full report - Daniel B. Johnson
advertisement

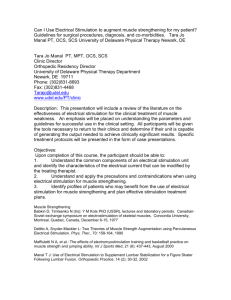
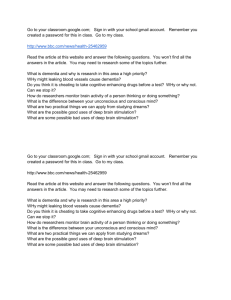
DANIEL JOHNSON GRADUATE STUDENT, ELECTRICAL ENGINEERING CALIFORNIA STATE UNIVERSITY , FULLERTON IEEE OC Student Design Contest NeuroMuscular Electronic Stimulator Functional Electrical Stimulation (FES) a technique that uses electrical currents to activate nerves innervating extremities affected by paralysis resulting from spinal cord injury, head injury, stroke or other neurological and physical disorders, restoring function in people with disabilities. There are many different types of devices in this field. Some that perform Neuromuscular electrical stimulation (NMES) while others that perform Transcutaneous electrical nerve stimulation (TENS). The aim of this device was to create a budget conscious unit that could work just as well with the same features of other devices. Neuromuscular Electrical Stimulation (NMES) is a non-invasive, non-addictive means of muscle rehabilitation after injury, surgery or disease. Patients with a wide range of orthopedic and neurologic diagnoses can benefit from NMES, which applies customized electrical stimulus to cause a muscle to contract. “The major benefit of integrating NMES in the treatment of patients is the reduction of total rehabilitation time and concomitant reduction in the total cost of recovery.” (Electrotherapy in Rehabilitation, Meryl Roth Gersh, 1992). Electrical stimulation is simply the application of electrical pulses to the body, be it for function or therapy. The classical example is that of the cardiac pacemaker. The range of clinical uses of electrical stimulation is wide and includes: pain relief (often known as TENS - Transcutaneous Electrical Nerve Stimulation) maintaining or increasing range of movement ( NMES ) muscle strengthening ( NMES ) facilitation of voluntary motor function ( NMES ) orthotic training or substitution ( NMES ) At the electrode-tissue interface a conversion occurs between the current of electrons passing through the wires and the current of ions moved within the tissue. Then through this externally applied current, the depolarization of nerve and muscle to threshold is produced by the transport of ions across the tissue membrane. The factors determining whether sufficient current flows to cause an action potential are: impedance of skin and body tissues electrode size and position Johnson Page | 1 stimulation parameters The conductivity of body tissues is related to their water and ion content. Muscle is a good conductor, but conducts much better in the longitudinal direction of its fibers than in the transverse one, while adipose tissue is a good insulator. Thus electrode position can affect the current required for stimulation. With surface electrical stimulation the effect of the electric current (the current density) diminishes with depth of tissue, as illustrated below: Figure 1: Representation of Current Density From: Functional Electrical Stimulation: A Practical Clinical Guide (2nd Edition). Benton, Baker et al., 1981 The electrical pulses applied may be: Monophasic Johnson Page | 2 The monophasic waveforms tend to be asymmetric biphasic as the net charge built up in the body by the waveform discharges: Charge Balanced When charge balanced pulse types are used no net charge is introduced to the body. This is particularly important for some types of denervated muscle stimulation and for implanted electrodes, where electrolysis at the electrode tissue interface could take place if there was a non-zero net charge. The various types of waveforms that are applicable to be implemented are as follows: Figure 2 : (Sine waves of type monophasic and biphasic were also implemented without damping to add features) 8 Total Johnson Page | 3 Edmark is a critically damped capacitor discharge, where as the Lown form is an underdamped capacitor discharge. There are three general types of techniques for electro-stimulation: Faradic Electrical Stimulation Faradic stimulation is used for innervated muscle, i.e. when the lower motor neurons are intact. Stimulation is applied via the nerves often at the muscle motor points. The nerves depolarization leads onto muscular contraction. Faradic stimulation can be considered