Gas Monitoring - Pheonix India

Gas Monitoring
Presented by: Dr. Meenal Aggarwal
Moderator: Dr. Dara Negi
Definitions
• Delay time: Time to achieve 10% of a step change in reading at the gas monitor
• Rise time/response time: Time required for a change from 10% to
90% of the total change in a gas value
• Total system response time: DT + RT
Monitor types
• 2 types: sidestream (diverting) or mainstream (nondiverting)
Mainstream:
• Sensor located directly in the gas stream (only for oxygen and CO
2
)
• Carbon dioxide: Using infrared technology with the sensor located between the breathing system and the patient
• Also available for the non-intubated patient: sensor attaches to a disposable oral and nasal adaptor
• Oxygen sensor: Uses electrochemical technology
Usually placed in the breathing system inspiratory limb.
Can measure both inspired and exhaled oxygen
Mainstream Infrared
CO 2 Analyser
• Advantages:
Fast response times, no delay time (waveform has better fidelity)
No gas is removed from the breathing system, so not necessary to scavenge these devices or to increase the fresh gas flow
Water and secretions rarely cause a problem (although secretions on the windows of the cuvette can cause erroneous readings: problem with CO
2 sensor)
Sample contamination by fresh gas is less likely
Standard gas is not required for calibration (Oxygen sensor: calibrated by using room air)
Use fewer disposable items than diverting monitors
• Disadvantages:
Adaptor placed near the patient: cause traction/ weight
Dead space
Leaks, disconnections, circuit obstructions
Condensed water, secretions, blood on the windows of the cuvette interferes with light transmission
Sensor may become dislodged from the cuvette
Expensive, vulnerable to damage
Available only for oxygen and CO
2
CO
2 sensor must be cleaned and disinfected between uses (potential for cross contamination), disposable become expensive
Prolonged contact of the CO
2 sensor assembly with the patient could cause pressure injury
Sidestream:
• Aspirates gas from the sampling site, sensor (located in the main unit)
• Sampling tube: short- decreases delay time and more satisfactory waveforms
• Usually zeroed using room air and calibrated using a gas of known composition
• Traps, filters and hydrophobic membranes
• Water droplets and secretions may increase resistance/ affect the accuracy
• Clear or purge the sample line, or tube may be changed
• Accuracy at 20-40 bpm and short length, > 40 bpm decreases accuracy
• Sampling flow rate: less than 150 mL/minute should not be used.
Elevated baseline, falsely low peak readings on lower flows
Devices used:
• Face mask: Large dead space relative to tidal volume, difficult to obtain accurate end-tidal values
can be attached to upper lip or placed in patient's nares or the lumen of an oral or nasopharyngeal airway under the mask
With a breathing system, most often attached to a component between the mask and the breathing system
• Tracheal Tube: Sampling site must be between the patient and the breathing system (measurement for both exp and insp)
Sampling site should be away from the fresh gas port (in mapleson circuits can l/t errors)
Tracheal tubes that incorporate a sampling lumen that extends to the middle or patient end of the tube are available
Tracheal tube connectors with an attachment or hole for a sampling tube are available or can be created
• Supraglottic devices: sampling tube can be inserted through the connector (preferred site is the distal end of the shaft)
may be inserted into a nasal airway
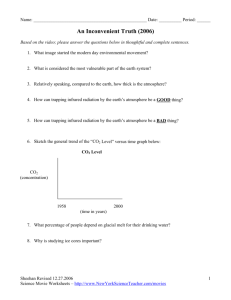
• Oxygen Supplementation Devices:
OxyArm: allow simultaneous administration of oxygen and carbon dioxide monitoring
In both nose and mouth breathers
A nasal cannula can be modified to accept a sampling tubing (may l/t choking hazard)
Sampling tube may be connected to mask outlet, inserted through a vent hole or a slit in the mask
Accuracy affected by: Mouth breathing, airway obstruction, and oxygen delivery through the ipsilateral nasal cannula
OxyArm
• Jet Ventilation: an injector incorporating a sampling lumen or a sampling tube placed in the airway may be used
Ventilatory frequency may need to be lowered to measure the endtidal CO
2
• Other ways:
Sampling line can be placed in front of or inside the patient's nostril
In mouth breather: in the nasopharynx or hypopharynx
Catheter placed in the trachea after extubation for CO
2 monitoring
Bite block can be modified to accommodate a sampling line
Sampling line can be placed over a tracheostomy stoma
• Advantages of Diverting devices:
Calibration and zeroing usually automatic (Occasional calibration is necessary, usually easy)
Added dead space is minimal.
