health & Ageing – 2006: Publication of “Delirium Clinical Practice Guidelines” – 2008: University of Wollongong commissioned to develop delirium care pathways – 2011: Publication of “Delirium Care Pathways” • CPG: 121 page document • Low level awareness that document exisits • Stoke Pathway: 46 page document • What can we do to increase awareness and use of pathway documents? “Delirium Care Pathways” Project Aims • Build on the “Clinical Practice Guidelines for the Management of Delirium in Older People” Develop cross-setting “Delirium Care Pathways” for • – – – (i) community (ii) acute (iii) residential aged care facilities Overall Project Design • Deductively develop “Delirium Care Pathways” • Range of stakeholders involved developing content and format – Practitioners – Patients/ clients – Carers • Qualitative data collection and analysis • Expert Advisory Group reviewed content and format throughout project • Trial of “Draft Delirium Care Pathways” Three Stage Project • Stage one – Literature review – Ethics approval from UoW and SESIAHS – Draft “Delirium Care Pathways” Version1 • Stage two – Focus groups and interviews – Draft “Delirium Care Pathways” Version2 – Draft “Delirium Care Pathways” Version3 • Stage three – Trial of Draft “Delirium Care Pathways” Version3 – “Delirium Care Pathways” Final Version Stakeholder Involvement State-wide and cross-setting representation • Practitioner Interviews –4 • Expert Interviews –4 • Focus groups – 7 (37 participants) Summary of Themes • Clinical Guidelines • Relevance of Pathways • Purpose of Pathways • Content of Pathways: Assessment and screening • Patient journeys to reflect cross-setting relevance of Pathways • Publication and distribution of Pathways Trial of “Delirium Care Pathways” • 15 sites –3 x community –5 x acute (3 x ASETs and 4 x wards) –5 x Residential Aged Care Facilities (high and low care) • 12 patients Improving practice • Knowledge translation – Awareness, acceptance, application and adherence • Diffusion process – Rogers model • Practice development – Manley, McCormack, Titchen, Dewing and Walsh – Critical social science and organisational culture change • The ‘Dementia Bridge Walk’ – Tom White, DCRC Implementing “Delirium Care Pathways” • Setting – Community – Acute – Residential Aged Care Facilities • Target audience – Registered Nurses and Enrolled Nurses – Medics including GPs – Allied health practitioners • Format – Printed copy – Poster version – Internet web version with hyperlinks embedded DELIRIUM CARE PATHWAYS Final Version6 Consider for use if aged over 65 years or 45 or older for Aboriginal or Torres Straight Island Communities (ATSI) Delirium may be a life threatening and potentially reversible condition Preventative Strategies for Delirium Has the patient/client been identified as potentially suffering from delirium? No Yes • Cognitive function assessment tools */pg 3 or ensure appropriate referral is made • Known risk factors for the development of delirium pg 4 • Information from patient/client, carer, GP, medical record or facility assessments • Delirium diagnostic tools or diagnosis by Expert * /pg 7 1. Conduct baseline cognitive function assessments * Does patient/client have a cognitive impairment? No Yes 2. Determine any changes in cognitive function Has there been a recent change in cognitive function? Yes No 3. Assess for Delirium Does patient have a confirmed diagnosis of delirium? Yes No 4. Consider subclinical delirium Does patient/client have some symptoms of delirium? Yes No Include in care plan • Prevention pg 5 • Screen at regular intervals for change in cognitive function pg 3 • Risk factor assessment and management pg 4 • Involve Mental Health Team as relevant Differential diagnosis (refer to Poole’s Algorithm pg 6) Adapt care plan • Consider who is consenting to care • Identify and address causes pg 8-10 • Manage symptoms pg 11 • Pharmacological management pg 12 • Provide supportive care pg 13 • Prevent complications pg 5 • Monitor resolution following facility guidelines* • Manage modifiable risk factors pg 4 • Educate patient and family, give facility pamphlet or pg 14, consider use of interpreter • Refer to advanced care plan 5. Monitor and respond to any sudden changes in cognitive function by repeating pathway *People to use service/facility preferred diagnostic and assessment tools or other relevant material. Adapted from: Clinical Epidemiology and Health Services Evaluation Unit 2006, Clinical Practice Guidelines for the Management of Delirium in Older People, Victorian Government Department of Human Services, Melbourne, Victoria. 