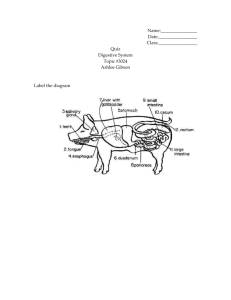
large intestine - Daniela Sartori
advertisement

Chapter 18 Lecture Outline Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Chapter 18 Outline Introduction to the Digestive System From Mouth to Stomach Small Intestine Large Intestine Liver, Gall Bladder, and Pancreas Neural and Endocrine Regulation of the Digestive System Digestion and Absorption of Carbohydrates, Lipids, and Proteins 18-2 Introduction to the Digestive System Inside gastrointestinal (GI) tract, food is broken down by hydrolysis into molecular monomers Absorption of monomers occurs in small intestine 18-3 18-4 Functions of GI Tract 18-5 Motility Is movement of food through GI tract by means of: Ingestion--taking food into mouth Mastication--chewing food and mixing it with saliva Deglutition--swallowing food Peristalsis--rhythmic wave-like contractions that move food through GI tract 18-6 Secretion Includes release of exocrine and endocrine products into GI tract Exocrine secretions include: HCl, H2O, HCO3-, bile, lipase, pepsin, amylase, trypsin, elastase, and histamine Endocrine includes hormones secreted into stomach and small intestine to help regulate GI system e.g. gastrin, secretin, CCK, GIP, GLP-1, guanylin, VIP, and somatostatin 18-7 Digestion Refers to breakdown of food molecules into smaller subunits Absorption Is passage of digested end products into blood or lymph 18-8 Storage and Elimination Includes temporary storage and subsequent elimination of indigestible components of food Immune Barrier Includes physical barrier formed by tight junctions between cells of small intestine And cells of the immune system that reside in connective tissue just below epithelium 18-9 Structure of Digestive System 18-10 Digestive System Is composed of GI tract (alimentary canal) and accessory digestive organs GI tract is 30 ft long; extends from mouth to anus 18-11 Digestive System continued Organs include oral cavity, pharynx, esophagus, stomach, and small and large intestine Accessory organs include teeth, tongue, salivary glands, liver, gallbladder, and pancreas 18-12 Layers of GI Tract Are called tunics The 4 tunics are mucosa, submucosa, muscularis, and serosa 18-13 Mucosa Is the absorptive and secretory layer lining lumen of GI tract In places is highly folded with villi to increase absorptive area Contains lymph nodules, mucus-secreting goblet cells, and thin layer of muscle 18-14 Submucosa Is a thick, highly vascular layer of connective tissue where absorbed molecules enter blood and lymphatic vessels Contains glands and nerve plexuses (submucosal plexus) that carry ANS activity to muscularis mucosae of small and large int. 18-15 Muscularis Is responsible for segmental contractions and peristaltic movement through GI tract Has an inner circular and outer longitudinal layer of smooth muscle Activity of these layers moves food through tract while pulverizing and mixing it Myenteric plexus between these layers is major nerve supply to GI tract Includes fibers and ganglia from both Symp and Parasymp systems 18-16 Serosa Is outermost layer; serves to bind and protect Consists of areolar connective tissue covered with layer of simple squamous epithelium 18-17 Regulation of GI Tract Parasympathetic effects, arising from vagus and spinal nerves, stimulate motility and secretions of GI tract Sympathetic activity reduces peristalsis and secretory activity GI tract contains an intrinsic system that controls its movements--the enteric nervous system GI motility is influenced by paracrine and hormonal signals 18-18 From Mouth to Stomach 18-19 From Mouth to Stomach Mastication (chewing) mixes food with saliva which contains salivary amylase An enzyme that catalyzes partial digestion of starch 18-20 From Mouth to Stomach continued Deglutition (swallowing) begins as voluntary activity Oral phase is voluntary and forms a food bolus Pharyngeal and esophageal phases are involuntary and cannot be stopped To swallow, larynx is raised so that epiglottis covers entrance to respiratory tract A swallowing center in medulla orchestrates complex pattern of contractions required for swallowing 18-21 From Mouth to Stomach continued Esophagus connects pharynx to stomach Upper third contains skeletal muscle Middle third contains mixture of skeletal and smooth Terminal portion contains only smooth Passes through diaphragm via esophageal hiatus 18-22 From Mouth to Stomach continued Peristalsis propels food thru GI tract = wave-like muscular contractions After food passes into stomach, the gastroesophageal sphincter constricts, preventing reflux 18-23 Stomach 18-24 Stomach Is most distensible part of GI tract Empties into the duodenum Functions in: storage of food; initial digestion of proteins; killing bacteria with high acidity; moving soupy food mixture (chyme) into