Potential for cross contamination between patients low.
Several gases can be measured simultaneously, allows automatic correction for nitrous oxide and oxygen.
Sampling port can be used to administer bronchodilators
These devices can be used when the monitor must be remote from the patient (e.g., during MRI)
• Disadvantages of Diverting devices:
Leaks, sampling tube obstruction, or failure of the aspirator pump or can kink (use elbow connector)
Sampling line can be connected to the wrong place
Leak in sampling line can l/t mixing with air and so dilution of sample
Aspirated gases must be either routed to the scavenging system (need to inc fresh gas flow) or returned to the breathing system
Some delay time
Supply of calibration gas
Disposable items (adaptors and catheters) used
Fresh gas dilution
More variable differences between arterial and end-tidal CO
2 level
Technologies
• Infrared Analysis
Black body Radiation technology
Microstream technology
• Paramagnetic oxygen analysis
• Electrochemical oxygen analysis
Galvanic cell
Polarographic electrode
• Peizoelectric Analysis
• Refractometry
Infrared Analysis:
• Most common technology in use
• Principle: Gases with two or more dissimilar atoms in the molecule
(nitrous oxide, CO
2
, and the halogenated agents) have specific and unique infrared light absorption spectra.
• Amount of infrared light absorbed is proportional to the concentration of the absorbing molecules, the concentration can be determined
• Nonpolar molecules cannot be measured
• 2 technologies available:
Black body radiation
Microstream technology
Blackbody Radiation Technology:
• Utilizes a heated element called a blackbody emitter as the source of infrared light, produces a broad infrared spectrum (redundant radiation to be removed using filters)
• Optical detectors must be calibrated to recognize only infrared radiation that is modulated at a certain frequency by using a spinning chopper wheel
• Analyzer selects the appropriate infrared wavelength, minimize absorption by other gases that could interfere with measurement of the desired component
• Then an electrical signal is produced and amplified, and the concentration is displayed
• For halogenated agents: separate chamber to measure absorption at several wavelengths (single-channel, four-wavelength infrared filter photometers) have filter for each anesthetic agent and one to provide a baseline for comparison
Diverting type:
• Gas to be measured is pumped continuously through a measuring chamber
• Filtered and pulsed light is passed through the sample chamber and also through a reference chamber (has no absorption characteristics)
• Light is focused on an infrared photosensor (partly absorbed by the sample gas acc to conc)
• Changing light levels on the photosensor produce changes in the electrical current running through it
• Provides hundreds of readings for each respiratory cycle (Continuous waveform produced)
• Monochromatic analyzers use one wavelength to measure potent inhalational agents (unable to distinguish between agents)
• Polychromatic analyzers use multiple wavelengths to both identify and quantify the various agents
• Measuring cell is calibrated to zero (using gas that is free of the gases of interest, usually room air) and to a standard level (using a calibration gas mixture)
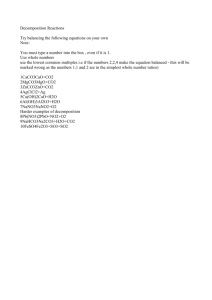
Non Diverting Type:
• Gas stream passes through a chamber (cuvette) with two windows, placed b/w the breathing system and the patient
• Sensor (has both the light source and detector) fits over the cuvette
• Sensor is heated slightly above body temperature (to prevent condensation)
• Infrared light passes through window on one side of the adaptor, sensor receives the light on the opposite side
• Then light goes through three ports in a rotating wheel, containing
(a) a sealed cell with a known high CO
2 concentration
(b) a chamber vented to the sensor's internal atmosphere
(c) a sealed cell containing only nitrogen
