pulmonary blood flow
advertisement

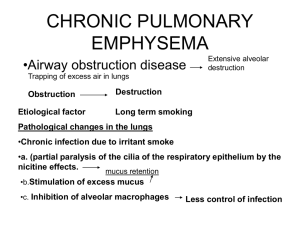
pulmonary blood flow Dr.Wael Abd Elfattah Lecturer of chest disease faculty of medicine - Ain Shams univeristy Ibn al-Nafis (1213–1288) was an Arab physician who made several important contributions to the early knowledge of the pulmonary circulation. He was the first person to challenge the long-held contention of the Galen School that blood could pass through the cardiac interventricular septum, and in keeping with this he believed that all the blood that reached the left ventricle passed through the lung What is pulmonary circulation? • Pulmonary circulation is the movement of blood from the heart, to the lungs, and back to the heart again. • This is just one phase of the overall circulatory system. • It carries waste-rich blood and oxygen depleted blood away from the heart and to the lungs and returns oxygenated blood back to the heart. • Deoxygenated blood exits the heart through the pulmonary arteries and enters the lungs and oxygenated blood comes back through pulmonary veins. The blood moves from right ventricle of the heart to the lungs back to the left atrium. What is the importance and functions of pulmonary circulation? • • • • • • Gas exghange. Blood reservoir. Metabolic function. Filtration of thrombi. Defensive function. Drug administration. What is difference between pulmonary and systemic circulation? Pulmonary vessels pressure Resistance Pulmonary circulation systemic circulation Thinner ( 30% ) less elastic and smooth muscle fibers Thicker More elastic and smooth muscle fibers 25/8 mmHg 120/80mmHg 1.8 mmHg/L/min (About 10% of systemic) 18 mmHg/L/min What are characteristics of pulmonary circulation? • low pressure • low resistance • High capacitance What are factors affecting pulmonary blood flow? • Neural control: -Sympathetic stimulation VC of pulm. vessels -Parasympathetic stimulation VD of pulm. vessels • Chemical control: -Mediators → VC:catecholamines-angiotensin ǁThromboxanA2- PGF2α -Mediators → VD: Histamin- acetylecholine- PGI2 • Blood gases control: - Hypoxia and hypercapnia VC of pulm. vessels, unlike most of the vessels in the body !!! What are other factors affecting pulmonary blood flow? • Gravity. • Respiratory movement. • Cardiac output. What are factors affecting fluid movement across pulmonary capillary? • The Starling equation can be applied to the pulmonary microcirculation in the same way as any other capillary bed. fluid movement = k × (ΔP – Δπ) • Hydrostatic pressure gradient • Oncotic pressure gradient • capillary permeability co-effiecent Typical values for the Starling’s Forces in Pulmonary Capillaries Capillary hydrostatic pressure (Pc) is 13 mmHg (arteriolar end) to 6 mmHg (venous end) but variable because of the hydrostatic effects of gravity esp in the erect lung. • Interstitial hydrostatic pressure (Pi) - Variable but ranges from zero to slightly negative. • Capillary oncotic pressure = 25 mmHg (Same as in systemic capillaries) • Interstitial oncotic pressure = 17 mmHg (This is estimated from measurements on lung lymph) The net force favors a small continuous leak of fluid out of capillaries into interstitial space.This fluid travels through the lung lymphatic drainage. Safety Factors Preventing Pulmonary Oedema • Increased lymph flow: Increased fluid filtration causes increased lymph flow which tends to remove the fluid. • Decrease in interstitial oncotic pressure (oncotic buffering mechanism): When filtration increases, the albumin loss in the filtrate decreases. This combined with the increased lymph flow washes the albumin out of the interstitium and interstitial oncotic pressure decreases. This protection does not work if the capillary membrane is damaged eg by septic mediators. • High interstitial compliance: A large volume of fluid can accumulate in the gel of the interstitium without much pressure rise. • Surfactant prevent alveolar collapse. These safety mechanisms are quite effective especially in preventing pulmonary oedema associated with rises in capillary hydrostatic pressure. It has been estimated that the capillary hydrostatic pressure can rise to three times normal before alveolar flooding occurs. Surfactant assists in the prevention of alveolar flooding also. Pulmonary edema • Def: It is extra vascular accumulation of fluid in the lung.( frist in the interstitium and later in the alveoli) • Causes: • Increased capillary Hydrostatic pressure • Decreased interstitial Hydrostatic pressure • capillary permeability • Lymphatic obstruction • Oncotic pressure gradient • Other conditions. Ventilation Definition: • The movement of air between the atmosphere and alveoli and the distribution of air within the lungs to maintain appropriate concentrations of oxygen and carbon dioxide in the blood. • In normal resting individuals, alveolar ventilation is about 4.0 L/min and pulmonary blood flow is about 5.0 L/min. • In normal individuals, alveolar ventilation and blood flow are each distributed uniformly to the gas-exchanging units • Healthy subjects seated in the upright posture breathing quietly from FRC show differences in regional ventilation. • Ventilation is directed preferentially to the bases of the lungs. Explanation for Differences in Regional Ventilation • In the upright lung intrapleural pressure varies from the top to the base of the lungs. • the intrapleural pressure at the apex of the lung is about – 8 cm H2O and at the base about – 1.5 cm H2O. This means that the alveoli at the apex are exposed to a greater distending pressure (PAPpl= 0 - -8= 8 cm H2O) compared to those at the base (PA-Ppl= 0 - 1.5= 1.5 cmH2O). It is this difference in initial volume that results in the preferential distribution