NSG3MCC Nursing Care Plan modified 3
advertisement

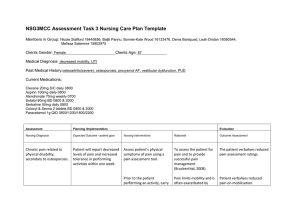
NSG3MCC Assessment Task 3 – Nursing Care Plan Group: Purple Group 1. Group Members: Nicole Stafford, 16445856 Baljit Pannu, Bonnie-Kate Wood, 16133476 Leah Dridan, 16080544 Melissa Salemme, 15802975 Group Facilitator: Anne Booms 1 Index Introduction .............................................................................................. 4 Diagnosis 1 - Chronic pain related to physical disability, secondary to osteoporosis. By Nicole Stafford 16445856 .............................................. 4 Diagnosis 2 - The patient may be experiencing some weakness due to a decrease in bone density secondary to osteoporosis. By Melissa Salemme 15802975 .................................................................. 6 Diagnosis 3 - Self-care deficit related to limited mobility due to severe OA. By Baljit Pannu .......................................................................... 8 Diagnosis 4 - Self-care deficit and inability to perform activities of daily living related to disease progression, weakness and joint deformity. By Bonnie-Kate Woods 16133476.............................................................. 9 Diagnosis 5 - Potential constipation during hospital stay due to Decreased Mobility and analgesic medications. By Leah Dridan 16080544 ......................................................................... 11 Conclusion - By Nicole Stafford 16445856 .............................................. 13 2 Bibliography ........................................................................................... 3 14 NSG3MCC Assessment Task 3 Nursing Care Plan. Members in Group: Nicole Stafford 16445856, Baljit Pannu , Bonnie-Kate Wood 16133476, Leah Dridan 16080544, Melissa Salemme 15802975. Clients Gender: Female Clients Age: 87 Medical Diagnosis: decreased mobility, UTI Past Medical History: osteoarthritis (severe), osteoporosis, proxysmol AF, vestibular dysfunction, PUD Current Medications: Clexane 20mg S/C daily 0800 Aspirin 100mg daily 0800 Alendronate 70mg weekly 0700 Sotalol 80mg BD 0800 & 2000 Sertraline 50mg daily 0800 Coloxyl & Senna 2 tablets BD 0800 & 2000 Paracetamol 1g QID 0800/1200/1800/2200 Assessment Planning /Implementation Evaluation Nursing Diagnosis Expected Outcome –patient goal Nursing Interventions Rationale Outcome Assessment 1. Chronic pain related to physical disability, secondary to osteoporosis. Patient will report decreased levels of pain and increased tolerance in performing activities within one week. Assess patient’s physical symptoms of pain using a pain assessment tool. To assess the patient for pain and to provide successful pain management (Bruckenthal, 2008). The patient verbalises reduced pain assessment ratings. 4 Prior to the patient performing an activity, carry out a pain assessment and treat the pain accordingly. Pain limits mobility and is often exacerbated by movement (Ackley & Ladwig, 2008) Patient verbalises reduced pain on mobilisation. Assess the patient’s cognitive functioning using a Mini Mental State Examination. To use appropriate pain assessment tool and to assess the extent of which the patient will be able to comply with the pain treatment regime (Scherder, Herr, Pickering, Gibson, Benedetti, & Lautenbacher, 2009). Patient suffers from depression and occasionally has short term memory issues; medications are prepared for her in a Webster pack to improve medication compliance. Educate patient on importance of taking medications and the relationship of the medications with her disease process. To empower patients and improve their knowledge with regard to their medications, which optimises the likelihood of patients to take their medications (Nurit, Bar Cohen, & Zelker Revital, 2009). The patient verbalises the importance of their medication regime and repeats back their understanding of the education session. Patient may need regular prompting to take medications due to short term memory issues. 5 2. The patient may be experiencing some weakness due to a decrease in bone density secondary to osteoporosis. The expected outcome will be that the patient will be more educated on how to manage osteoporosis as well as show an improvement in their bone density and strength before being discharged from the hospital. Assess the patient’s bone density by ordering a bone density scan in order to accurately assess the deterioration of the bones. Bone density scans are usually used to analyse the extent of the density of the bones in order to be able to plan treatment (Blake & Fogelman, 2007). These scans are also used to measure any improvement in bone density once interventions have been put in place (Blake & Fogelman, 2007). Continuous bone density scans in order to determine an improvement in bone density and strength. Refer the patient to a dietician who will organise an appropriate diet for an individual with osteoporosis. A diet high in calcium will help to prevent osteoporosis as well as slow down the progression of the disease in effected individuals and therefore increase their strength (Stransky & Rysava, 2009). Monitor the patient’s diet and make sure that they are well educated on the foods that are beneficial to bone strength. Administer calcium and vitamin D supplements. Administering calcium and vitamin D supplements in the treatment of osteoporosis will help to absorb the calcium in Make sure that the patient is taking their supplements. 