Poster
advertisement

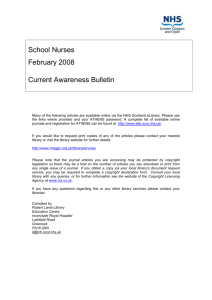
Modernisation of Roles SA 211 NURS 6035 Seminar Presentations The Role of the Patient SICK ROLE RESPONSIBILITY CHOICE EXPERT PATIENT • Following the formation of the NHS in the late 1940s, Parsons (1975) presented the idea of the ‘sick role’ in which the patient is seen as a social deviant and there is a hierarchical inequality between the patient and therapeutic agencies. • The sick role was thought to be socially constructed by: • Assertion and acceptance by self and others of being a victim of illness. • Exemption of ordinary daily obligations e.g. by staying in bed. • Seeking help from an institutionalised health service agency which entails an admission that being sick is undesirable/deviant and requires proper management. • Parson’s theory suggested that patients only choice was to accept the fact that they were ill and seek professional help to get better. Patients could no longer self refer to hospital as they had done in the past, instead they had to be referred by a GP. • The nurse-patient relationship was not an equal one at this time. Instead, the nurse was the figure of authority, and the patient was expected to obediently entrust his care to her. • Through the 1950s and 1960s the involvement of patients in their care became more common. • The Chief Nursing Officer (1948-1958), Dame Elizabeth Cockayne, commented on the change of role (Rivett): ‘The patient’s point of view is given more attention today, indeed the patient is part of the team. We find ourselves doing things with patients, and not just for them as previously, leading them to self-direction and graduated degrees of independence.’ • Nursing care became a partnership with the patient with increasing treatment options available and a collaborative approach to managing conditions. • More emphasis was also put on patients taking responsibility for their own health with increasing education and information available for patients towards the end of the twentieth century. • Increasingly policy has been focused on a health service which will enable people to take responsibility for their own health while still providing a free at point of use service as needed. • The NHS Plan (2000) placed a renewed importance on the patient’s role in their own care, with a shift towards patient choice, listening to patient views and clinical choices made in consultation with the patient. • Patient choice has continued to hold a prominent position in policy to the present continuing through the change of governments. • Patient choice can be seen from two very different angles: • A patient’s lifestyle choices – with an increasing emphasis on health promotion and encouraging people to choose healthy behaviours. • Treatment choices – a patient’s ability to consider different treatment options, location, provider or to refuse treatment. • The two White Papers issued in 2010 each have one of these angles central to their proposals. Equity and Excellence (2010a) particularly has a focus on increasing treatment choices for individuals although in reality this could create inequalities. • Knowledge and experience of their condition held by the patient has in the past been an untapped resource. Utilising it could greatly benefit the quality of patients’ care and ultimately their quality of life. • The idea of developing a major initiative on Expert Patients was set out in the Government’s 1999 White Paper, Saving Lives: Our Healthier Nation. A further commitment to implementing a formal programme was made in The NHS Plan (2000). • A patient’s knowledge of his or her condition would ideally be developed to a level whereby self-management, within the boundaries of a medical regime, becomes a real option. • It has been reported that patients want more care available outside hospitals and to be able to take responsibility for their own health, demand for community nurses is likely to rise. • Modern technology is increasingly being utilised in the development of telecare which allows those with long term conditions to be monitored remotely by trained staff. Patients would need to be educated and empowered to use this type of system (Giordano et al 2010). DH 1999 Saving Lives: Our Healthier Nation 1942 The Beveridge Report DH 1997 The New NHS 1946 The NHS Act DH 2000 The NHS Plan DH 2001a The Expert Patient DH 2001c Valuing People DH 2001b Tackling Health Inequalities DH 2004a Agenda for Change DH 2004b Choosing Health DH 2005a Independence, Wellbeing & Choice DH 2005b Self-care: A Real Choice DH 2006a Our Health, Our Care, Our Say DH 2006b Modernising Nursing Careers: Setting the Direction DH 2010a Equity & Excellence DH 2010b Healthy Lives, Healthy People The Role of the Nurse TENDING THE ‘SICK’ • The NHS Act (1946) failed to provide