intestine 18-25 Stomach continued Is enclosed by gastroesophageal sphincter on top and pyloric sphincter on bottom Is divided into 3 regions: Fundus Body Antrum 18-26 Stomach continued Inner surface of stomach is highly folded into rugae Contractions of stomach churn chyme, mixing it with gastric secretions Eventually these will propel food into small intestine 18-27 Stomach continued Gastric mucosa has gastric pits in its folds Cells that line folds deeper in the mucosa, are exocrine gastric glands 18-28 Stomach continued Gastric glands contain cells that secrete different products that form gastric juice Goblet cells secrete mucus Parietal cells secrete HCl and intrinsic factor (necessary for B12 absorption in intestine) Chief cells secrete pepsinogen (precursor for pepsin) 18-29 Stomach continued Enterochromaffin- like cells secrete histamine and serotonin G cells secrete gastrin D cells secrete somatostatin 18-30 HCl in Stomach Is produced by parietal cells which pump H+ into lumen via an H+/ K+ pump (pH ~1) Cl- is secreted by facilitated diffusion H+ comes from dissociation of H2CO3 Cl- comes from blood side of cell in exchange for HCO318-31 HCl in Stomach continued Is secreted in response to the hormone gastrin; and ACh from vagus These are indirect effects since both stimulate release of histamine which causes parietal cells to secrete HCl 18-32 HCl in Stomach continued Makes gastric juice very acidic which denatures proteins to make them more digestible Converts pepsinogen into pepsin Pepsin is more active at low pHs 18-33 Protection of Stomach Against HCL and Pepsin Both HCL and pepsin can damage lining and produce a peptic ulcer 1st line of defense is the adherent layer of mucus = a stable gel of mucus coating the gastric epithelium Contains bicarbonate for neutralizing HCL Is a barrier to actions of pepsin Gastric epithelial cells contain tight junctions to prevent HCL and pepsin from penetrating the surface Gastric epithelial cells are replaced every 3 days 18-34 Digestion and Absorption in Stomach Proteins are partially digested by pepsin Carbohydrate digestion by salivary amylase is soon inactivated by acidity Alcohol and aspirin are the only commonly ingested substances that are absorbed 18-35 Gastric and Peptic Ulcers Peptic ulcers are erosions of mucous membranes of stomach or duodenum caused by action of HCl In Zollinger-Ellison syndrome, duodenal ulcers result from excessive gastric acid in response to high levels of gastrin Helicobacter pylori infection is associated with ulcers Antibiotics are useful in treating ulcers And also proton pump inhibitors such as Prilosec Acute gastritis is an inflammation that results in acid damage due to histamine released by inflammation Is why histamine receptor blockers such as Tagamet and Zantac can treat gastritis 18-36 Small Intestine 18-37 Small Intestine (SI) Is longest part of GI tract; approximately 3m long Duodenum is 1st 25cm after pyloric sphincter Jejunum is next 2/5 of length Ileum is last 3/5 of length; empties into large intestine 18-38 Small Intestine (SI) continued Absorption of digested food occurs in SI Facilitated by long length and tremendous surface area 18-39 Small Intestine (SI) continued Surface area increased by foldings and projections Large folds are plicae circulares Microscopic fingerlike projections are villi Apical hair-like projections are microvilli 18-40 Small Intestine (SI) continued Each villus is covered with columnar epithelial cells interspersed with goblet cells Epithelial cells at tips of villi are exfoliated and replaced by mitosis in crypts of Lieberkuhn Inside each villus are lymphocytes, capillaries, and central lacteal 18-41 Small Intestine (SI) continued A carpet of hair-like microvilli project from apical surface of each epithelial cell Create a brush border 18-42 Intestinal Enzymes Attached to microvilli are brush border enzymes that are not secreted into lumen Enzyme active sites are exposed to chyme 18-43 Intestinal Contractions and Motility 2 major types of contractions occur in SI: Peristalsis is weak and slow and occurs mostly because pressure at pyloric end is greater than at distal end Segmentation is major contractile activity of SI Is contraction of circular smooth muscle to mix chyme (shown in diagram) 18-44 Intestinal Contractions and Motility continued Occur automatically via endogenous pacemaker activity Contractions are driven by graded depolarizations called slow waves 18-45 Intestinal Contractions and Motility continued Slow waves are produced by nonneuronal/nonmuscular cells called interstitial cells of Cajal (ICC) Have long processes joined to each other and to smooth muscle via gap junctions Spreads depolariz. from one cell to next 18-46 Intestinal Contractions and Motility continued When slow waves exceed