• Then passes through a filter (to isolate CO
2 information)
• Signal amplified and sent to the display module
• Calibration done using: low calibration cell contains 100% nitrogen, high cell contains a known partial pressure of CO
2
• Corrections for nitrous oxide and oxygen entered manually
Infrared Mainstream Analyser
Microstream Technology:
• Uses laser-based technology to generate infrared rays that match the absorption spectrum of CO
2
• Smaller sample cell, low flow rate
• Emission source: Glass discharge lamp coupled with an infrared transmitting window
• Electrons (generated by a radio frequency voltage) excite nitrogen molecules Carbon dioxide molecules are excited by collision with the excited nitrogen molecules These drop back to their ground state and emit the signature wavelength of CO
2
• This emission now passes through main optical detector and reference detector (compensates for changes in infrared output)
• Measurements made every 25 msec
• As low sample flow and small sample cell, useful for measuring:
CO
2 in very small patients
high respiratory rates
low-flow applications
unintubated patients
• Readings not affected by high concentrations of oxygen or anesthetic gases
Advantages of Infrared Analysis:
• Multigas Capability
• Volatile Agent Detection
• Small, compact, lightweight
• Quick response times (faster for CO
2
)
• Short warm-up time
• Convenience (no complicated calibrations)
• Lack of interference from other gases (argon, low conc NO)
• Detecting anaesthetic agent breakdown (desflurane to CO will show as wrong or mixed agent)
Disadvantages of Infrared Analysis:
• O
2 and N
2 cannot be measured
• Gas interference :
O
2 causes broadening of CO
2 spectrum l/t lower readings
N
2
O absorption spectrum overlaps with CO
2
(l/t higher vlues): so need either automatic or manual correction for N
2
O
He l/t underestimation of CO
2
• Other substances l/t inaccuracies (ethanol, methanol, diethyl ether, methane): give high volatile agent reading, polychromatic less affected
• Water vapors: Absorb infrared rays (l/t lower values), use water traps, hydrophobic membranes
• Slow response time (with rapid resp rates)
• Difficulty in adding new volatile agents
Paramagnetic Oxygen Analysis:
• Paramagnetic substances: Substances which locate themselves in the strongest portion of the field when introduced into a magnetic field
• Oxygen is paramagnetic
• Principle: When a gas that contains oxygen is passed through a switched magnetic field, the gas will expand and contract, causing a pressure wave that is proportional to the oxygen partial pressure
• Pressure difference is detected by the transducer and converted into an electrical signal that is displayed as oxygen partial pressure or volumes percent.
• Short rise time so both inspired and end-tidal oxygen levels can be measured
• Desflurane disturbs the paramagnetic oxygen sensor and it reads higher than expected
Eletrochemical Oxygen Analysis:
• Consists of a sensor, analyzer box, display, and alarms
• Sensor: A cathode and an anode surrounded by electrolyte
• Sensor is placed in the inspiratory limb
• Gel held in place by a membrane (nonpermeable to ions, proteins, but is permeable to oxygen)
• Older ones respond slowly to changes in oxygen pressure, so cannot be used to measure end-tidal concentrations (not so with new analyzers)
• Technology:
Galvanic cell/ fuel cell
Polarographic electrode
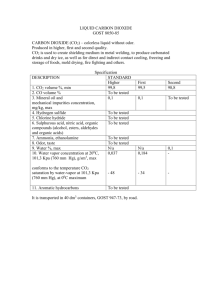
Galvanic cell:
• Principle: Oxygen diffuses through the sensor membrane and electrolyte to the cathode, where it is reduced, causing a current to flow
• Current generated is proportional to the partial pressure of oxygen in the gas
Cathode: O
2
+ 2H
2
O + 4e → 4OH -
Anode: 4OH + 2Pb → 2PbO + 2H
2
O + 4e -
• Cathode is the sensing electrode, anode is usually consumed
• The current is strong enough to operate the meter so a separate power source is not required to operate the analyzer
.
