FRACTURES
advertisement

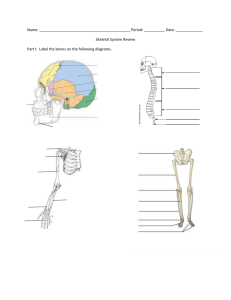
FRACTURES By Mahima Charan 4th Year Medical Student Key Points I. Definition; A disruption in the continuity of a bone. II. Open Vs Closed III.Location IV. Simple/Comminuted V. Types/Pattern VI. Displacement/Angulation/Shortening Open Vs Closed Open ( “open to the air”) A fracture in which bone penetrates through the skin . Look out for an open wound/soft tissue laceration. Closed Fracture with intact overlying skin. Location Can be described in many ways; 1. Segmental (long bones) Epiphysis, Metaphysis, Diaphysis 2. Thirds (long bones) Proximal 1/3, Middle 1/3, Distal 1/3 3. Anatomical landmarks Head, Neck, Body, Condyle, Base Neck of Femur e.g. anatomical landmarks to describe fractures Simple Fracture; The fracture passes at right angles/<30o to the shaft of the long bone Transverse (Tibia) A fracture that consists of the bone breaking into 2 fragments The fracture passes at an angle oblique (> 30o) to the shaft of the long bone Oblique (Metartarsal) Simple spiral Fracture This fracture of the tibia resulted from a twisting injury. The fracture line spirals along the shaft of the long bone Comminuted A bone injury that results in >2 separate components is known as a commented fracture. This is also known as a multifragmentary fracture. Proximal humeral shaft Fracture Displacement Displacement of fractures is defined in terms of the abnormal position of the distal fracture fragment in relation to the proximal bone. Types of displacement include1. Angulation 2. Rotation 3. Shortening 4. Impaction and Distraction Angulation and Rotation To describe fracture angulation the direction of the distal bone and degree of angulation in relation to the proximal bone should be stated. Medial angulation can be termed ‘varus’ and lateral angulation ‘valgus’ Rotation of a long bone may be internal or external The fracture on the left has resulted in angulation of the distal component. The fracture on the right has resulted in rotation of the distal component Shortening Proximal migration of the distal fracture component results in shortening of the overall bone length. An oblique fracture is more readily shortened than a transverse fracture, which would need to be fully 'offended' before it can shorten. The fracture on the left is displaced without shortening The fracture on the right is both displaced and shortened Impaction and Distraction A fracture resulting in increased overall bone length, is due to distraction (widening) of the bone components. If there is shortening of bone without loss of alignment, the fracture is impacted. The bone substance of each component is driven into the other. The left image shows fracture widening or distraction. The right image shows a line of increased density due to fracture impaction. Let’s have a look at some common fractures….. Humeral fracture Elbow The lateral image shows the anterior fat lad is raised way from the humerus but does not show a fracture. Posterior fat pad visible- ALWAYS ABNORMAL A fracture of the radial head is visible on the AP image Monteggia vs Galeazzi A Monteggia injury; fracture of the ulna shaft with dislocation of the radial head at the elbow. The radiocapitellar line should pass through the midline of the capitulum of the humerus. A Galeazzi injury is a fracture of the radial shaft with dislocation of the ulna from its articulation with the radius at the distal radio-ulnar joint. Monteggia Colles Fracture Common injury in elderly people with low bone density. njury comprises a transverse fracture of the distal radius with dorsal displacement and shorten The fracture is often accompanied by a fracture of the ulnar styloid. Classical presentation is “Fall on an outstretched hand” Normal Hip Anatomy If displaced, may present with shortened and externally rotated leg! Tx- I/II Put in a screw III/IV Austin Moore ( hemiarthroplasty) Garden Classification for NOF Fractures Avascular Necrosis scaphoid fractures ( tenderness in anatomical snuffbox) (greater risk in intracapsular fractures and Scaphoid Fracture Principles of Management I. First aid- If open ( clean wound, debride, tetanus injection) Analgesia for pain associated with fracture II. Immobilise (traction, splints, casts) III. Reduction ( if displaced) IV. Active Rehabilitation DON’T FORGET YOU NEED 2 VIEWS ON AN XRAY! Open Reduction Internal Fixation Immobilise ( e.g. Kirschner wires Fracture Complications Soft tissue injury and neurovascular compromise Malunion Non-union Avascular Necrosis Osteopenia Compartment Syndrome Sudecks atrophy (Complex regional pain syndrome) Thankyou very much! Mahima Charan