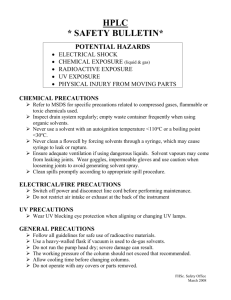
Pre-Event Planning Evaluating your facility Plan of Action Emergency management plan Mitigation Preparedness Response Recovery Identifying a Problem Most common features of an outbreak caused by a bioterrorism agent Influenza-like illness Viral exanthem: rash/fever Gastrointestinal complaints Surveillance Methods Databases Mainframe systems Admissions Emergency department Microbiology Surveillance Methods Mainframe systems Laboratory Pathology Radiology Pharmacy Surveillance Methods Access to system Report distribution Computer access Patient electronic medical record HIPAA concerns ? Confirming the Diagnosis Coordination of surveillance plan Review of symptoms Gathering data Communication with internal and external resources Facilities/Environmental Isolation Rooms Negative Pressure Alternatives Transportation Routes Lockdown Disinfectants PPE Laboratory Support Level of involvement Level Level Level Level A: Initial work- r/o BT agents B: County/state- agent confirmation C: Large state lab/ advanced labs D: CDC/DOD labs Laboratory Support BSL levels 1: 2: 3: 4: General office Biosafety cabinets Negative airflow “Moon suits” Specimen Collection Collection Preparation Media Preservation Shipping Notification Febrile, Vesicular Rash Illness Algorithm for Evaluating Patients for Smallpox Patient with Acute, Generalized Vesicular or Pustular Rash Illness Institute Airborne & Contact Precautions Alert Infection Control on Admission Low Risk for Smallpox Moderate Risk of Smallpox High Risk for Smallpox (see criteria below) (see criteria below) (see criteria below) ID and/or Derm Consultation VZV +/- Other Lab Testing as indicated ID and/or Derm Consultation Alert Infx Control & Local and State Health Depts History and Exam Highly Suggestive of Varicella Diagnosis Uncertain Varicella Testing Optional Test for VZV and Other Conditions as Indicated Non-Smallpox Diagnosis Confirmed Report Results to Infx Control No Diagnosis Made Ensure Adequacy of Specimen ID or Derm Consultant Re-Evaluates Patient Smallpox Response Team Collects Specimens and Advises on Management Cannot R/O Smallpox Contact Local/State Health Dept Testing at CDC NOT Smallpox Further Testing SMALLPOX Smallpox Diagnosis Traditional confirmatory methods Electron microscopy of vesicle fluid Rapidly confirms if orthopoxvirus Culture on chick membrane or cell culture Slow, specific for variola Newer rapid tests Available only at reference labs (e.g. CDC) PCR, RFLP Lab Methods for Confirmation of Orthopoxvirus Diagnosis PCR related methods for DNA identification, (e.g., realtime PCR) Electron microscopy Histopathology Culture Serology Antigen detection (IFA, EIA ag capture) IgM capture Neutralization antibodies IgG ELISA Negative Stain Electron Microscopy Vaccinia Specimen Collection Vaccinia and variola specimen collection essentially the same Check CDC website for: Recent updates in orthopox specimen collection specifics Appropriate infection control practices Shipping criteria Laboratories www.bt.cdc.gov/agent/smallpox/ responseplan/files/guide-d.pdf Specimens for Vaccinia-Related Disease: Vesicular Rash Lesion ‘roofs’ and crusts Vesicular fluids: Touch prep EM grid Biopsy Serum Others (e.g., CSF) Specimen procurement/handling By recently successfully immunized person Appropriate PPE (gowns, gloves, mask, protective eyewear) Open vesicle with blunt end of blade Collect with cotton swab Place swab into sealed vacuum blood tube Place tube in larger jar, tape lid Vaccinia lesion on foot Lifting a crust or ‘roof’ from the skin Applying microscope slide to lesion Handling VHF Specimens Sample for serology - 10-12 ml ship on dry ice Tissue for immunohistochemistry formalin-fixed or paraffin block ship at room temperature Tissue for PCR/virus isolation ante-mortem, post-mortem; ship on dry ice Ship serum cold or on dry ice in a plastic tube Centers for Disease Control and Prevention Yersinia pestis: Specimen Selection Specimen selection is important Bubonic - bubo - lymph node aspirate Septicemic - blood - Obtain three sets 10-30 minutes apart Pneumonic Sputum/throat Bronchial washings Centers for Disease Control and Prevention Yersinia pestis: Specimen inoculation Inoculate routine plating media and make thin smear for DFA Use Wayson only if DFA is unavailable Centers for Disease Control and Prevention Laboratory Confirmation By State Health Dept., CDC and Military labsAntigen detection PCR IgM enzyme immunoassay Immuno-staining Level A Lab Procedures Yersinia pestis Gram stain Wayson stain Growth characteristics on agar Growth characteristics in broth Centers for Disease Control and Prevention Yersinia pestis Gram stain