threshold, trigger APs in smooth muscle by opening V-gated Ca2+ channels Influx of Ca2+ produces depolarization phase of AP and stimulates contraction Repolarization via K+ efflux Contractions are modified by ANS activity ACh from Parasymp increases amplitude and duration of slow waves Norepi and Epi from Symp decrease activity of intestines 18-47 Large Intestine 18-48 Large Intestine (LI) or Colon Has no digestive function but absorbs H2O, electrolytes, B and K vitamins, and folic acid Internal surface has no villi or crypts and is not very elaborate Contains large population of microflora = 1013 to 1014 commensal bacteria of 400 species which produce folic acid and vitamin K and ferment indigestible food to produce fatty acids And reduce ability of pathogenic bacteria to infect LI antibiotics can negatively affect commensals 18-49 Large Intestine (LI) or Colon continued Extends from ileocecal valve at end of SI to anus Outer surface bulges to form pouches (haustra) Chyme from SI enters cecum, then passes to ascending colon, transverse colon, descending colon, sigmoid colon, rectum, and anal canal 18-50 Fluid and Electrolyte Absorption in LI SI absorbs most water but LI absorbs 90% of water it receives Begins with osmotic gradient set up by Na+/K+ pumps Water follows by osmosis Salt and water reabsorption stimulated by aldosterone LI can also secrete H2O via active transport of NaCl into intestinal lumen 18-51 Defecation After electrolytes and water have been absorbed, waste material passes to rectum, creating urge to defecate Defecation reflex begins with relaxation of the external anal sphincter allowing feces to enter anal canal Longitudinal rectal muscles contract to increase rectal pressure; internal anal sphincter relaxes Excretion is aided by contractions of abdominal and pelvic muscles which push feces from rectum 18-52 Liver 18-53 Structure of Liver Liver is the largest internal organ Hepatocytes form hepatic plates that are 1–2 cells thick Plates are separated by sinusoids which are fenestrated and permeable even to proteins Contain phagocytic Kupffer cells 18-54 Structure of Liver continued A damaged liver can regenerate itself from mitosis of surviving hepatocytes In some cases, such as alcohol abuse or viral hepatitis, regeneration does not occur Can lead to liver fibrosis and ultimately cirrhosis 18-55 Hepatic Portal System Food absorbed in SI is delivered 1st to liver Capillaries in digestive tract drain into the hepatic portal vein which carries blood to liver Hepatic vein drains liver Liver also receives blood from the hepatic artery 18-56 Liver Lobules Are functional units formed by hepatic plates In middle of each is central vein At edge of each lobule are branches of hepatic portal vein and artery which open into sinusoids 18-57 Liver Lobules continued Bile is secreted by hepatocytes in bile canaliculi Empty into bile ducts which flow into hepatic ducts that carry bile away from liver 18-58 Enterohepatic Circulation Is recirculation of compounds between liver and intestine Many compounds are released in bile, reabsorbed in SI, and returned to liver to be recycled Liver excretes drug metabolites into bile to pass out in feces 18-59 18-60 Bile Production and Secretion Amounts to 250–1500 ml/day Bile pigment (bilirubin) is produced in spleen, bone marrow, and liver Is a derivative of heme groups (minus iron) from Hb Carried in blood attached to albumin Free bilirubin combines with glucuronic acid to form conjugated bilirubin that is secreted into bile Converted by intestinal bacteria to urobilinogen 30-50% of urobilogen is absorbed by intestine and enters hepatic vein Thus enters enterohepatic circulation to be recycled or filtered by kidneys and excreted in urine 18-61 Metabolism of Heme and Bilirubin 18-62 Bile Acids Are formed in major breakdown pathway for cholesterol Are mostly cholic and chenodeoxycholic acids Form bile salts by combining with glycine or taurine Bile salts aggregate as micelles 95% of bile acids are absorbed by ileum 18-63 Detoxication of Blood Liver can remove hormones, drugs, and other biologically active molecules from blood by: Excretion into bile Phagocytosis by Kupffer cells Chemical alteration of molecules e.g. ammonia is produced by deamination of amino acids in liver Liver converts it to urea which is excreted in urine 18-64 Detoxification of Blood continued Liver conjugates steroid hormones and xenobiotics with groups that make them anionic Which can be transported into bile or urine by multispecific organic anion transport carriers and excreted Cytochrome P450 enzymes are involved in hepatic metabolism of steroids and drugs Stim. by activation of nuclear receptors =SXR (steroid and xenobiotic receptor 18-65 Secretion of Glucose, Triglycerides and Ketones Liver helps regulate blood glucose by removing