Sexuality & Fertility Issues in Cancer Patients
advertisement

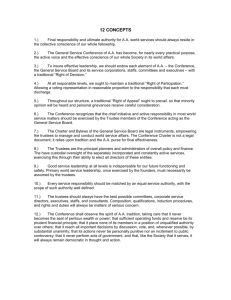
Sexuality & Fertility Issues in Cancer Patients Carolyn Vachani, MSN, RN, AOCN 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 1 Scope of Sexuality Issues • 40-100% of cancer patients experience some form of sexual dysfunction • Issues do not always resolve after therapy • Almost all cancer treatments have the potential to alter sexual function (surgery, chemotherapy, radiation, hormones) • Represents major quality of life (QOL) issue • With intervention, up to 70% of patients can have improved functioning 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 2 To Optimize QOL, Nurses Can: • Learn evidence-based information on how diagnosis/treatment affects sexual function • Conduct assessments before/during therapy • Inform patients of possible changes • Educate clients & partners • Provide guidance & suggestions for adapting to changes • Know resources & refer when needed 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 3 Survey of Physician/Patient Communications If you wanted to talk to your doctor about a sexual problem, how concerned would you be that --- might happen? Your doctor would be uncomfortable talking about the problem because it was sexual in nature 45% Your doctor would dismiss your concerns and say it was just in your head 51% There would be no medical treatment for your problem 20% 46% 0% Very Concerned 23% 10 20 30 40 % % % % Somewhat concerned 30% 50 % 60 % 70 % 80 % Marwick, C Survey says patients expect little physician help on sex. JAMA 1999;281:2173-2174. Nurses’ Beliefs • Someone else will do it • Patients never ask about it, so they must not care • I don’t know how to help or have time • I don’t agree with their lifestyle • They should be happy to be alive • They are too old, sick, young, etc. • I will offend them by asking 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 5 Johnson’s Behavioral Model • All of the patterned, repetitive, purposeful ways of behaving that characterize each person's life make up an organized and integrated whole, a “system” • Categorizes all human behavior into seven subsystems: Attachment, Achievement, Aggressive, Dependence, Sexual, Ingestive, and Eliminative • Disturbance in one subsystem affects the other subsystems • Can be applied to sexual dysfunction 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 6 PLISSIT Model for Communication • Permission (Assessment) • Limited Information (Education) • Specific Suggestion (Counseling) • Intensive Therapy (Referral) • Developed in 1976 by Robinson & Annon based on the four levels of intervention • Applied to sexuality by Estes in 2002 • 70% can be managed by first 3 levels 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 7 Sexual Dysfunction in Men • Chemo/hormonal therapy: Erectile dysfunction, decreased libido, ejaculatory dysfunction, gynecomastia, penile/ testicular atrophy, and infertility • Radiation/ brachytherapy: Urinary issues, impotence, bowel dysfunction, penile/ testicular atrophy • Surgery: Urinary issues, impotence, body image, pain, retrograde ejaculation 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 8 Sexual Dysfunction in Women • Chemo/Hormone therapy: Irregular menses, early menopause, hot flashes, insomnia, irritability, depression, vaginal dryness, painful intercourse, infertility, and decreased libido • Radiation/ brachytherapy: Pelvic fibrosis, vaginal atrophy/stenosis, scarring, decreased lubrication, urinary effects, erythema, edema, ulceration, decreased elasticity, shortening, and increased irritation of vagina • Surgery: Body image, bowel changes, ROM issues, menopause, pain, changes in vaginal size/sensitivity, loss of nipple 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 11 General Nursing Interventions • Ask the question! • Educational resources – ACS booklets for men & women • Suggestions for energy conservation, alternatives to intercourse, position changes, resting • Set the right mood with relaxation, candles, music, wine • Sense of humor 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 13 General Nursing Interventions • Suggest open communication with partner • Use of pillows to alleviate pain with positioning, use of pain meds • Kegel exercises to relax pelvic muscles • Treat depression • Neutropenic pts - no intercourse / tampons • Referral to therapist – relationship & sexual issues – Look for AASECT (American Association of Sex Educators, Counselors, Therapists) credentials and/or a marriage and family therapist who has experience with people with cancer 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 14 Ostomy Surgery: Interventions • Address issues of Body Image • Concerns about odor – Tight appliance – Avoid foods that cause flatulence or urinary odor (asparagus) • Appliance cover, lingerie • Ostomy accessories (search for “ostomates”) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 15 Interventions for Male Issues • Surgical Nerve-Sparing Techniques – Results depend on surgeon skill, pt age (better if <50yo, worse if >70yo), comorbidities – Both nerve bundles spared: 50-90% success – One bundle spared: 25-50% success – No nerves spared: >84% with impotence – More likely to have initial impotence, but regain function within 6 mos – 3 yrs – Early intervention with meds to prevent atrophy – Without prostate, can have orgasm / normal sensation, but no ejaculate/semen “dry orgasm” 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 16 Interventions for Female Issues • Vaginal lubricants – Use before/during sexual activity – Water soluble, water- or silicone-based – Petroleum-based can damage condoms and encourage vaginal infection • Vaginal Moisturizer – Replens: 3x a week, for a minimum of 3 months – Vaginal tissue regains moisture & elasticity – Use with lubricants, can also use Replens before intercourse 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 18 Interventions for Female Issues • Vaginal Estrogens – Creams: use 2-3x week – Causes elevated systemic estrogen (highest in first 3-4 mos), not good for breast cancer pts – E-string: silicone ring, slow release of local estrogen over three months – Vagifem: tablet inserted at night, QD for 2 weeks, then biweekly – Risk is thought to be low for breast cancer pts. With ring & tablets, but long term studies not done yet – Don’t confuse with Femring (a hormone replacement therapy)! 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 19 Radiation-Induced Vaginal Stenosis • Radiation for cervical and endometrial cancers, or to the pelvic region: risk for fibrosis / stenosis • Risk increases with brachytherapy • Decreased blood supply leads to dry, tender, less elastic tissue that may close off vagina • Women who are sexually active should be encouraged to remain active • Vaginal dilator with or without estrogen cream used 3 times a week for life (can substitute with intercourse). Start when radiation starts. • Educate on use and cleaning of dilator, give written instructions – also important for exam comfort (not just sexual activity), can start small and increase size of dilator 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 20 Other Interventions for Women • Eros device to increase blood flow to clitoris, use 3-4x a week. Increases sensitivity & lubrication with gentle vacuum • Sensua & Viagel – creams containing L-arginine (dilates blood vessels) & menthol applied to clitoris to increase blood flow • Viagra being tested in women 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 21 Resources • www.eyesontheprize.org (online community for gynecologic cancers) • Support groups (Gilda’s Club, Wellness Community) • www.oncolink.org • www.ustoo.org (prostate cancer website) • www.fertilehope.org • www.resolve.org (fertility) • ACS Sexuality booklets (available on ACS website) Pregnancy & Treatment • ~4% (50,000) of people diagnosed with cancer are under age 35 • Discuss importance of birth control use - for both sexes - during hormones, chemo, xrt • Condoms for 48 hrs after chemo (excreted in semen) • IUD, sponge, diaphragm – risk of infection if neutropenic, foams can irritate vaginal tissue • Should not conceive after treatment for ~1 yr for women, ~2 yrs for men • Data on risk for fetus exposed to chemo is limited and related to trimester (1st is greatest risk) • Drug choice, does it enter fetal circulation? • Delay radiation until after birth or use shielding • Use non-radiation tests (US, MRI), choose safe anesthesia 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 23 Risk of Infertility: Radiation • Small dose can = big damage • Temporary or permanent, can take up to 4 yrs to resume fertility: monitor FSH & sperm counts if desire pregnancy • Permanent sperm damage at 4 Gy, but Leydig cells need higher dose (20-30 Gy), so sexual characteristics can be unaffected • Oocytes related to pre-treatment pool size • >40 yrs old: 5-6 Gy; <40 yrs old: 20 Gy for permanent ovarian failure • <35 yrs old more likely to resume menstruation, but can still have premature menopause • TBI causes sterility in 80% men, 90% women • Cranial XRT affecting pituitary - may require supplemental hormones (testosterone, FSH) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 24 Radiation Risk to Future Pregnancy • Pelvic/ Uterine radiation • XRT in childhood results in changes in uterine musculature & blood flow, decrease in size (40% of normal size) • Spontaneous abortion: 38% vs. 12% (in the general public) • Preterm labor: 62% vs. 9% • Low birth weight: 62% vs. 6% • No increase in birth defects seen after XRT or chemo in men or women 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 25 Risk of Infertility: Chemo • Drug(s), dose, duration, and age of patient • Higher dose, longer duration, and older age pose highest risk • Alkalating agents most likely to cause infertility (don’t require cell proliferation to cause damage) • Stem cell / BMT (without TBI): infertility extremely likely in women, 50% of men • Women can regain menses and still have premature menopause (42% by age 31 vs. 5% of normal population) • Resumption of menses is no guarantee of fertility • Men can develop low/no sperm count with no damage to Leydig cells 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 26 Chemotherapy (dose to cause effect) Known Effect on Sperm Count Chlorambucil (1.4 g/m2) Cyclophosphamide (19 g/m2) Procarbazine (4 g/m2) Melphalan (140 mg/m2) Cisplatin (500 mg/m2) Prolonged or permanent azoospermia in 90% of men; platinum agents 50% BCNU (1 g/m2) CCNU (500 mg/m2) Azoospermia in adulthood if treated before puberty Busulfan (600 mg/M2) Ifosfamide (42 g/m2) BCNU (300 mg/m2) Nitrogen mustard Actinomycin D Azoospermia likely, and