Intramuscular Injections IM's

Chapter 21 Perry & Potter
•
•
Order: ½ NS @ 125cc/hr
Drop factor: 15 gtt/ml
Drop rate:
– 31.25 gtt/min (31-32)
125 cc/hr x 15 gtt/ml = 31.23 (31-32)
60 min
•
•
Order: D5 ½ NS @ 100 ml/hr
Drop factor: 10 gtt/ml
Drop rate:
– 16.6 gtt/min (16-17)
Order: Maxeran 10 mg IVPB ½ hour ac meals
Available: 10 mg/ml
Further dilute: 50 ml NS, infuse over 15 min
What is the rate:
◦ 200 ml/hr
◦ 50 ml X ?
15 min 60 min
= 200 ml/hr
What is the drip rate (drop factor 15 gtt/ml):
◦ 50 gtt/min
Order: Pantoprazole 40 mg IV now
•
•
•
•
Available: 40 mg vial
Reconstitute with 10 ml NS (final concentration 4 mg/mL).
Reconstituted solution may be given intravenously (over 2 minutes) or may be added to 100 mL D
5 minute infusion).
W, NS, or LR (for 15-
Stable in D
5
W, LR, NS.
Y-site administration: Incompatible: Midazolam, zinc.
•
•
•
How much do you add to the minibag:
– 10 ml
What is the rate:
– 440 ml/hr
What is the drip rate with drop factor of 15 gtt/ml:
– 110 gtt/min (this will be difficult to count)
Primary line: NS with 40 meq KCL @ 75 ml/hr
Order: Pantoprazole 40 mg IV now
•
•
•
•
•
What do you need to know before you begin?
Reason for primary infusion & reason for IV med
Drug information (expected & unexpected)
Client’s history & allergies
Client’s knowledge of medication
IV compatibility!!!
IV therapy
◦ Monitoring an IV Site, checking Infusion Rate, and
Changing an IV Solution Container
◦ Replacing IV Solution Container and Administration
Tubing
IV Medications
◦ Administrating IV Medications by Piggyback
Infusion
Order: Lovenox 40 mg SC OD
•
•
Available: 300mg/3ml (100mg/ml)
Info: Lovenox is a sterile aqueous solution containing enoxaparin sodium, a low molecular weight heparin.
Lovenox® is indicated for the prophylaxis of deep vein thrombosis (DVT), which may lead to pulmonary embolism
(PE)
•
•
•
How much do you withdrawl?
– 0.4 ml
Identify the appropriate syringe:
– 1 ml
Where are you going to administer this medication?
– Outer aspect of abdomen (never arms)
•
Mixing Two Insulin's in One Syringe
•
Important information you need to know?
– If insulin’s are compatible
– Is it safe to give (know clients blood sugar)
– Insulin(s) information (onset, peak, duration)
– Draw up rapid acting insulin first (unmodified)
– Check dose with RN/instructor
– Know S&S of hyper/hypoglycemia
– Injections sites
•
•
•
•
•
Faster absorption
Less danger of causing tissue damage
Risk of injecting into blood vessels exists
Muscle is less sensitive to irritating and viscous drugs
Large well developed muscles (adults) can tolerate as much as 5 ml of medication (infants
0.5-1ml, toddler 1-2ml, preschool 2-3ml, adolescents 3-5ml)
Vastus lateralis and ventraogluteal sites used in infants
Deltoid used in well developed children and adolescents
In estimating needle length in children, grasp muscle between thumb and index, needle length showed be half the distance between fingers.
Insert needle as close to 90 degrees as possible
Rotate sites to decrease risk of hypertrophy
Gauge often determined by length
Most water soluble medications use:
◦ 22-27 gauge needle
More viscous medications use:
◦ 18-25 gauge needle
Older or cachectic clients may need shorter smaller gauge needle
Average length:
◦ Children: 5/8 – 1 inch
◦ Adults: 1- 1 ½ inches
Assess integrity of a muscle prior to injection
Help client assume a position that reduces strain on the muscle.
Area must be free of infection or necrosis, bruising or abrasions, underlying bones, nerves & major blood vessels.
Review order (medication rights)
Obtain medication information
Review history and assess factors contraindicating injection (muscle atrophy, shock, impaired circulation)
◦ What would you do if contraindicated?
Call prescriber for alternative route!
Medical history, allergies, medication history
Client’s knowledge/concerns
6 rights, 3 checks
Prepared correct dose from vial/ampule
Replace needle with needle for injection
◦ Children: 5/8 – 1 inch
◦ Adults: 1- 1 ½ inches (22-27 gauge)
: 1 ½ inch (18-25 gauge) viscous medications
Check arm band/compare with MAR
Explain procedure, locate site, BE CONFIDENT
A deep site, situated away from major nerves and blood vessels, less chance of contamination in incontinent clients or infants because it is away from rectum.