it from blood or releasing it to blood Removes it via glycogenesis and lipogenesis Or produces it via glycogenolysis and gluconeogenesis Can convert free fatty acids into ketone bodies (ketogenesis) that can be used for energy during fasting 18-66 Production of Plasma Proteins Albumin and most of plasma globulins are produced by liver Albumin makes up 70% of total plasma protein and contributes most of the colloid osmotic pressure of blood Globulins transport cholesterol, triglycerides, steroid and thyroid hormones, inhibit trypsin, and are involved in blood clotting Clotting factors I, II, V, VII, IX, and XI as well as angiotensinogen all prod. by liver 18-67 Gallbladder and Pancreas 18-68 Gallbladder Is a sac-like organ attached to inferior surface of liver Stores and concentrates bile continuously produced by liver When SI is empty, sphincter of Oddi in common bile duct closes and bile is forced into gallbladder Expands as it fills with bile When food is in SI, sphincter of Oddi opens, gall bladder contracts, and bile is ejected thru cystic duct into common bile duct then to duodenum 18-69 Pancreas Is located behind stomach Has both endocrine and exocrine functions Endocrine function performed by islets of Langerhans Secretes insulin and glucagon Exocrine secretions include bicarbonate solution and digestive enzymes These pass in pancreatic duct to SI Exocrine secretory units are acini 18-70 Pancreatic juice and bile are secreted into the duodenum 18-71 The Pancreas is Both an Exocrine and Endocrine Gland (a) A photomicrograph of the endocrine and exocrine portions of the pancreas (b) An illustration depicting the exocrine acini, where acinar cells prod. Inactive enzymes stored as zymogen granules which are secreted via ducts into duodenum 18-72 Pancreatic Juice Contains water, bicarbonate, and digestive enzymes Digestive enzymes include amylase for starch, trypsin for proteins, and lipase for fats Brush border enzymes are also required for complete digestion 18-73 The Activation of Pancreatic Juice Enzymes Most pancreatic enzymes are produced in inactive form (zymogens) Trypsin is activated by brush border enzyme, enterokinase Trypsin in turn activates other zymogens 18-74 18-75 Neural and Endocrine Control of the Digestive System 18-76 Neural and Endocrine Regulation Neural and endocrine mechanisms modify activity of GI system Vagus nerve is heavily involved in regulating and coordinating digestive activities GI tract is both an endocrine gland and target for action of hormones Hormones include secretin, gastrin, CCK, and GIP 18-77 Regulation of Gastric Function Gastric motility and secretion occur automatically Waves of contraction are initiated spontaneously by pacesetter cells and secretion occurs in absence of hormonal and neural input ANS and hormonal effects are superimposed on automatic activity Extrinsic control of gastric function is divided into cephalic, gastric, and intestinal phases 18-78 Cephalic Phase Refers to control by brain of vagus activity Stimulated by sight, smell, and taste of food Activation of vagus: Stimulates chief cells to secrete pepsinogen Directly stimulates G cells to secrete gastrin Directly stimulates ECL cells to secrete histamine Indirectly stimulates parietal cells to secrete HCl Continues into 1st 30 min of a meal 18-79 Gastric Phase Distention of stomach stim. vagus nerve Vagus nerve stim. acid secretion Amino acids and peptides in stomach lumen stim. acid secretion Direct stim. of parietal cells Stim. of gastrin secretion; gastrin stim. acid secretion Gastrin secretion inhibited by when pH of gastric juice falls below 2.5 18-80 Gastric Phase continued Short polypeptides and amino acids stimulate G cells to secrete gastrin and chief cells to secrete pepsinogen Gastrin stimulates ECL cells to secrete histamine which stimulates parietal cell secretion of HCl This is a positive feedback mechanism: As more HCl and pepsinogen are secreted, more polypeptides and amino acids are released 18-81 Gastric Phase continued Secretion of HCl is also regulated by a negative feedback mechanism: HCl secretion decreases if pH < 2.5; at pH 1 gastrin secretion stops D cells stimulate secretion of somatostatin which inhibits gastrin secretion 18-82 Intestinal Phase Begins when chyme enters the SI and inhibits gastric activity Arrival of chyme in SI is detected by sensory neurons of vagus This causes a neural reflex that inhibits gastric motility and secretion Fat in chyme stimulates SI to secrete enterogasterones-hormones that inhibit gastric motility and secretion Enterogasterones include somatostatin, GIP, CCK, and GLP-1 GIP and GLP-1 stimulate insulin secretion in anticipation of glucose entering blood from digestion 18-83 Enteric Nervous System ENS organized into ganglia interconnected by 2 plexuses: Outer myenteric (Auerbach’s) plexus found along entire length of GI tract Inner submucosal (meissner’s plexus) located only in small and large intestine ENS contains 100 million neurons and similar diversity of neurotransmitters as CNS Has interneurons, sensory, autonomic, and glia Peristalsis is controlled by enteric NS 18-84 Enteric Nervous System continued For peristalsis: ACh and substance P stimulate smooth muscle contraction above bolus NO, VIP, and ATP stimulate smooth muscle relaxation below bolus 18-85 Paracrine Regulators of Intestine ECL cells release serotonin and motilin in response to pressure and chemical stimuli in SI Serotonin stimulates intrinsic afferents which activate motor neurons in intrinsic NS Motilin stimulates contraction in duodenum and stomach antrum Guanylin, from ileum and colon, stimulates production of cGMP which inhibits absorption of Na+and causes secretion of Cl- and H2O Uroguanylin found in urine---appears to be prod. by intestines and may function as hormone that stim. kidneys to excrete salt in urine 18-86 Intestinal Reflexes Can be mediated by enteric NS and paracrines; and regulated by ANS and hormones Gastroileal reflex refers to increased motility of ileum and movement of chyme thru ileocecal sphincter in response to increased gastric activity Ileogastric reflex decreases gastric motility in response to distension of ileum Intestino-intestinal reflex causes relaxation of rest of intestine when any part is overdistended 18-87 Secretion of Pancreatic Juice Secretion of pancreatic juice is stimulated by secretin and CCK (cholecystokinin) Secretin is secreted in response to duodenal pH < 4.5 Stimulates release of HCO3- into SI by pancreas CCK is secreted in response to fat and protein content of chyme in duodenum Stimulates production of pancreatic enzymes Enhances secretin Stimulates contraction of sphincter of Oddi 18-88 Digestion and Absorption of Carbohydrates, Lipids, and Proteins 18-89 The Action of Pancreatic Amylase Most carbohydrates are ingested as starch-a polymer of glucose Salivary amylase begins starch digestion Pancreatic amylase converts starch to oligosaccharides Oligosaccharides hydrolyzed by SI brush border enzymes 18-90 Digestion and Absorption of Protein Begins in stomach when pepsin digests proteins to form polypeptides In SI, the pancreatic juice enzymes endopeptidases (trypsin, chymotrypsin, elastase) cleave peptide bonds in interior of polypeptides SI exopeptidases (carboxypeptidase -pancreatic juice and aminopeptidase- brush border enzyme) cleave peptide bonds from ends of polypeptides Results in free amino acids, dipeptides, and tripeptides Free amino acids absorbed by cotransport with Na+ into epith. cells and secreted into blood caps. Di- and tripeptides carried into epith. cell where hydrolyzed into free amino acids then secreted 18-91 Digestion and Absorption of Protein continued Protein digestion in SI results in free amino acids, dipeptides, and tripeptides Which are transported into SI cells where diand tripeptides are broken down to amino acids Which are secreted into blood 18-92 Digestion and Absorption of Lipids Occurs in SI Arrival of lipids in duodenum causes secretion of bile Fat is emulsified by bile salt micelles Forms tiny droplets of fat dissolved in bile salt micelles Greatly increases surface area for fat digestion 18-93 Digestion of Triglycerides Pancreatic lipase hydrolyzes triglycerides to free fatty acids and monglycerides Phospholipase A breaks down phospholipids into fatty acids and lysolecithin 18-94 Fat Digestion and Emulsification Products of fat digestion dissolve in micelles forming mixed micelles which move to brush border 18-95 The Absorption of Fat Free fatty acids, monoglycerides, and lysolecithin leave micelles and enter epithelial cells Inside epithelial cells, they are resynthesized into triglycerides and phospholipids 18-96 Digestion and Absorption of Lipids continued Triglycerides and phospholipids combine with a protein to form small particles called chylomicrons Which are secreted into central lacteals of SI villi 18-97 Transport of Lipids In blood, chylomicrons combine with apolipoprotein Which allows them to bind to receptors on capillaries in muscle and fat There endothelial lipoprotein lipase hydrolyzes the triglycerides to free fatty acids and glycerol for energy use by muscle and storage in fat Cholesterol-containing remnants are taken up by liver 18-98 Transport of Lipids continued Cholesterol and triglycerides from liver form VLDLs which are secreted and take triglycerides to cells Once triglycerides are removed, VLDLs become LDLs LDLs transport cholesterol to organs and blood vessels HDLs transport excess cholesterol back to liver High ratio of HDL-cholesterol to total cholesterol is believed to confer protection against atherosclerosis 18-99