the pancreas - Orange Coast College
advertisement

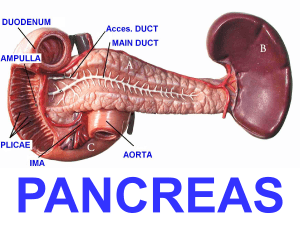
THE PANCREAS I. Introduction/General Information A. Located in epigastric & left hypochondriac regions B. Dimensions: 1. 5 - 6” length x 2. 1-1/2” width x 3. 1/2 - 1” thick C. Lies retroperitoneally at ~T-12/L-1 to L-3 The Pancreas in situ Right lobe of liver Falciform ligament Gallbladder Pancreas Duodenum L-3 Pancreas, Introduction, continued … D. Head fills concavity of duodenum E. Body crosses left kidney F. Tail reaches hilus of the spleen G. Related anteriorly to transverse colon Pancreas in situ Duodenum Head of Pancreas Pancreas, Introduction, continued … H. Aorta, IVC lie posterior I. Uncinate process: a. Lies posterior to SMA and SMV b. Lies anterior to aorta J. Neck lies anterior to SMV, with pylorus just above Venous Drainage of the Pancreas IVC SMV Introduction, continued L. Body related posteriorly to left crus, left adrenal, left renal vein, and splenic vein K. Celiac Axis (trunk, artery) lies superior to body II. Detailed Anatomy A. Landmark structures 1. Splenic Artery: a. Branch of celiac trunk b. passes right to left c. Course is along upper margin of body and tail Detailed Anatomy, con’t… 2. Hepatic Artery: a. Branch of celiac trunk b. courses left to right c. along upper margin of neck and head 3. Superior Mesenteric Artery: at its origin from aorta, points at body of pancreas Arterial Supply to Pancreas Proper Hepatic Artery Common Hepatic Artery Superior Mesenteric Artery Landmark structures, continued … 4. Splenic Vein: a. runs parallel to artery b. on posterior surface of pancreas c. Terminates in portal vein Landmark structures, continued … 5. Superior & Inferior Mesenteric Veins: a. pass (inferior to superior) deep to pancreas b. merge with splenic vein c. Terminate in portal vein Landmark structures, continued … 6. Common Bile Duct: a. passes behind first portion of duodenum b. then through head of pancreas c. Terminates at ampulla of vater Detailed Anatomy continued … B. Head of Pancreas 1. Important clinically because: a. Numerous ducts and vessels traverse it b. Carcinoma usually located here Head of Pancreas, Detailed Anatomy, continued … 2. Tumor will compress surrounding structures a. First indication may be jaundice b. Tumor may compress duodenum c. May involve local vessels *Metastases may spread through these vessels* Head of Pancreas, Detailed Anatomy, continued … 3. Lymphatics from head of pancreas a. Drain to celiac nodes b. metastases may follow lymph c. Metastases may spread via lesser omentum to liver d. Some terminate in lumbar nodes Head of Pancreas, Detailed Anatomy, continued … 4. Vessels supplying head of pancreas a. Superior & inferior pancreaticoduodenal arteries b. Both divide into two parallel vessels c. one anterior and one posterior to head Head of Pancreas, Detailed Anatomy, continued … 1. Anterior branch of pancreaticoduodenal artery a. superior branch: anterior superior pancreaticoduodenal artery b. inferior branch: anterior inferior pancreaticoduodenal artery Head of Pancreas, Detailed Anatomy, continued … 2. Posterior branch of pancreaticoduodenal artery a. superior branch: posterior superior pancreaticoduodenal artery b. inferior branch: posterior inferior pancreaticoduodenal artery **extensive blood supply** Anterior Pancreaticoduodenal Artery •Branches are continuous with one another •Superior branches originate from the GDA •Inferior branches originate from the SMA Detailed Anatomy, continued … C. Body & Tail of Pancreas: 1. Supplied by splenic artery 2. Have three surfaces: a. Anterior surface 1. Concave 