for the training of nurses. This meant that the number of trained nurses and their skill level did not match the ambitions laid out in the Beveridge Report (1942). • Entry requirements and training standards for nursing had relaxed during the second world war and in many places the number of students greatly exceeded trained staff. For 600 beds, Aberdeen Royal Infirmary had 93 trained staff and 330 students (Rivett). • There was therefore a reliance on students as part of the workforce which inevitably impacted on the trained nursing role and the nurse-patient relationship. • In 1952 more stringent standards were reintroduced by the General Nursing Council and the foundations for building nursing as a profession were laid (Tweddell 2008). MANAGERS SPECIALISTS EDUCATORS / ADVOCATES • Through the 1950s and 1960s the role of the nurse went through a transitional period from lack of training and hands on care to improved education and training and a wider responsibility to both give hands on care and a take a lead in its provision. • The role of matron disappeared in the late 1960s but was reintroduced in 2001 following ‘The NHS Plan’. Modern matrons were a key part of modernising the NHS with the aim to improve patient experience. • In 2004 knowledge and skills frameworks (KSFs) were introduced as part of Agenda for Change (2004a). These outline key competencies for any role in the NHS to identify skills needed and guide individual’s development. • With the transition of students to supernumerary status and the resulting increase in health care support workers. Nurses also nearly always act as managers within their team. • Many nurses now operate in specialist fields and advanced practice ensuring that experienced and highly skilled nurses stay close to patient care (DH 2006b). • Over 50,000 nurses in the UK can now prescribe for their patients (DH 2006b). • NMC definitions of advanced practitioners with role expansion involving physical examination, making a final diagnosis, carrying out treatment and prescribing are difficult to distinguish from that of doctors roles (Wiseman 2007). • It is thought that in future nurses roles will continue to extend and become more specialist (Longley, Shaw and Dolan 2007). • Essential nursing care could then be increasingly completed by health care support workers and the growing numbers of assistant practitioners, who are currently unregistered. Responsibility for care given needs to be clearly defined. • Historically, the role of patient advocacy for nurses has been a moral obligation. Advocacy is usually employed by someone powerful on behalf of someone who has no power (Teasdale 1998). • The idea of advocacy holds true for nursing with additional aspects including of educating patients to understand their condition to empower them to self advocacy. • Practicability of nurse advocacy can be limited in practice as it’s difficult to teach and nurses may not be the most impartial people to provide advocacy, importance of keeping the patient’s best interest at the centre of care. • Supporting staff with training to educate patients is highlighted in the white paper Choosing Health (DH 2004b). This is crucial to allow patients to make informed choices. • Patient education and self-management is one of the main areas thought to help reduce rehospitalisation (IHI 2009). OTHER REFERENCES Giordano, R., Clark, M. Goodwin. (2010). Perspectives on telehealth and telecare: Learning from the 12 Whole System Demonstrator Action Network (WSDAN) sites Briefing Paper. The King’s Fund Institute for Healthcare Improvement (IHI) (2009) Effective Interventions to Reduce Rehospitalisations: A Survey of the Published Evidence, Available at: http://www.ihi.org/offerings/Initiatives/STAAR/Documents/STAAR_A_Survey_of_the_Published_Evidence.pdf Longley, Shaw and Dolan (2007) Nursing: Towards 2015 Alternative scenarios for healthcare, nursing and nurse education in the UK in 2015 (Commissioned by the NMC) Parsons, T. (1975) ‘The sick role and the role of the physician reconsidered’, Milbank Memorial Fund Quarterly, 53(3), pp 257-278 RESEARCH POSTER PRESENTATION DESIGN © 2011 www.PosterPresentations.com Rivett, G. National Health Service history: 1948 – 1957 – Establishing the National Health Service, http://nhshistory.net/Chapter%201.htm#Nursing (Accessed 22 February 2012) Teasdale (1998) Advocacy in Health Care. Oxford: Blackwell Science Tweddell, L. (2008) The birth of the NHS – July 5th 1948: The facts, figures and quotes that shaped the history of the national health service, Available at: http://www.nursingtimes.net/the-birth-of-the-nhs-july-5th-1948/441954.article (Accessed: 22 February 2012) Wiseman H. (2007) Advanced nursing practice – the influences and accountabilities. British Journal of Nursing, 16(3), 167-173