Mannequins, Clinical Simulations and E
advertisement

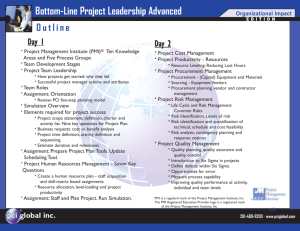
Mannequins, Simulators and E-learning in Medicine Sem Lampotang, PhD Professor of Anesthesiology Center for Simulation, Advanced Learning and Technology Department of Anesthesiology Medical Update University of Mauritius July 25, 2007 Disclosure • Co-inventor of the Human Patient Simulator • Developer of the simulations on the Virtual Anesthesia Machine web site http://vam.anest.ufl.edu/wip.html Acknowledgements • • • • • • • • • • • Thomas H. Maren Foundation - USA Anesthesia Patient Safety Foundation - USA Novo Nordisk - Denmark IBM Thomas J. Watson Research Center - USA GE Healthcare / Ohmeda - USA GaleMed – Taiwan Prodol/AirTraq - Spain Enturia - USA Molecular Products – United Kingdom Karl Storz - Germany The VAM team Outline • Simulation in Healthcare • Mannequin simulators • Web simulation and e-learning Deaths from medical error • Institute of Medicine’s 1999 report “To err is human” estimates that medical error causes between 44,000 to 98,000 deaths each year in the United States • Equivalent on the low end to 2 jumbo jets full of passengers crashing every week! Reliable Performance is Elusive…. Troglitazone LFT monitoring IRS Tax Advice ACE-I for EF <40% and yearly HbA1C for DM B blockers after AMI 1,000,000 Restaurant bill mistakes 100,000 Six Sigma Sigma Values +/- 1 = 68.26% +/- 2 = 95.44% +/- 3 = 99.73% 10,000 Point of Inflection Airline baggage handling p(d) Negligence in hospitals ABX for Viral URI 1,000 p(d) s1 Defects per Million 6 100 5 4 3 2 1 LSL A 6 Sigma Process includes 6 standard deviations between the mean and the spec limit 10 1 M 2 3 4 5 6 USL 6 sigma accuracy = 3.4 defects per million Anesthesia deaths Airline safety 1 0 1 2 3 4 5 6 Sigma Level 6 Rene Alamberti, Ann Intern Med. 2005;142:756 Criteria for justifying the expense of simulation (in any field) • Errors are expensive • Reality is dangerous • Events are rare Why simulation? • Learning in clinical medicine has traditionally followed an apprenticeship model: “see one, do one, teach one” • Rate of discovery and creation of new knowledge keeps on accelerating, including in healthcare – apprenticeship model no longer tenable • Learning by doing • Hands-on learning Mannequin Simulators • • • • Consumes O2, produces CO2 Clinical signs Monitored physiological signs Mathematical models of pharmacokinetics/pharmacodynamics • Cardiopulmonary model • Can simulate different disease states Gainesville Anesthesia Simulator Human Patient Simulator Respiratory System Respiratory System Respiratory System O2 CO2 N2 N2O Invasive and non-invasive blood pressure Electrocardiogram Multi-compartment model • • • • • • • • • • • • • • • Left atrium Left ventricle Intrathoracic artery Extrathoracic artery Vessel rich group tissue Muscle group tissue Fat group tissue Extrathoracic vein Intrathoracic vein Right atrium Right Ventricle Pulmonary artery Ventilated lung tissue Shunted lung tissue Pulmonary vein Nervous System Nervous System Urinary System Drug Recognition Drug Recognition Installations worldwide • http://www.meti.com • HPS Installations Some problems spanning the entire healthcare system… • • • • • Industry education Education of regulatory body personnel User education and training Patient education issues Patient safety issues involving healthcare systems Transparent Reality (TR) Simulation • Invented at UF • “Transparent reality simulation” coined at UF • Identified as 4 – 5 years away from general adoption by Educause Horizon Report 2006 Some problems … • Industry education – Basic science and R&D – Engineering/production/pre-market approval (Mannequin Simulator-Based Usability studies) – Marketing/Sales force training • Education of regulatory body personnel (FDA) Some problems … • User education and training – Reality is opaque and complex and can get in the way of learning – Incompatible international standards – Medical error • Human error 3 times more common than equipment failure for anesthesia machines (Closed claims study) • Failure to check, failure to detect, failure to teach – “Black hole” users/ Difficult users • Are clinicians really using the training material? • How much are they really getting? What do they find hard? – Credentialing • Can clinicians really use a given product safely? – Equitable access to essential patient safety materials Some problems … • Patient education issues – Patient compliance • Non-compliance major reason for organ transplant rejection Some problems … • Patient safety issues; Systems issues – Defining the problem • Identifying the problem • Quantifying the problem • Investigating causal factors and possible solutions – A FMEA (Failure Mode Effects Analysis) exercise has to take into account the entire system including user training, competency, vigilance and fatigue UF Virtual Anesthesia Machine Web Site http://vam.anest.ufl.edu/wip.html The UF VAM web site will be used as a concrete example of the different forms of web applications that address some of the previously identified problems. Transparent reality simulation Blackbox opaque simulation TR Provides Better Learning 3 Quality Score (max. 4.0) Transparent VAM 2.5 Opaque VAM 2 1.5 1 0.5 0 Component Identity Component Function System Dynamics Some problems … • Patient education issues – Patient compliance • Non-compliance major reason for organ transplant rejection Some problems … • Patient safety issues; Systems issues – Defining the problem (anesthesia machine pre-use check survey) • Identifying the problem • Quantifying the problem • Investigating causal factors and solutions – Survey results • 20% check before every case, 50% only first case of the day, what about remaining 30%? Does this really work? • The web provides democratic “peer review” where everyone votes with their mouse. • #1 on Google for “anesthesia machine” • #1 on Google for “airway device” • #1 on Google for “fospropofol simulation” • #1 on many more terms and search engines • Webalizer stats • AwStats stats Equitable access to essential patient safety materials Questions? • Email: sem@anest.ufl.edu • Simulation portfolio URL: http://vam.anest.ufl.edu/wip.html