2. Deep to stomach 3. Separated from stomach by lesser sac of peritoneum (aka omental bursa) Anterior surface of pancreas Epiploic foramen Anterior surface of pancreas Lesser sac, continued … 4. Lesser sac bounded by: a. Liver, superiorly b. Below, extends to greater omentum c. Anteriorly: lesser omentum, stomach, greater omentum Lesser sac, continued … d. Posteriorly: greater omentum transverse colon, transverse mesocolon e. Laterally: 1. Foramen of Winslow on right 2. Spleen on left Detailed Anatomy, continued … f. Foramen of Winslow (AKA: Epiploic Foramen): 1. Lies between greater & lesser sacs of peritoneum 2. posterior to free edge of lesser omentum 3. close to porta hepatis Three Surfaces, continued … 2. Posterior surface: a. b. c. d. e. f. separated from vertebrae by Aorta Splenic vein Left kidney and renal vessels Left adrenal gland Left Crus of diaphragm SMA and SMV Three surfaces, continued … 3. Inferior surface of Pancreatic body: a. Rests on duodeno-jejunal flexure b. Left extremity (tail) 1. Rests on splenic flexure 2. Abuts hilus of spleen Detailed Anatomy, continued … D. Pancreatic Duct System 1. Pancreatic Duct (of Wirsung) a. Course is left to right b. Receives numerous small ducts c. @ neck of pancreas, duct turns inferior, posterior & to the right d. AKA “main pancreatic duct’ Duct of Wirsung (Main pancreatic duct) Pancreatic Duct System, continued … d. joins CBD at Ampulla of Vater 3 - 4” below pylorus e. results from fusion of ducts during fetal development 1. One from ventral pancreas 2. One from dorsal pancreas (see Netter’s Embryology, p. 142, for Pancreas development) Duct of Wirsung Duct of Wirsung Pancreatic Duct System, continued … 2. Duct of Santorini: a. accessory pancreatic duct b. Not universally identified c. joins duodenum @ minor papilla d. part of duct from dorsal pancreas Duct of Santorini Pancreatic Duct System, continued … 3. In 10% of population a. ducts fail to fuse b. result is drainage of tail, body, & most of head through minor papilla c. Not pathological III. Scanning Anatomy A. Depends on recognition of pancreatic margins B. Sonography best used as screening procedure 1. May be interference from bowel gas (especially in tail region) Scanning Anatomy, continued … 2. Extremely accurate in detection of pseudocysts 3. U/S can show texture of organ 4. By ID-ing vessels, can delineate head, portions of body Scanning Anatomy, continued … 5. U/S can frequently detect dilation of pancreatic duct 6. Splenic Vein: landmark vessel a. usually seen along posterior margin of body, tail b. May be anterior (~30%) Scanning Anatomy, continued … C. Head: 1. SMV outlines medial head to neck region 2. Duodenum & GB outline lateral head 3. Superiorly, delineated by gastroduodenal artery (GDA) 4. Inferiorly, bounded by CBD Scanning Anatomy, continued … D. Further delineation by vascular landmarks: 1. SMA: a. Lies immediately posterior to body, points to it! b. Recognized by echogenic fat collar surrounding vessel Vascular Landmarks of the Pancreas Pancreatic sonography depends largely on identifying surrounding landmark vessels Scanning Anatomy, continued … 2. SMV: a. Delineates medial head b. Larger diameter than SMA c. Lies to right of SMA d. Uncinate process wraps it (and SMA), lies posterior & medial Vascular Landmarks of the Pancreas Venous landmarks of the pancreas include the SMV and renal veins Scanning Anatomy, continued … 3. Left Renal Vein: a. as it enters IVC b. head & uncinate process should lie within 1 – 2 cm c. Landmark vessel posterior to body of pancreas Scanning Anatomy, continued … E. Tail of Pancreas 1. May