System Responses to Exercise and Disease

System Responses to
Exercise and Disease
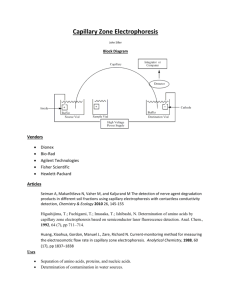
Hemodynamic changes in response to hemorrhage
A drop in systemic arterial pressure initiates the baroreceptor reflex and greatly increases sympathetic outflow.
This accounts for the increases in heart rate and TPR. Remember that the regulated variable here is mean arterial pressure. In this example, the blood loss is mild (no more than about
1 liter for a 60-70 Kg person) and the reflexive compensation is able to protect MAP while slower responses can restore the lost fluid, electrolytes and blood cells. Note that cardiac output is not a regulated variable and cannot return to normal until volume restoration occurs.
Irreversible Hemorrhagic Shock
If the immediate responses were inadequate, a rapid positive-feedback cycle would cause hemorrhagic shock.
Cardiac depression : heart fails to pump enough blood to meet the needs of itself and the CNS, leading to
Vasomotor Failure : depressed blood flow to brain is the most potent of sympathetic stimulants, but after a few minutes of depressed blood flow, sympathetic outflow drops and those arterioles that had been constricted by their adrenergic inputs then dilate, causing a collapse of
MAP.
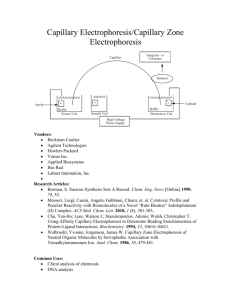
Hemodynamic changes during exercise
Organ Resting
Perfusion
(L/min)
Perfusion during Exercise
(L/min)
Dominant effect
Brain 1
Heart 0.5
Skeletal Muscle 1
1
1
12 autoregulation autoregulation autoregulation + beta adrenergic effect
Skin 0.5
4 thermoregulation
Splanchnic
Kidney
TOTAL CO
2
2
7
1
1
20
Alpha adrenergic effect
Alpha adrenergic effect
How is a 3X increase in CO possible during exercise?
• Can it be the result of cardiac effects only? Use the model to find out.
CO
RAP
Exercise responses are multifactorial
The magnitudes of MAP, CO and
TPR changes in exercise are affected by multiple factors, including
Conditioning
Muscle mass
Exercise intensity level
Environmental temperature
In some highly muscular individuals, MAP may decrease significantly in intense exercise, due to a profound decrease in diastolic pressure.
Capillary Filtration, Interstitial
Fluid and the Lymphatic System
Capillaries and Capillary Filtration
• Capillaries are the major sites of exchange of materials between tissues and bloodstream
• Materials may move across capillary walls only by diffusion and bulk flow, with exceptions:
– brain capillaries actively transport glucose into the brain ISF
– Ordinarily, capillary slits are not permeable to molecules as large as plasma proteins, but in order for protein hormones to enter the bloodstream and to reach their targets, and for antibodies to reach sites of infection, selected proteins can move across capillary endothelial cells by transcytosis.
There are 3 basic capillary types
The most common type – clefts are 10-
15 nm wide, but smaller in brain capillaries, which form the blood-brain barrier
A fenestra is a window.
Endothelial cells are perforated like a shower head – to increase bulk flow
- found in epithelia like intestine and exocrine glands.
Large gaps are present – this allows the capillary to pass proteins – this form is found in liver, where plasma proteins are synthesized.
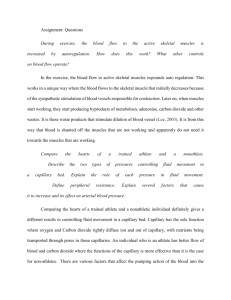
Capillary filtration
3
28
Osmotic pressure gradient is due to plasma proteins and doesn’t change along capillary length – little protein is filtered.
3
28
Arteriolar end
Venular end
Total pressure
= 10 outward
35
~0
15
Capillary hydrostatic pressure decreases along capillary length due to friction
~0
Total pressure =
10 inward
Edema is an excess of ISF that reflects an imbalance between rates of formation and drainage of ISF
Hydrostatic factors that promote systemic edema:
– Hypertension
– Vasodilation
– Increased venous pressure
– Erect posture or compression of central veins
– Lymphatic blockage
– Right Heart failure
Osmotic factors that promote systemic edema:
Loss of serum proteins (protein undernutrition) inflammation with increased capillary leakiness and release of tissue proteins
Edema and congestive heart failure
“Congestive” refers to the fact that the disease-weakened heart must operate in a larger range of EDV and ESV to be able to generate enough force to sustain MAP.
The edema results from increased venous pressure that backs up to increase capillary hydrostatic pressure, favoring filtration over absorption.
Patients with generalized congestive heart failure typically experience peripheral edema during the day and pulmonary edema at night.
The Lymphatic System
• Lymphatic capillaries are blind-ended tubes with flap valves that permit entry of
ISF
• Lymphatic veins have 1way valves like blood veins, so periodic compression of lymphatics improves lymph flow.
• Ultimately, lymph drains back into the blood vascular system through two ducts – the thoracic duct (to left subclavian vein) and right lymphatic duct (right subclavian vein).
Lymph drainage
• opposes edema
• recovers proteins that escape across capillary walls
• delivers information about presence of infectious agents and non-self antigens to lymph nodes for immune surveillance
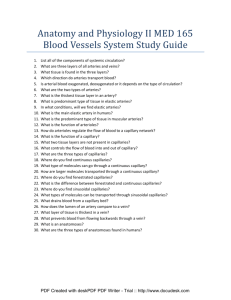
Overview of blood and lymph transport
Note that:
Cardiac output is a really large number
The fluid cycle between blood and
ISF is a large number
Diffusional exchanges of water and glucose between tissues and blood are truly huge numbers, compared to filtrative flows
Major Issues to know/understand about
Cardiovascular Physiology
• Heart cycle – sequence of events and cause-effect relationships
• EKG: correlate waves with heart processes, determine axis, and recognize simple abnormalities.
• Baroreceptor reflex and control of heart and vasculature by ANS
• System properties: what they are, how they can change, and how they interact to determine the system variables.
– Know which tissues are dominated by extrinsic control and which by autoregulation
– As demonstrated in class, be able to use the model to predict outcomes for system variables in exercise, blood loss, disease, and application of drugs that affect specific system properties
• Capillary filtration and lymphatic function – forces involved in ISF formation, and how they can change in disease states.
• Know approximate normal values of the following variables for humans:
– Resting CO/min and daily CO
– MAP for systemic and pulmonary loops
– RAP
– Daily values of capillary filtration and lymph flow