• The chemical reaction is temperature dependent (a thermistor may be connected in parallel with the sensor.)
Galvanic cell
Fuel cell Oxygen Analyzer
• Sensor comes packaged in a sealed container that does not contain oxygen
• Its useful life is cited in percent hours: the product of hours of exposure and oxygen percentage
• Sensor life can be prolonged by removing it from the breathing system and exposing it to air when not in use
• Whole sensor cartridge must be replaced when it becomes exhausted
Polarographic Electrode:
• Components: anode, a cathode, an electrolyte, and a gas-permeable membrane
• Needs power source for inducing a potential between the anode and the cathode
• Same principle as galvanic cell
• May be either preassembled disposable cartridges or units that can be disassembled and reused by changing the membrane and/or electrolyte
Advantages:
Easy to use, low cost, compact
No effect of argon
Disadvantages:
Maintenance (more in polarographic)
Need to be calibrated every day (every 8 hrs)
Slower response time
Peizoelectric Analysis:
• Uses vibrating crystals that are coated with a layer of lipid to measure volatile anesthetic agents
• Principle: When exposed to a volatile anesthetic agent, the vapor is adsorbed into the lipid resulting change in the mass of the lipid alters the vibration frequency
• By using an electronic system consisting of two oscillating circuits, one has an uncoated (reference) crystal and the other a coated (detector) crystal, an electric signal that is proportional to the vapour concentration is generated
• Diverting devices
Advantages:
Accuracy
Fast response time
No need for scavenging
Short warm up time
Compact
Disadvantages:
Only one gas measured
No agent discrimination
Inaccuracy with water vapours
Chemical Carbon Dioxide Detection
• Consists of a pH-sensitive indicator
• Principle: When the indicator is exposed to carbonic acid that is formed as a product of the reaction between CO
2 and water it becomes more acidic and changes color
Technology:
Hygroscopic
Hydrophobic
Uses:
• For confirming tracheal intubation when a capnometer is not available
• Disposable so it may be useful to confirm tracheal intubation in patients with respiratory diseases (e.g.SARS)
Advantages:
• Easy to use, small size, low cost
• Not affected by N
2
O, volatile anaesthetics
• Offers minimal resistance to flow
• CO doesn’t interfere
Disadvantages:
• Recommended to wait six breaths before making a determination
• False-negative results may be seen with very low tidal volumes
• Drugs instilled in the trachea or gastric contents can cause irreversible damage to the device
• False-positive results can occur if CO
2 in the stomach
• Semiquantitative, cannot give accurate measurement of CO
2
(So use limited to check endotracheal intubation)
Refractometry:
• Optical interference refractometer (interferometer): Light beam passes through a chamber into which the sample gas has been aspirated, also passes through an identical chamber containing air.
• Vapour slows the velocity of light, the portion passing through the vapor chamber is delayed
• Beams form dark and light bands, position of these bands yields the vapor concentration
• Used primarily for vaporizer calibration
• Sensitive to nitrous oxide (so cannot be used to measure halogenated agents in a O
2
, N
2
O, agent mixture)
Gas Measurement
Oxygen:
• Standard requirements:
Oxygen readings shall be within ±2.5% of the actual level (min for 6hrs together)
The high and low oxygen level alarms must be at least medium priority, oxygen concentration below 18% (should be high priority alarm)
It shall not be possible to set the low oxygen alarm limit below 18%
• Technology used:
Electrochemical Technology
Paramagnetic Technology: Rapid response time, even for nonintubated
Applications of Oxygen Analysis:
•
Detecting Hypoxic or Hyperoxic Mixtures:
