13CKotton case for TID2015
advertisement

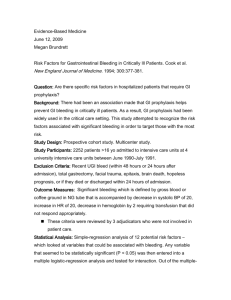
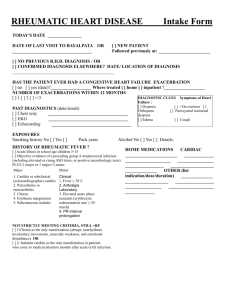
Pithy Case (…or a regular consult) Camille Nelson Kotton MD, FIDSA Clinical Director, Transplant & Immunocompromised Host Infectious Diseases Group, Infectious Diseases Division, Massachusetts General Hospital Associate Professor, Harvard Medical School Chair, Infectious Disease Community of Practice, American Society of Transplantation Immediate Past President, Infectious Disease Section, The Transplantation Society Clinical Vignette 36yo male, Type I diabetes, 3 months after kidney/pancreas transplant (on prednisone 5 mg/day, mycophenolate mofetil (Cellcept) 1000mg twice a day, tacrolimus 4 mg twice a day) Transferred with three days of worsening L sided abdominal and flank pain Chest CT findings concerning for necrotizing pneumonia/cavitating lesion. On valganciclovir and TMP/SMX prophylaxis Exam: ill appearing, febrile, dull breath sounds at left base, crackles both lungs, surgical incisions are fine Two days later What is the diagnosis? A. Aspergillus B. Mucormycosis C. Necrotizing Gram negative D. Mycobacterial (M. kansasii, etc) E. Nocardia Diagnostics Fungal markers all negative (blood) 1,3 beta D glucan Galactomannan Ag Cryptococcal Ag Thoracentisis exudate, chest tube placed Bronchoscopy, biopsy Culture Data Specimen Type: LEFT EFFUSION/PLEURAL FLUID (and BAL) Gram Stain – SPUN SLIDE: abundant polys, moderate red blood cells, few mononuclear cells, no organisms seen Fluid Culture - MIC DILUTION METHOD Amikacin Amoxicillin/Clavulanate Susceptible ** Ceftriaxone Intermediate Ciprofloxacin Resistant Clarithromycin Susceptible Doxycycline Resistant Imipenem Susceptible Linezolid NOCARDIA NOVA COMPLEX, subspecies veterana Susceptible Susceptible Minocycline Intermediate Moxifloxacin Resistant Tobramycin Resistant Trimethoprim/Sulfa Susceptible Treatment Brain CT negative for metastatic infection Imipenem + azithromycin until radiographic improvement** Markedly improved in first few days (?chest tube placement) Doing well at 6 months, double treatment stopped Will need long term secondary prophylaxis with TMP/SMX “There are increasing reports of breakthrough infections by TMP-SMX-susceptible Nocardia isolates in patients taking TMP-SMX prophylaxis, creating some doubt about the utility of this agent for prevention of nocardiosis (14). Minero and colleagues found that 21.6% in their series were on TMP-SMX prophylaxis at the diagnosis of nocardiosis, of which 62.5% were still susceptible to the drug (14). Similarly, in their series of 19 Nocardia cases, Santos and colleagues noted that most had received TMP-SMX prophylaxis for Pneumocystis jiroveci (25). In many of these reports, dosing of TMP-SMX prophylaxis is not provided. Because the dosing of TMP-SMX employed at some centers for prophylaxis of Pneumocystis jiroveci in organ transplant recipients is two to three times per week, insufficient blood levels due to intermittent dosing could explain breakthrough infections, although nocardiosis has also been reported despite daily TMP-SMX prophylaxis (54).” Clinical Vignette www.idimages.org