be visualized through fluid-filled stomach 2. Tail seen as 2-3 cm rounded mass anterior to hilus of left kidney IV. Pancreatic Disorders A. Pancreatitis: diagnosis depends on clinical evidence 1. Usually secondary to biliary tract disease 2. Surgery of biliary tract or stomach, alcoholism are other causes Pancreatitis, Pancreatic Disorders, continued … 3. Infrequent causes: a. Infectious diseases b. Trauma d. Drugs e. Hyperparathyroidism 4. Inflammation may be diffuse or spotty Pancreatitis, Pancreatic Disorders, continued … 5. Important factor is release of protein kinins a. Increase permeability of vessels & cells b. Releases tissue fluid c. Edema may compress vessels d. Tissue damage occurs Pancreatitis, Pancreatic Disorders, continued … 6. WBC’s may increase to 20,000/ml 7. Increase in pancreatic enzymes a. serum bilirubinase (by 25%) b. serum amylase c. serum lipase Pancreatic Disorders, continued … B. Pseudocysts: 1. “False” cysts that may arise a. due to tissue necrosis b. From enzymatic destruction 2. May persist after inflammation subsides 3. Usually near or in pancreas Pancreatic Disorders, continued … 4. Rarely, may be elsewhere a. in abdomen or pelvis b. Rarely, mediastinum 5. Pseudocyst appearance a. unilocular or multilocular b. echoes from pus & cellular debris Pancreatic Diseases, continued C. Acute Pancreatitis 1. Diffuse enlargement 2. Less echogenic due to edema 3. Echogenicity usually > liver parenchyma Pancreatic Diseases, continued … D. Chronic Pancreatitis 1. organ usually appears as small, atrophic 2. Contains scattered echoes from calcifications 3. Primary cause is alcoholism Pancreatic Diseases, continued … E. Dilation of Pancreatic Duct 1. Seen in acute or chronic pancreatitis 2. Frequently associated with neoplasm of pancreas 3. Biliary tract problems Pancreatic Diseases, continued … F. Abscess or Hemorrhagic Pancreatitis 1. Similar in sonographic appearance 2. Hemorrhagic: a. Mass with inhomogeneous texture b. Acute hemorrhage: sonolucent to echogenic c. CT scan used for differentiation Pancreatic Disorders, continued … G. Pancreatic Tumors 1. Malignant tumors usually arise as adenocarcinomas 2. In head of Pancreas: Sx a. Painless jaundice b. Anorexia Pancreatic Tumors, In head, continued … c. Nausea d. Weight loss e. Increased plasma amylase f. Increased alkaline phosphatase g. May involve compression of pancreatic duct, CBD Pancreatic Tumors in the Head Tumors in the head may compress biliary ducts or pancreatic ducts Pancreatic tumors, continued … 3. In Body of Pancreas: Sx a. Gnawing pain radiating to back b. Pain increases after eating or lying down c. Weight loss, anorexia d. Large tumor may compress IVC, portal vein Pancreatic tumors, continued … 4. In Tail of Pancreas: Sx a. Often silent until local metastasis occurs b. May metastasize to: 1. para-aortic lymph nodes 2. spleen Pancreatic tumors, continued … 5. Identified by organ enlargement, subtle echo changes, irregular outline 6. Metastases to stomach, liver & lungs are common 7. Often causes dilation of ducts Pancreatic Disorders, continued … H. Fibrocystic Disease 1. Result of cystic fibrosis 2. Diagnosed by methods other than ultrasound Pancreatic Disorders, continued … I. Pancreaticolithiasis 1. Characteristic stone echoes in pancreatic duct 2. May see atrophied pancreatic parenchyma 3. Associated with chronic alcoholic pancreatitis 4. Contours of body, tail show irregularities Pancreatolithiasis, continued … 5. Incidence slightly higher in head 6. Associated with occult pancreatic carcinoma a. Mass < 2mm diameter b. Seen with dilation of pancreatic duct or CBD