6 their diet as well as prevent the occurrence of an osteoporotic fracture (Stransky & Rysava, 2009). Refer the patient to a physiotherapist in order to do simple strengthening exercises. Simple exercises such as walking or simple stretches can help to strengthen bones as well as prevent or slow down progression of osteoporosis (Keramat et. al, 2008). Allow the patient to demonstrate various simple exercises to promote bone strength. Educate the patient on osteoporosis by providing them with various brochures and information sessions in the community. Education is important for the patient to self care for their osteoporosis in the community setting (Nielsen et. al, 2010). It may be beneficial for the patient to join a community group who educate on osteoporosis, as it has been proven to be more successful in slowing down the progression of the condition through consolidating their education into practice and therefore producing stronger Let the patient tell you about osteoporosis and the treatments to prevent further progression and improve bone density. 7 bones (Nielsen et. al, 2010). Group sessions also increase the likelihood that the patient will adhere to their treatment plan (Nielsen et. al, 2010). 3. Self-care deficit related to limited mobility due to severe OA. Patient is able to show the level of functioning in the following activities such as bathing, dressing, feeding and toileting. Also patient demonstrates the ability to use assistive devices. Educate the patient about the variety of assistive devices used in home for bathing, dressing and toileting such as grip bars in shower, long handled zipper device, reacher, raised toilet seat or grip handle around toilet. To increase the patient’s sense of control over her life and to improve self-care ability (Carpenito, L. J., 2009). Monitor the patient’s activities and record them in charts. Schedule the activities in between to provide adequate rest periods. To decrease exhaustion as it decreases motivation for self-care activities (Brown & Edwards, 2009). Assess the patient’s selfcare activities and review the patient’s feelings whether she feels tired, restless or not. Refer to the occupational therapy for instructions in conserving energy techniques and use of assistive devices. Occupational therapy provides specific instructions and further assistance if required (Carpentio, L. J., 2009). Refer to the notes written by occupational therapist and assess the patient. Discuss with family members the changing family processes resulting Limited mobility associated with the chronic disease The family are adopting themselves with the chronic disease of the patient. 8 4. Self-care deficit and inability to perform activities of daily living related to disease progression, weakness and joint deformity. Achieve independence of self-care and maintain optimal role function. from the patient’s illness. interferes with the client’s ability to care for herself, her family and home which disrupts family functioning (Ralph, S. S. & Taylor, C. M., 2007). Discuss the importance of promoting client’s self-care at an appropriate level with the family. Maximum self-care activities promote positive self-esteem and reduces the feelings of powerlessness which leads to effective family functioning (Ralph, S. S. & Taylor, C. M., 2007). Ask the patient and family to verbally give response about coping with the present condition of the patient. Monitor patient’s ability to perform independent selfcare. Knowing what the patient is capable of enables us to plan appropriate interventions (Brown & Edwards, 2008). A reasonable goal is set based on the patient’s capabilities. Monitor patient’s needs for adaptive advices for personal hygiene, dressing, grooming, toileting and eating. Advices can compensate for contractures and weakness, so that the patient can perform as many self-care activities as possible, promoting All necessary advices are available to the patient if they are needed to achieve the goal of being independent and confident in performing her ADL’s. 9 independence (Ward & Loring, 2005). Establish a routine for selfcare activities with rest periods. Establishing a routine fosters maximum independence for the patient and rest periods allow minimal fatigue (Brown & Edwards, 2008). Assess the patients understanding of tasks to be completed