Oxygen monitor provides earlier warning of inadequate oxygen than pulse oximetry
Problems resulting from hyperoxygenation: patient movement during surgery, awareness, damage to the lungs and eyes, fires
•
Detecting Disconnections and Leaks:
However not dependable
•
Detecting Hypoventilation:
Normal: Difference b/w inspired and expired oxygen is 4% to 5%
•
End tidal Oxygen Measurement:
Assess pt’s oxygen consumption (Malignant hyperthermia)
To detect air embolism (inc ET O
2
)
Carbon Dioxide Analysis:
• Means for assessing metabolism, circulation, and ventilation
• ASA guidelines: Correct positioning of ET tube must be verified by identifying CO
2 in the expired gas
• Capnometry: Measurement of CO
2 in gas mixture
• Capnography: Recording of CO
2
Conc versus time
Standard requirements of Capnometer:
• CO
2 reading shall be within ±12% of the actual value or ±4 mm Hg
• Must have a high CO
2 alarm for both inspired and exhaled CO
2
Technology:
• Infrared Analysis
• Chemical colorimetric analysis
Clinical Significance of Capnometry:
• Metabolism
• Respiration
• Circulation
• Equipment Function
• Confirming endotracheal and enteric tube placement
• Dec ET CO
2
:
Impaired peripheral circulation
Impaired lung circulation (Pulmn embolus)
Increased patient dead space
Hyperventilation
Hypothermia
Increased depth of anaesthesia
Use of muscle relaxants
Leak in sampling line
Leak around ET
• Increased ET CO
2
:
Absorption of CO2 from peritoneal cavity
Injection of NaHCO
3
Convulsions
Hyperthermia
Pain, anxiety, shivering
Increased muscle tone (reversal of muscle relaxation)
Hyperventilation
Upper airway obstruction
Rebreathing
Increased circulation from tissues to lung (release of tourniquet)
• Absent waveform:
Esophageal intubation
Disconnection
Apnea
Blockade of sampling line
Correlation between Arterial and End-tidal Carbon dioxide levels
• Normal: PaCO
2
– ET CO
2
= 2-5 torr
• Altered with:
Reduced FRC (Pregnancy, Obese pt)
Rebreathing
Neurosurgical procedures
During one lung ventilation
(In these cases transcutaneous CO
2 monitoring more accurate)
Capnography
• Examined for:
Height (Depends on ETCO
2
)
Frequency (R.R.)
Rhythm
Baseline (normally zero)
Shape (Top hat or Sine wave is normal)
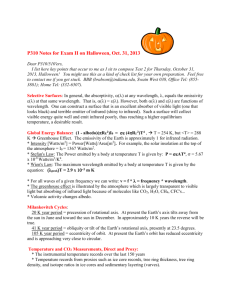
Capnography cont…
• Phase 1: E (Inspiratory baseline)
• Phase 2: B to C (Expiratory upstroke), S shaped- represents transition from dead space to alveolar space
• Phase 3: C to D (all from alveoli)
• End of Phase 3 (Point D): End tidal point (Max CO
2
)
• Alpha : Angle b/w Phase 2 & 3 (normal 100-110 degree)
• Beta: B/w end of phase 3 & Descending limb (90 degree)
• The slope of phase 3 (C to D) increases:
With PEEP
Airway obstruction
V/Q mismatch
And so angle Alpha also increases
And angle Beta decreases
• Angle Beta increases with:
Rebreathing
Prolonged response time
Unusual waveforms:
• Leak in sample line: Brief peak at the end of plateau
• Partially paralysed (making intermittent resp effort) :Curare cleft
• Cardiogenic occilations:
Seen in pediatric pts
(d/t heart beating against
Lungs)
Volatile Anaesthetic Agents:
• Standard Requirements:
Difference in value shall be within ) 0.2% vol%
High conc alarm is mandatory, low conc alarm is optional
• Measurement technique:
Infrared Analysis
Refractometry
Peizoelectric Analysis
• Significance:
Assess vaporizer function and contents
Information of patient uptake of the agent (insp & exp conc)
Information on Anaesthetic depth
Detecting contaminants/ disconnection
Nitrous Oxide:
• Measurement technique:
Infrared Analysis
• Significance:
Assess flowmeter function
Nitrogen:
• Previously measured using Raman spectroscopy or mass spectrometry
• Now no longer available
• Significance:
Verifying adequate denitrogenation before induction (imp for pediatric pt, in lung ds, dec FRC)
Detecting air emboli (Inc ET N2)