12 Case Study: Community • 83 year old male known to ASET admitted to emergency department with extreme acute confusion. Family not coping with caring for man due to his confused state. Yet again, confusion due to a urinary tract infection which would not have caused delirium if treated sooner when first symptoms noted by community care. Community Outcome • Delirium would not have resulted in a emergency presentation because community staff would have provided some education for family members about UTIs and delirium and ensured anti-biotics prescribed sooner. Case Study: Acute • 78 year old woman lives with family and experiences some level of cognitive impairment and family report a “confusion” which recently increased. Came to emergency with shortness of breath. Doctor reviewed, prescribed anti-biotics, and recommended discharge. ASET fulfilled usual role in “screening” all frail older people discharge. Patient extremely acutely confused and on questioning family patient normally only disorientated to time. Acute Outcome • ASET immediately searched out medic to discuss case. Medic took on board recommendation by ASET and patient admitted to medical ward for further assessment. Case Study: Residential Aged Care Facilities • 88 year old man who has a catheter and presents to the emergency department because of increased wandering and agitated behaviour around care home. On presentation urinalysis reveals a urinary tract infection which was not identified by care home staff. RACF Outcome • It is common for some care homes to not to undertake routine urinalysis of residents with catheters. Admission for 24 hours while intravenous antibiotics have time to start working and extreme acute confusion diminished and care home able to care for gentleman. Implementation strategies • Piggy back on ‘Essentials of Care’ project • Management ‘buy-in’ for clinical staff – – – – Complete facilitation skills sessions Undertake audit Implement practice development strategy Recruit ‘delirium champions in ‘soft target’ clinical area • Bottom up implementation strategy to improve practice Implementation project: Audit • 5 x ASETS in South East Sydney and Illawarra and Shoalhaven Local Health Networks • 200 audits • Presentation rate of delirium • Screening rates for delirium • Treatment rates for delirium • Implementation timeframe Conclusion • Across setting “Delirium Care Pathways” document now approved to accompany “Clinical Guidelines” • Deductively developed documentation informed by experts and current practitioners • User friendly “smart” documentation • Documentation available Australia-wide for use in late 2010 • Potential for use to an international audience • Large scale implementation plan in SESIAHS Aged Services Emergency Team in Spring 2010 References • KPMG (2008) Broken Hill Aged Care Project in the Greater Western Area Health Service: Implementation report Sydney: NSW Health • Han L. McCusker J. Cole M. et al. (2001) Use of medications with anticholinergic effect predicts clinical severity of delirium symptoms in older medical in-patients. Archives of Internal Medicine 161(8):1099-105 • Inouye, Sharon; van Dyck, Christopher; Alessi, Cahty; Balkin, Sharyl; Siegal, Alan & Horwitz, Ralph (1990) Clarifying confusion: The confusion assessment method: A new method for detecting delirium Annals Internal Medicine 113; 941-948 • Karlsson I. (1999) Drugs that induce delirium. Dementia Geriatric Cogn Disord 10:412415 • Aged Care Services, Liverpool Hospital (2004) Delirium in the Older Person Liverpool: South Sydney & Western Area Health Service • Melbourne Health (2006) Clinical Practice Guidelines for the Management of Delirium in Older People Melbourne: Victorian Government Department of Human Services • NHMRC (2003) When Does Quality Assurance in Health Care Require Independent Ethical Approval? Canberra: NHMRC • NSW Health (2007) Guidelines for Ethics Submission Sydney: NSW Health • Poole, Julia & McMahon, Christine (2005) An evaluation of the response to Poole’s Algorithm Education Programme by Aged Care Facility Staff Australian Journal of Advanced Nursing 22(3); 15-20 • Wilhelm, Kay & Brakespear, Michael (2007) Delirium Pathways Sydney: St Vincent’s Hospital Contact Details Associate Professor Victoria Traynor School of Nursing, Midwifery & Indigenous Health NSW/ACT Dementia Training Study Centre Building 41 University of Wollongong Telephone: +61 (2) 4221 5213 Fax: +61 (2) 4221 4718 Web address: http://www.uow.edu.au/nursing /health/nursing/ http://dementia.uow.edu.au