Small, gram-negative bipolar-stained coccobacilli Must confirm by DFA and mouse inoculation Centers for Disease Control and Prevention Gram Negative Coccobacilli Most likely Acinetobacter Actinobacillus H. aphrophilus Bordetella spp. Pasturella spp. Least likely DF-3 Brucella spp. Francisella spp. Level A Lab Procedures Francisella tularensis This is a dangerous, highly virulent organism and it should not be manipulated at the bench, but under a controlled environment Gram stain Growth characteristics in broth Growth characteristics in agar Centers for Disease Control and Prevention Transportation Communications Security Transportation is More than… Communications is More than… Security is More than… Transportation Transportation Mission Organize and coordinate the transportation of all casualties, ambulatory and non-ambulatory Arrange for the transportation of human and material resources to and from the facility Anticipate Transportation Needs: Transfer agreements with lower levels of care: Which patients? What facilities? How…what means of transportation? Anticipate Transportation Needs: Transporting discharged patients (or getting family members to pick them up) Limited or no access to facility Difficulty contacting families Secure private ambulance/cabs for discharged patients Anticipate Transportation Needs Plan for transportation of staff and supplies to and from your organization: Off sight gathering locations: Private vehicle vs. group (bus/van) transportation Non essential employees? Housekeeping Anticipate Transportation Needs Provisions Agreements in place to have vendors send supplies without actual request Need for identification system of suppliers to pass through police or security checkpoints Transportation Utilize personnel from labor pool as patient transporters Assemble stretchers and wheelchairs in proximity to ambulance off loading and triage area Identify transportation needs of `walking’ decontaminated or noninjured individuals Communications Communications Mission Organize and coordinate internal and external communications Act as custodian of all logged/documented communications Anticipate Communication Needs: Provisions for normal system overloaded or inoperable: Telephone Page Cellular Fax Alternative arrangements: Telephone trees Pay phones Walkie-talkies Anticipate Communication Needs: Organized runner or messenger system: Area layout maps Established communications with local emergency medical services or management agencies Plans to keep staff informed Internal Communication Systems and equipment Train staff to repair equipment Availability of replacement parts Telephone lines buried, marked and protected Internal Communication Keep written records Radio transmitter/receivers equipped to operate on multiple frequencies Potentially use closed circuit TV or broadcast one-way messages Internal Communications: Patient Records Updating and keeping track of patient records essential Triage tags Medical records Registration History Treatment Communications: Staff Information Frequent communications of accurate information What has happened How many patients to expect and when How organization will help meet needs Recognize healthcare workers’ needs to contact families Call trees Designated phone number External Communications: Establish communication lines with community and national disaster agencies Employees, medical staff and volunteers Family members, friends and visitors Community office of emergency management External Communications: Law enforcement or military EMS dispatch/services Public utilities Radio operations Public safety communication services Health Department Security Security Mission Ensure any activity is done with maximum security Provide personal security to staff, patients, visitors and property Anticipate Security Needs: Nuclear, biological, chemical and explosive Internal vs. external Internal Damage to structure Evacuation while minimizing passage through contaminated areas Damage to support systems: water or electric External Prevailing winds Evaluate need to turn off air conditioning, seal windows Security Personnel trained: Early recognition Procedure to lock down or minimize access and egress Direct exposed foot traffic to decontamination Direct families/friends to centralized area Direct media to designated spokesperson Security Entry route for staff, supplies etc Personnel identification policy Establish ambulance entry and exit routes Secure triage, ER, morgue and other sensitive areas Security Maintain effective crowd control Maintain chain of evidence for any criminal or other investigation Provide vehicular and pedestrian traffic control Parking and decontamination