Easily identified by prominent bony landmark.
Safe for all clients
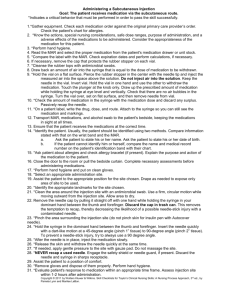
Land marking (p. 725):
◦ Place heel of hand over the greater trochanter of the client's hip
right hand over left hip
left hand over right hip
Point thumb towards client's groin
Index finger over anterior superior iliac spine
Extend middle finger back along the iliac crest toward the buttock
Create a triangle between index finger, middle finger and the iliac crest (towards the buttocks)
Inject in the middle of this triangle
Flexing of the knee and hip helps person to relax
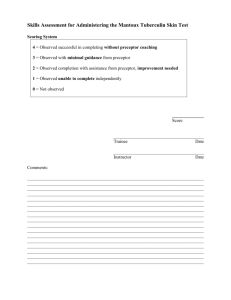
Vastus Lateralis - lacks major nerves and blood vessels, rapid drug absorption, developed muscle
◦ Site used for giving children IM medication
(preferred for immunizations)
◦ Client should lie with the knee slightly flexed or in a sitting position
Land marking (p.725):
Located on the anterior lateral aspect of the thigh
◦ Handbreadth above the knee to a handbreadth below the greater trochanter of the femur.
◦ In width, from the midline of the thigh to the midline of the thighs outer side.
◦ Inject into the middle third of the muscle.
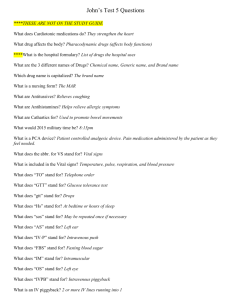
Not well developed in most adults & children
(not recommended for use in infants or children)
Radial & ulnar nerves & brachial artery lie within the upper arm along the humerus
Used when other injection sites are inaccessible
Used for small amount of drugs (2 ml or less)
Landmarking (p. 726):
Expose upper arm
Palpate lower edge of the acromion process
(base of triangle)
Inject in the middle of the triangle (3-5 cm below the acromion process)
No longer a recommended site
Runs risk of striking underlying sciatic nerve, greater trochanter, major blood vessel.
Often used by nurses in hospitals (4 quadrant landmarking), practice is slowly changing
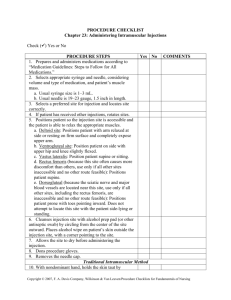
Minimizes tissue irritation by sealing the drug within the muscle tissues and decreasing pain.
Recommended technique for all IM’s when possible
Privacy
Wash hands
Expose only required area
Select appropriate injection site & ensure client is comfortable
Landmark site
With nondominant hand, pull skin 2.5-3.5 cm down or lateral (Z track), hold this position until medication is administered.
Cleanse site with antiseptic (center and rotate outward ~
5 cm)
Gauze in nondominant hand
Remove cap (pull straight off)
Hold syringe like a dart
Inject quickly at 90 degrees
Hold lower part of syringe to stabilize syringe
Pull back on plunger 5-10 sec, if no blood inject medication slowly (1 ml/10 sec)
Wait 10 sec, slowly withdrawl needle, place gauze over site
Assess site
Observe response to medication
Record on MAR, record response (i.e prn/STAT)
Document and report undesirable effects
Video: Intramuscular Injection
1.
Order: Demerol 50 mg IM q4h, prn
Order: Gravol 25 mg IM, q4h, prn
Supplied :
◦ Demerol 50 mg / ml (ampule)
◦ Gravol 50 mg / ml (vial)
How much do you need of each?
◦ Demerol: 1 ml
◦ Gravol: 0.5 ml
(Draw up medication from vial first, using filtered needle)
2. Order:
Diphenhydramine
25mg IM stat
Supplied: 50 mg/ml
3. Order:
Dimenhydrinate 50mg
IM/IV/PO q4-6 h prn
Supplied 50 mg/ml
Order: Solumedrol 100 mg IM stat
Directions for Reconstitution
Available 40 mg: Aseptically add 1 mL Bacteriostatic Water for Injection
Available 125 mg: Aseptically add 2 mL Bacteriostatic Water for Injection
How much do you draw up in the syringe?
◦ 1.6 ml
125 mg X 100 mg
2 ml ?
= 1.6 ml
Or
Dose X Stock 100 mg X 2ml = 1.6 ml
Have 125 mg
Next Lab: Sterile Dressings
Perry & Potter: Chapter 37 & 38