to be ac with pulse widths <1ms (typically around 0.3ms with a frequency <100 Hz (due to the absolute refractory period of normal muscle). The contractions produced can be: approaching near normal voluntary levels of muscle force sustained tetanic It is for these reasons that the majority of functional electrical stimulation techniques require intact lower motor neurons, and use faradic stimulation techniques to achieve the desired muscle contraction. Galvanic Electrical Stimulation This is often known as interrupted dc as it conventionally requires pulsewidths of about 100 ms. It is used to stimulate denervated muscle directly, but at best produces weak tetanic forces. The use of this technique for functional restoration is therefore limited, and with the conventional approach the therapeutic benefits have been considered minimal. However, more recent work has indicated that there are increased, though largely therapeutic, benefits to be gained by using biphasic waveforms of around 10-15 ms pulsewidth and frequencies of about 10Hz Interferential Electrical Stimulation This is used for deep tissues where with faradic type pulses a high, and consequently often painful, stimulation intensity is needed to reach the desired muscles, e.g. pelvic floor muscles. By increasing the frequency the body impedance is reduced and thus the necessary stimulation intensity to ensure depolarization of the deep nervous tissue is lowered. In a simple application two medium frequency signals, e.g. of the order of 3kHz, are applied to the body. The "mixing" of these within the body produce a beat signal with a pulsewidth within the faradic range. This then leads onto nerve depolarization as would be the case with direct faradic stimulation. Johnson Page | 4 Interferential stimulation is not often used for functional neuromotor stimulation as compared with faradic type stimulation, it requires greater energy consumption and often a greater number of electrodes. NMES type devices typically use Faradic Electrical Stimulation to physically fire motor neurons in your nerves and contract muscles physically for the purpose of muscle and motor control retraining. TENS type devices typically use Interferential Electrical Stimulation and mainly use of interferential currents to massage deep tissue without causing contraction of said muscle for the purpose of pain relief. Transcutaneous Stimulation Transcutaneous stimulation takes place on the skin via surface electrodes. The intensity needed varies greatly with the muscle, its condition, the stimulation pulsewidth used and the contraction required, but in some cases, e.g. when stimulating the quadriceps to effect standing, then amplitudes up to around 150 mA are not uncommon. Figure 3: Typical Electrode Positions for Quadricep Stimulation (-ve over motor point) (c) David Ewins 1990 Johnson Page | 5 Figure 4: Typical Electrode Positions for Peroneal Stimulation -withdrawal reflex (c) David Ewins 1990 Monophasic or charge balanced pulse types may be used. Johnson Page | 6 My Design: Future improvements: Fully Isolate both channels Implement a hand trigger Apply for Safety Standards: EN EN60601-1, EN EN60601-1-2, EC 60601-2-10 Specifications: Pulse Current: 0-100 mA Pulse Amplitude: 0 – 40 Volts 8 waveforms (Asymmetric Biphasic Pulse Ready) 2 Channels Stimulation Modes: Synchronous, Constant, and Alternate Adjustable frequency, pulse duration, and timer via software and switch selection 9V DC Battery Pulse width: 50 - 300 microseconds Pulse rate: 2 – 120 Hz Contraction time: 2 - 99 seconds Relaxation OFF time: 2 - 99 seconds Timer: 5-90 minutes Overcurrent Protection (blocks current > 100mA) Microcontroller controlled, except wave amplitude which is user controlled The device will have two output channels that can operate in three different modes of operation (stimulation): Synchronous, Constant or Alternate. The main focus of the design is on the power circuit, control circuit and the amplifier circuits for outputting the appropriate signals at the appropriate and predefined (by the user ) waveforms and intensities. The purpose of this design is the challenge to build a lower cost NMES machine comparable to what is on the medical market (©EMPI $1500.00). The hardest part of the design is to create an