of ventilation to the alveoli at the base of the lungs. • The alveoli at the base of the lung have a smaller initial and being relatively more compliant, the alveoli at the base fill to a greater extend for a given change in intrapleural pressure during inspiration compared to the alveoli at the apex. • Conversely, the alveoli at the apex are exposed to a larger distending pressure, being relatively less compliant and fill less during inspiration. Distribution of Perfusion in the Normal Upright Lung • Pulmonary blood flow is preferentially directed to the base of the lungs. This distribution is dependent on three relative pressures: alveolar pressure, pulmonary arterial pressure and pulmonary venous pressure. • Three functional zones based on these pressure relationships where first suggested by John West and characterized in experiments on excised, perfused upright animal lungs under low arterial perfusion pressures. • The most apical region, zone 1: where PA>Pa>Pv, alveolar pressure exceeds vascular pressures resulting in capillary collapse and no blood flow. The alveoli in this zone do not participate in gas exchange and are part of the lung’s alveolar dead space. • In healthy subjects under normal perfusion pressures, zone I is not present because arterial pressures is just sufficient to raise blood to the top of the lung and exceed alveolar pressure. • Zone I may be present if pulmonary arterial pressure is reduced (followingsevere hemorrhage) or if alveolar pressure is raised (during positive pressure ventilation). • In Zone 2: where Pa>PA>Pv, there is intermittent blood flow only during the pulmonary arterial pressure peaks because the systolic pressure is then greater than the alveolar air pressure, but the diastolic pressure is less than the alveolar air pressure • InZone 3: where Pa>Pv>PA, there is continuous blood flow because the alveolar capillary pressure remains greater than alveolar air pressure during the entire cardiac cycle • Normally, the lungs have only zones 2 and 3 blood flow—zone 2 (intermittent flow) in the apices, and zone 3 (continuous flow) in all the lower areas. Ventilation Perfusion Ratio • Both airflow and blood flow increase down the lung, but the differences in perfusion are greater than the differences in ventilation. Blood flow shows about a 5-fold difference between the top and bottom of the lung, while ventilation shows about a 2-fold difference. Blood flow is proportionately greater than ventilation at the base, reflecting a lower V/Q ratio and ventilation is proportionately greater than blood flow at the apex, demonstrating a higher V/Q ratio • The alveolar partial pressure of oxygen and carbon dioxide are determined by the ratio of ventilation to perfusion. TYPES OF V/Q RELATIONSHIP • IDEAL V/Q or V/Q OF 1 • An ideal is a condition where in the respiratory unit receives equal amount of ventilation and perfusion. In this situation gas exchange between the alveolar gas and pulmonary capillary blood is optimal that is why it is known as an ideal . • For example, if a respiratory unit receives 3 lpm of ventilation and 3 lpm of blood flow, then the relationship is 3/3 or 1. IDEAL V/Q or V/Q OF 1 LOW V/Q or V/Q<1 • This condition exists when the respiratory unit receives inappropriate low ventilation relative to its perfusion such as at lung base. • This may be caused by a low respiratory unit ventilation due to low compliance such as in pulmonary fibrosis and lack of surfactant or due to high airway resistance found in asthma and chronic obstructive pulmonary disease. • For example, a respiratory unit receives 2 lpm of ventilation and 3 lpm of blood flow, then the relationship is 2/3 or V/Q less than 1. HIGH V/Q or V/Q>1 • This condition exists when the respiratory unit receives inappropriate low perfusion relative to its ventilation such as lung apical part. • Hypotensive states or a partial obstruction of pulmonary blood vessels present in pulmonary embolism may be responsible for a high V/Q. • For example, a respiratory unit receives 3 lpm of ventilation and 2 lpm of blood flow, then the relationship is 3/2 or V/Q greater than 1. PO2-PCO2 , V/Q diagram • The upper regions of the lungs with higher V/Q ratio have relatively higher PO2s and lower PCO2s compared to the lower regions. • At first glance this may seem to indicate that there is greater gas exchange at the upper regions of the lungs but recall that there is greater ventilation and perfusion to the bases of the lungs and therefore greater gas exchange at the base of the lungs. • Overall this arrangement results in adequate gas exchange but if disease states affect either the distribution of ventilation or perfusion, there will be an increase in V/Q mismatching and gas exchange worsens ZERO V/Q • This conditon exists when the respiratory unit receives no ventilation but perfusion remains normal.(venous to arterial shunt) • This may be caused by alveolar flooding found in pneumonia and ARDS, complete obstruction of the airway, and extrinsic compresion of alveoli present in compression atelectasis due to hydrothorax or pneumothorax. • For example, a respiratory unit receives 0 lpm of ventilation and 3 lpm of blood flow, then the relationship is 0/3 or V/Q = 0. V/Q of Infinity • This condition exists when the respiratory unit receives no perfusion but ventilation remains normal. ( alveolar dead space) • This may be found when there is a complete obstruction of the pulmonary blood vessels. • For example, a respiratory unit receives 3 lpm of ventilation and 0 lpm of blood flow, then the relationship is 3/0 or V/Q of infinity. Compensating mechanisms matching ventilation and perfusion • Alveolar hypoventilation. • Decreased pulmonary perfusion 32 33 36