Horner Syndrome
advertisement

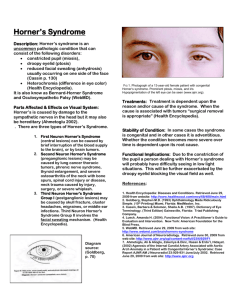
Grand Rounds Conference Lara Rosenwasser Newman, MD University of Louisville Department of Ophthalmology and Visual Sciences October 2, 2015 Patient 1 - Subjective CC: unequal pupils (anisocoria) HPI: 4 month old male in whom pediatrician and parents noted unequal pupils History POH: None PMH: born via spontaneous vaginal delivery at home, complicated by no prenatal care (mother did not know she was pregnant), nuchal cord x2 Eye Meds: None Meds: none Allergies: NKDA Objective BCVA: Pupils: IOP: EOM: OD CSM 6->4 soft full OU OS CSM 5->3 soft Objective SLE: OD OS External/Lids WNL mild ptosis, 1-2 mm Conjunctiva/Sclera clear/white clear/white Cornea clear clear Anterior Chamber formed formed Iris increased brown pigment less brown pigment Lens clear clear DFE ON pink/sharp, M/V/P WNL OU Clinical Photo Impression & Plan Horner syndrome OS Decreased iris pigmentation OS Ptosis OS, 1-2 mm Miosis OS vs OD Likely congenital Still could be acquired in a 4 month old Ordered MRI head/neck/chest Patient 2 CC: “unequal pupil size and clogged tear ducts” HPI: 6 month old girl with OD pupil larger than OS, drainage OU, OD draining more and yellow Exam: vision CSM OU Pupils 6.5 OD and 4.5 OS in dark, 2.5 OU in light Dilation lag OS MRI head/neck/chest ordered DDx of Anisocoria in Children Physiologic anisocoria: Usually <1 mm, can vary day to day, inequality does not change with bright/dim light Tonic pupil: greater in bright light, sluggish, segmentally responsive to light, more responsive at near Horner syndrome: greater in dim light, associated ptosis miosis Horner• Pupillary Syndrome • Facial anhidrosis AKA oculosympathetic palsy Clinical picture: Ptosis, miosis, and anhidrosis Congenital cases associated with iris heterochromia Due to disturbance somewhere along sympathetic pathway to dilator pupillae muscle and ciliary body Central or 1st order: • Hypothalamus • Brainstem • Cervical spinal cord Terminates at ciliospinal center of Budge between C8-T2 Pre-ganglionic or 2nd order: • Spinal cord, cervical/thoracic • Brachial plexus • Pleural apex Post-ganglionic or 3rd order: • Superior cervical ganglion • Cavernous sinus • Internal carotid artery • Joins ophthalmic division of trigeminal nerve Diagnosis and Localization Diagnose with topical cocaine or apraclonidine Cocaine dilates unaffected eye, no effect on affected eye Apraclonidine has little effect on normal pupils, but dilates sympathetically denervated/hypersensitive eyes Localize with topical hydroxyamphetamine Enhances release of NE from intact 3rd order neuron Pupil does not dilate: suspect 3rd order lesion Pupil dilates: 1st or 2nd order First Order Causes of Horner’s Lateralpresents Medullary Most commonly as partSyndrome of lateral (Wallenberg Syndrome) medullary syndrome or Wallenberg syndrome Infarction in lateral medulla in brainstem leads to Infarction ataxia,• vertigo, Horner’s • Ataxia Other central causes: • Vertigo Trauma • Horner’s Demyelination Syndrome Cord neoplasm Syringomyelia Second Order Causes Preganglionic Trauma: Birth Iatrogenic Chest tube Surgery birth, iatrogenic (chest tube, surgery) Tumors: Trauma Tumor Mediastinal Lung Vertebral / Rib mediastinal, lung, vertebral, rib Other: infectious, vascular, thyroid mass, thoracic aortic aneurysm, brachial plexus trauma PNET Third Order Sites/Causes Carotid space – carotid artery, internal jugular vein, lymph nodes Neoplasm at skull base, cavernous sinus, nasopharynx Infections including: Otitis media Lemierre syndrome: acute pharyngitis due to Fusobacterium necrophorum, leading to septic thrombophlebitis of internal jugular Foreign body rd 3 order Horner’s with pain Cluster headaches Raeder paratrigeminal syndrome Carotid artery dissection Pain in temple, orbit, sometimes throat Get MRA Pediatric Carotid Space Masses Neuroblastoma Neurofibroma Schwannoma Myofibrous tumors Paraganglioma (rare) What to image Hypothalamus Brainstem Brachial plexus Lung apex Carotid space Skull base Cavernous sinus Orbital apex Order: MRI head, neck, and chest with and without contrast Hedlund, Gary. Imaging the Pediatric Patient with Horner’s Syndrome. Medicine.utah.edu/radiology conferences/Friday/62-HedlundHornerSynd.pdf Patient 2 MRI results MRI brain: Nonspecific bilateral otomastoid disease, congestive vs inflammatory, otherwise WNL MRI Neck: “small