output signal that is linear and not stepped for precision and comfort to a patient. The basics treatment of this device is that it should be a handheld device and easily useable from a medical practitioner like Doctor of Physical Therapy or a home user with just a brief usage training. Johnson Page | 7 Figure 5: Full NMES circuit Johnson Page | 8 Figure 6: 9v to positive/negative 5v Supplies Johnson Page | 9 Figure 7: Boost converter 9v to 42v DC I did not have the correct part in my CAD program here is what the circuit is supposed to look like: This is run in non-bootstrapped mode for the higher output voltage threshold. Johnson Page | 10 Figure 8: Control Circuit Initially my circuit called for four PWM channels, but under revised circuit design I got it down to two. This PIC microcontroller is a tad more powerful than required and can easily be substituted for a cheaper model. Figure 9: 50%PWM to SINE to SQUARE Johnson Page | 11 Figure 10: Preamp ( 0 < Gain < 1 ) In order for the next final dual stage amplifier to correctly amplify the signal, the 5V,peakpeak has to be considerably de-amplified to a small signal representation. Figure 11: Final Dual Stage High variable gain amplifier circuit Johnson Page | 12 The bottom left Potentiometer/Switch is available to the user to switch on the devices power and control amplification of the waveforms to the output pads. Now this is another amplifier I did not have the correct model in my CAD program so here is the correct representation of the first stage: VG is linear gain control and should be a value between 0 and 2V DC. Johnson Page | 13 Figure 12: Waveform selection circuit All three of these tactile switches select through a mechanism deciding which signals make it from the original Sine wave to the preamplifier then on to Main two stage output amplifier. These switches control both channels at the same time. (Type of Damping: Edmark/Lown) (Dampening: On/Off)(Mono/Bi Phasic) Figure 13: The output interconnect This is the output interconnect, CH1 – GND - CH2 - GND Notice both channel one and channel two have output overcurrent protection via Resettable Fuse PTC Current Cutoff Thermistors. The way these devices operate are they act as very small resistance resistors (typically 1.2 ohms) and once a certain current threshold is hit ( In this case 100mA) they begin to heat up and as they heat up their resistance goes up drastically towards infinite cutting off current flow out of the device. Johnson Page | 14 Conclusion Currently in industry the most prominent manufacturer of these types of medical devices are some noname companies that create cheap products and EMPI, Inc. which is a large biomedical company. They offer a NMES unit that goes for the average cost of $1500 USD new. With some basic revisions, implementation and testing of my design you could produce an NMES unit for much less, in the neighborhood of $40 – $100 USD. Electrode lead wires to be used: Koalaty Products, Inc. 20-032-01. Research Due to only having three days of design time and one day to work on a final report, much of the information and images contained in this report were found from external sources. I edited some of these images for my own use. I do fully take credit for my circuit design and much of the knowledge presented in this report. I did not however do the biomedical research myself; I only read and studied it. Research Sources: Electrotherapy in Rehabilitation, Meryl Roth Gersh, 1992 Atlas of Human Anatomy, Second Edition, Frank H Netter, 1997. http://www.empi.com/ http://www.surrey.ac.uk/eng/research/biomedical/de_page/fes_intr/ http://www.monroecc.edu/depts/PSTC/backup/parabiph.htm http://www.arroncake.net/circuits/vinertr.asp Dr. Denny A. Patel, PT, DPT, CSCS Biography: Daniel B Johnson http://www.danielbjohnson.net/ Johnson.danielb@yahoo.com Graduated in 2003 from Foothill High School in Santa Ana, CA. Attended California State University, Fullerton as an Undergraduate and obtained a Bachelors of Science, in Electrical Engineering in 2009. I have just recently started the Masters program at California State University, Fullerton with an emphasis in Control Systems Engineering. Interest include: Embedded Systems, Control Systems, Fast Prototyping, and Robotics. Johnson Page | 15