issues Security Secure food, water, medical and blood reserves Credentialing/screening process of volunteers Initiate contact with fire, police agencies through communication liaison when necessary Anticipate, Plan and Practice Isolation Guidelines ANTHRAX Use Standard Precautions Patient Placement Private rooms not necessary Skin lesions may be infectious by direct contact Patient Transport Use Standard Precautions Cleaning, disinfection, sterilization Use facility procedures for surfaces, equipment Bleach Standard Precautions for post-mortem care BOTULISM Use Standard Precautions Patient Placement No person-to-person transmission Patient Transport Use Standard Precautions Cleaning, disinfection, sterilization Use facility procedures for surfaces, equipment Standard Precautions for post-mortem care PLAGUE For pneumonic plague, Droplet Precautions until 72 hours of antimicrobial therapy completed Patient Placement Place infected patients in private room Cohort symptomatic patients with similar symptoms when private rooms not available Maintain at least three feet between infected patients and others when cohorting is not possible Avoid placing patients requiring Droplet Precautions with immunocompromised patients PLAGUE Patient Transport Transport for essential purposes only Patient should wear surgical mask Cleaning, disinfecting, sterilization Use facility procedures for surfaces, equipment Standard plus Droplet Precautions for post-mortem care SMALLPOX Airborne and Contact Precautions Patient Placement Monitored negative pressure room Doors must remain closed Facilities without negative pressure rooms should have plans for transfer of patients Cohorting maybe be used in outbreaks SMALLPOX Patient Transport Transport for emergencies only Patient must wear surgical mask and be completely covered Cleaning, disinfection, sterilization Ensure management of contaminated surfaces and equipment Airborne and Contact Precautions for post-mortem care Glass vials or tubes should not be used for laboratory specimens TULAREMIA Use Standard Precautions Patient placement No person-to-person transmission Patient transport Use Standard Precautions Cleaning, disinfection, sterilization Use facility procedures for surfaces, equipment Standard Precautions for postmortem care VIRAL HEMORRHAGIC FEVERS (VHF) Use Airborne Precautions If negative pressure room not available, use HEPA filtration unit Face shields in addition to N95 respirators Patient Placement Monitored Negative pressure room Cohort patients with similar symptoms Patient transport Transport for essential purposes only In elevator, all personnel should wear PPE Patient must wear surgical mask and be completely covered VHF Cleaning, disinfection, sterilization Meticulous cleaning daily of all surfaces and equipment in patient’s room Disinfectant discarded before exiting patient’s room Reusable cloths and mop heads should not be reused and sent for disinfection/laundering All reusable equipment to be cleaned and disinfected before taking from room Curtains and linens should be changed when soiled or on discharge VHF Cleaning, disinfection, sterilization continued Cleaning bucket and mop handle to remain in patient’s room. Contact and Airborne Precautions for post-mortem care BRUCELLOSIS Use Standard Precautions Patient placement Not transmitted person-to-person Patient transport Use Standard Precautions Cleaning, disinfection, sterilization Use facility procedures for surfaces, equipment Standard Precautions for post-mortem care Q FEVER Use Standard Precautions Patient placement No person-to-person transmission Patient transport Use Standard Precautions Cleaning, disinfection, sterilization Use facility procedures for surfaces, equipment Standard Precautions for postmortem care Precautions Patient Placement Patient Transport Cleaning, sterilization Postmortem Anthrax Standard No special Standard Precautions Facility policy Standard Botulism Standard No special Standard Precautions Facility policy Standard Brucellosis Standard No special Standard Precautions Facility policy Standard Essential purposes Patient wears mask Facility policy Standard + Droplet Meticulous Special treatment of mop head and water Airborne + Contact Disease Plague Droplet for pneumonic Private room or cohort, leave three feet if no private rooms Smallpox Airborne + Contact Negative pressure Doors closed Transfer plans May cohort Essential purposes Patient wears mask Patient covered Q Fever Standard No special Standard Precautions Facility policy Standard Tularemia Standard No special Standard Precautions Facility policy Standard
 0
0
advertisement


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users