are often given with other highly sterilizing agents, adding to the effect Risk for Infertility: Surgery • • • • • • Orchiectomy (bilateral) Penectomy Prostate or bladder surgery damage Prostatectomy Hysterectomy Oopherectomy (bilateral) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 31 Options for fertility preservation in men • Sperm banking – only after puberty – $700-1500 for 1-3 donations/ 1-5 yrs storage – Although many men have poor quality sperm at diagnosis, new techniques can use it anyway (even just 1-2 samples) – No sex for 5 days prior, 24-48 hours between samples; Testicular aspirate if no semen • Intracytoplasmic sperm injection (ICSI) – Newer technique for fertilization, very successful • GnRH agonist/antagonists – “Turn off” gonads (only tested in mice, no births) • Cryopreservation of testicular tissue, then transplant or grow in vivo (+ births in mice) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 32 Options for Fertility Preservation in Women • Embryo freezing – cycle 12-14 days, 10-25% chance of pregnancy per embryo stored, cost $8-12,000, then cost of storage, thaw & implanting • Ovarian transposition (oophoropexy) – move ovaries from XRT field, can be laparoscopic, cost ?, been done for 30yrs, 16-90% success rate • Egg cryopreservation – cycle 12-14 days, 2% chance of live birth per thawed egg, cost ~$8,000, then cost of storage, thaw, fertilizing & implanting 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 33 Options for Fertility Preservation in Women • GnRH agonist/antagonist : theory is to stop proliferation – Suppress ovarian function via hypothalamic-pituitary access (some studies use birth control pills for same effect) – Experimental, studies +/-, large randomized study by SWOG ongoing • Ovarian tissue freezing: 60% follicles lost to freezing, have been 2 live births* – 5 laparoscopic biopsies can yield 3500 follicles – Transplant: auto* (orthotopic/heterotopic), xeno (mice), In Vitro Maturation (success in mice, cows) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 34 Options for Fertility Preservation in Women • Radical trachelectomy: for cervical cancer, experimental? – Remove cervix, leave uterus intact, permanent cerclage (stitch closed uterus) – Started in 1987, >100 live births, 53% chance of pregnancy over 5 years – High risk births (premature rupture of membranes) – about ½ premature delivery, all need c-section – Recurrence rates equivalent to radical hysterectomy – Only for early stage disease (IA & IB) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 35 Assessing Ovarian Function in Survivors • FSH & Estradiol – Check on 3rd day of menses – FSH >12mIU or E2 > 75pg/ml =severely impaired fertility (or poor ovarian reserve) – Levels effected by tamoxifen • Anti-Mullerian hormone (AMH) – Produced by early follicles, good predictor of reserve • Antral follicle count – Via ultrasound on 3rd day menses, not affected by tamoxifen – Count # developing follicles, is proportionate to # remaining 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 36 Financial Assistance • 11 states require insurance companies to cover infertility dx & tx (unless self-insured) (NJ, NY & MD) • www.resolve.org (has info for all states) • Check on extent of benefits, talk to HR representatives • Sharing Hope program thru Fertile Hope – sperm bank for $150 (1yr storage) (must meet requirements) • www.fertilehope.org – has many financial assistance links/tips • Rates vary greatly!! Shop around 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 37 Local Sites for Sperm Banking • 3 National organizations (by mail) – www.cryolab.com – www.reprot.com – www.xytextissues.com • • • • • Women’s Institute; 815 Locust / Plymouth Meeting Penn Fertility 3701 Market Fairfax Cryobank 3401 Market (http://www.fairfaxcryobank.com/) Drexel Fertility Bala Cynwyd / Center City Reproductive Science Institute Jenkintown (http://www.rsiinfertility.com/) • Women’s Health Group of PA Bryn Mawr 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 38 Local Sites for Women • Women’s Institute: 815 Locust / Plymouth Meeting (http://www.womensinstitute.org/) • Penn Fertility: 3701 Market (http://www.pennhealth.com/fertility) • Drexel Fertility: Bala Cynwyd / Center City (http://www.drexelfertility.medem.com) • Women’s Health Group of PA: Bryn Mawr (http://www.mainlinefertility.com) 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 39 References • Devita, VT, Hellman, S & Rosenberg, SA. Cancer: Principles & Practice of Oncology (7th edition). Lippincott Williams & Wilkins, Philadelphia, PA 2005. • Itano, JK & Taika, KN. Core Curriculum for Oncology Nursing (4th edition). Oncology Nursing Society 2005. • Krebs, L. & Marrs, JA. What Should I Say? Talking With Patients About Sexuality Issues. Clinical Journal of Oncology Nursing. 10 (3)313-315, 2006. • Lee SJ, Schover LR, Partridge AH, et al: American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. Journal of Clinical Oncology 24:2917-31, 2006 • Nieman CL, Kazer R, Brannigan RE, et al: Cancer survivors and infertility: a review of a new problem and novel answers. Journal of Supportive Oncology 4:171-8, 2006 • Simon B, Lee SJ, Partridge AH, et al: Preserving fertility after cancer. CA: A Cancer Journal for Clinicians 55:211-28; quiz 263-4, 2005 9/12/2006 OncoLink Copyright © Trustees of the University of Pennsylvania 40