Brophy-Citrate - Pediatric Continuous Renal Replacement
advertisement

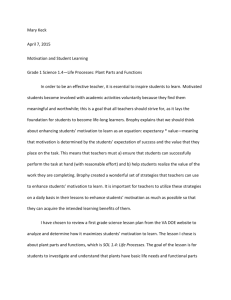
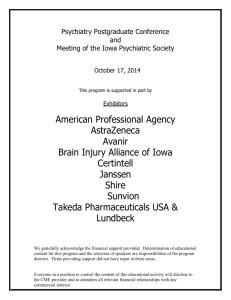
Citrate Anticoagulation Patrick Brophy MD, MHCDS Professor & Director Pediatric Nephrology University of Iowa- Children’s Hospital London 2015 Brophy University of Iowa Objectives Review rationale for anticoagulation Options Available data Brophy University of Iowa Relevance to CRRT Functional circuit life is imperative to: Dose delivery Staff statisfaction Patient morbidity (changing lines) Cost of therapy—multi circuit use Brophy University of Iowa Optimal Anticoagulation Should be: Readily available Consistently delivered (protocols) Safe!!!! Easily monitored Commercially available Be associated with minimal side effects Brophy University of Iowa Anticoagulants Saline Flushes Heparin Peds Citrate regional anticoagulation Peds Low molecular weight heparin Prostacyclin Nafamostat mesilate Danaparoid* Hirudin/Lepirudin Argatroban (thrombin inhibitor)* * No antidote known Brophy University of Iowa Brophy University of Iowa Sites of Thrombus Formation Any blood surface interface Hemofilter Bubble trap Catheter (Especially Pediatrics) Areas of turbulence resistance Luer lock connections / 3 way stopcocks Brophy University of Iowa Citrate Brophy University of Iowa How does citrate work Clotting is a calcium dependent mechanism, removal of calcium from the blood will inhibit clotting Adding citrate to blood will bind the free calcium (ionized) calcium in the blood thus inhibiting clotting Common example of this is blood banked blood Brophy University of Iowa Calcium Dependent Pathways CITRATE Brophy University of Iowa How is citrate used? In most protocols citrate is infused post patient but prefilter often at the “arterial” access of the dual (or triple) lumen access that is used for hemofiltration (HF) Calcium is returned to the patient independent of the dual lumen HF access or can be infused via the 3rd lumen of the triple lumen access Brophy University of Iowa (Citrate = 1.5 x BFR 150 mls/hr) (Ca = 0.4 x citrate rate 60 mls/hr) (8mg/ml) Pediatr Neph 2002, 17:150-154 (BFR = 100 mls/min) Replacement Fluid Dialysate Brophy University of Iowa Calcium can be infused in 3rd lumen of triple lumen access if available. Citrate: Technical Considerations Measure patient and system iCa in 2 hours then at 6 hr increments Pre-filter infusion of Citrate Aim for system iCa of 0.3-0.4 mmol/l Adjust for levels Systemic calcium infusion Aim for patient iCa of 1.1-1.3 mmol/l Adjust for levels Brophy University of Iowa Citrate: Advantages No need for heparin Commercially available solutions exist (ACDcitrate-Baxter) Less bleeding risk Simple to monitor Many protocols exist Brophy University of Iowa Advantages of Citrate Has zero effect upon patient bleeding as opposed to heparin which effects system and patient bleeding Easy to monitor with ionized calcium assay Activated Clotting Time (ACT) nor PTT needed Programs report less clotted circuits = less disposable cost and less overtime nursing hours Bedside surveys demonstrate less work of machinery allowing more attention to patient Brophy University of Iowa Citrate: Problems Metabolic alkalosis Metabolized in liver / other tissues May be associated with post CRRT raclcitrant hypercalcemia Electrolyte disorders Hypernatremia Hypocalcemia Hypomagnesemia Cardiac toxicity Neonatal hearts Brophy University of Iowa Complications of Citrate: Metabolic alkalosis Metabolic alkalosis due to citrate conversion to HCO3 Solutions with 35 meq/l HCO3 NG losses TPN with acetate component Treatment Solutions with 35 meq/l HCO3 Decrease bicarbonate dialysis rate and replace at the same rate with NS (pH 5) NG losses Replace with ½-2/3 NS TPN with acetate component Use high Cl ratio Brophy University of Iowa Complications of Citrate: “Citrate Lock” Seen with rising total calcium with dropping/Stable patient ionized calcium Essentially delivery of citrate exceeds hepatic metabolism and CRRT clearance Treatment of “citrate lock” Decrease or stop citrate for 1 hr then restart at 70% of prior rate or Increase D or FRF rate to enhance clearance Brophy University of Iowa Citrate or Heparin: literature Brophy University of Iowa Hoffbauer R et al. Kidney Int. 1999;56:1578-1583. Citrate Unfractionated Heparin Brophy University of Iowa Anticoagulation In adults: Monchi M et al. Int Care Med 2004;30:260-65 Median filter life was 70 hr Citrate, 40 hr Heparin Fewer PRBC transfused in Citrate group (surrogate of bleeding per study) 0.2 units/day of CVVH Citrate vs 1 units/day of CVVH Heparin Brophy University of Iowa Heparin or Citrate? . single center - 209Nephron adults Clin Pract. 2004; 97(4):c131-6. Morgera S, et.al. regional anticoagulation : trisodium citrate vs standard heparin protocol ( customized calcium-free dialysate) CitACG was the sole anticoagulant in 37 patients, 87 patients received low-dose heparin plus citrate, and 85 patients received only hepACG. Both groups receiving citACG had prolonged filter life when compared to the hepACG group. significant cost saving due to prolonged filter life when using citACG. Brophy University of Iowa Seven ppCRRT centers 138 patients/442 circuits 3 centers: hepACG only 2 centers: citACG only 2 centers: switched from hepACG to citACG HepACG = 230 circuits CitACG= 158 circuits NoACG = 54 circuits Circuit survival censored for Scheduled change Unrelated patient issue Death/witdrawal of support Regain renal function/switch to intermittent HD Brophy University of Iowa Brophy University of Iowa ppCRRT ACG Side Effects Heparin 11 cases of systemic bleeding on heparin 5 cases no ACG used secondary to bleeding 1 case of HIT Citrate 19 cases of metabolic alkalosis 1 change to heparin for hyperglycemia 1 change to heparin for alkalosis 3 cases of citrate lock Brophy University of Iowa Anticoagulation and CRRT Heparin and citrate anticoagulation most commonly used methods Heparin: bleeding risk Citrate: alkalosis, citrate lock Brophy University of Iowa Reference Tools Adqi.net-web site for information on CRRT AKIN.org Crrtonline.com-web site for info on Dr Mehta’s meeting www.PCRRT.com Pediatric CRRT with links to other meetings, protocols, industry PCRRT list serve (contact Tim Bunchman) Brophy University of Iowa Thanks ppCRRT members Bedside ICU and Dialysis Nurses patients Brophy University of Iowa