paraspinal mass at L lung apex adjacent to T1 and T2 vertebral bodies… abuts vertebral bodies without evidence of osseous invasion or neural foramina involvement… measures approx 1.2 cm (TR) x 1.6 cm (AP) x 2.2 cm (SI)… most suggestive of the ganglioneuroma/neuroblastoma spectrum given the history of Horner's syndrome. Small lymph nodes are visualized in the jugular chain bilaterally consistent with benign reactive disease. MRI Chest: “Enhancing solid lesion left posterior mediastinum/paraspinal location at C7-T2. Measuring approximately 2.2 cm craniocaudally x 1.2 cm medial laterally x 1.6 cm anteroposterior. Likely represents a neuroblastoma/similar etiology. Within study limits, no definite spinal extension. However study was not dedicated to evaluate the spine.” MRI Chest Patient 2 - Course Underwent resection of L apical lung tumor via videoassisted thoracoscopy 19 days after presentation to ophthalmologist Op note: purplish mass at lung apex, appearing to arise from 2 most cephalad superior ganglia Posteriorly connected to sympathetic chain Had to divide sympathetic chain, remove ganglia A few small nodes removed with the specimen Patient 2 - Pathology Neuroblastoma – favorable histology Poorly differentiated Margins involved – “minimal periganglion soft tissue margin positive” Extent: extracapillary extension without adjacent organ involvement 6/6 adherent lymph nodes positive for tumor MYCN gene negative Patient 2 - Immunophenotyping Discrete population of large cells negative for CD3, CD19, CD45, brightly positive for CD56 Consistent with non-hematopoietic malignancy Bright CD56 positivity: suggestive of neuroendocrine origin Retrospective chart review of 56 children seen for Horner Syndrome 1993-2005 @ UPenn Of 18 who had both urine studies and imaging, 33% (6) had responsible mass lesions found 24 had urine catecholamine metabolite studies (all negative results) 20 had complete modern imaging (brain/neck/chest) Neuroblastoma (4), Ewing sarcoma (1), juvenile xanthogranuloma (1) Conclusion: recommend MRI brain, neck, chest with and without contrast and urine studies (imaging more sensitive) Two cases of 6-month olds Patient 23: parents thought lid abnormality present since 2 wks old, maybe since birth MRI w/right apical lung mass Stage 2A neuroblastoma resected Patient 24: anisocoria and ptosis, vacuum extraction at birth, lid “swelling” noted by parents at 4.5 months MRI with cervical lymph node Repeat MRI 3 months later node larger Stage 3 intermediate risk neuroblastoma resected Mahoney NR, Liu GT, Menacker SJ, Wilson MC, Hogarty MD, Maris JM. Pediatric horner syndrome: etiologies and roles of imaging and urine studies to detect neuroblastoma and other responsible mass lesions References 1. BCSC: Pediatric Ophthalmology and Strabismus (Section 6) 2. BCSC: Neuro-ophthalmology (section 5) 3. Mahoney NR, Liu GT, Menacker SJ, Wilson MC, Hogarty MD, Maris JM. Pediatric horner syndrome: etiologies and roles of imaging and urine studies to detect neuroblastoma and other responsible mass lesions. Am J Ophthalmol. 2006 Oct;142(4):651-9. PubMed PMID: 17011859. 4. Hedlund, Gary. Imaging the Pediatric Patient with Horner’s Syndrome. Medicine.utah.edu/radiology conferences/Friday/62HedlundHornerSynd.pdf 5. Kanski and Bowling’s Clinical Ophthalmology, 7th edition THANK YOU DDx of Pediatric Heterochromia Hypochromic heterochromia: Horner syndrome Incontinentia pigmenti (Bloch-Sulzberger syndrome) Fuchs heterochromia Waardenburg syndrome Non-pigmented tumors Hypomelanosis of Ito Hyperchromic heterochromia: Oculodermal melanocytosis Pigmented tumors Siderosis Iris ectropion syndrome Extensive rubeosis Port-wine stain Diagnosis of Horner Syndrome Topical cocaine (4% or 10%): Blocks re-uptake of norepinephrine released at sympathetic terminals in the eye dilation, lid retraction, conj blanching in unaffected eye Affected eye: no norepinephrine secreted so no effect on pupil Topical apraclonidine (0.5% or 1%), weak alpha-1 agonist: Little effect on pupil size in most normal eyes Iris dilator is supersensitive to adrenergics in sympathetically denervated eyes pupil in affected eye will dilate Localization of lesion in Horner’s Topical 1% hydroxyamphetamine: Enhances release of presynaptic norepinephrine from an intact 3rd order neuron If pupil does not dilate: suspect 3rd order lesion If both pupils dilate well, 1st or 2nd order lesion