and with a routine she will more than likely comply with the tasks. Modifications to home such as removing rugs, providing rails and elevated toilet seat. Modifications may be necessary to allow the patient to be as independent as possible without the risk of possible injury (DVA, 2011) Modifications help the patient to be safe and at the same time independent with activities of daily living. Teach family to encourage independence and to intervene only when the patient is unable to perform the task Teaching the family to only intervene when absolutely necessary is to allow the patient to understand they can do it and gives them independence in activites (Ward & Loring, 2005). With family encouragement the patient builds up a confidence that they can do specific tasks. Asking the family questions to see if they feel she has improved in confidence to perform tasks. 10 5. Potential constipation during hospital stay due to decreased mobility and analgesic medications. Patient will maintain regular to substantial bowel motions during her hospital stay. Observe and monitor usual defecation patterns, including amount, frequency and stool consistency. Compare this to regular bowel motions of patient prior to hospital stay and during hospital stay. This allows a baseline that enables nursing and medical staff to compare if patient becomes distended and impacted (Gulanick & Myers, 2007). Monitor the chart to recognise any changes in bowel actions. Encourage mobility and ADL’s. Ensure these are undertaken post pain medication administration for patient comfort. Mobilising and being active increases peristalsis of the bowels enabling bowel motions and decreasing the chances of constipation (Gulanick & Myers, 2007). Reassess mobility levels daily and determine which method of mobilising is most comfortable for the patient. (Gulanick & Myers, 2007). If patient is in too much pain for weight bearing, encourage movements on the bed, including twisting and changing positions while in bed, lifting her left leg up and down slowly, pulling her left knee to her hip and slowly straightening her leg. Other exercises can include lifting her upper torso slightly whilst flexing her abdominal muscles. The patient is more likely to be apprehensive of mobilising when there is strong pain involved on movement. Despite pain medications contributing to decreased elimination, the patient is best to mobilise out of bed when medications are administered, than nil movement after 11 (Gulanick & Myers, 2007). Encourage fluid intake, 6-8 Adequate fluid intake is glasses per day necessary to prevent hard and dry stools that are difficult to pass (Eoff & Lembo, 2008). Use a fluid balance chart to monitor fluid intake and output. Encourage oral intake, a diet high in fibre. When fibre reaches the colon, it absorbs water forming a gel and adding bulk to faeces, enabling full stools that are easy to pass (Eoff & Lembo, 2008). Use a food chart to monitor nutritional intake. Educate the patient on how and why the constipations have occurred, as well as interventions they can initiate to prevent it Education will allow the patient to understand constipation better; hence enabling them to self-initiate and manage their own care (Eoff & Lembo, 2008). Assess the patients understanding of constipation and have them talk the steps into preventing constipation. Provide laxatives, suppositories, and enemas ordered or when required. These soften stool, lubricate intestinal mucosa and help peristalsis (Gulanick & Myers, 2007). Assess patient’s bowel chart and ask patient about their bowel motions, any discomfort or pain that is present. From this information, determine if medication will be needed. (Eoff & Lembo, 2008). 12 Conclusion In caring for our patient with her diagnosed chronic conditions we individually came up with nursing diagnoses that we believed would affect her daily life. We believed her main issues would relate to pain, weakness, self-care deficit, potential risk for constipation due to immobility and analgesic medications. Most of our interventions were based around education and how we could support our patient to live an improved quality of life. In developing nursing interventions we looked at diet, assessments, involving the patient’s family and referral to other health services within the multidisciplinary team. We were focusing our care around a patient centred approach to ensure; that we involved the patient and their significant others in the development of her care plan. As this will encourage the patient’s compliance, independence and will hopefully give our patient family support, as they were too involved in the care plan process. 13 Bibliography Ackley, B. J., & Ladwig, G. B. (2008). Nursing diagnosis handbook: an evidenced-based guide to planning care. St Louis: Mosby Elsevier. Blake, G. M., & Fogelman, I. (2007). The role of DXA bone density scans in the diagnosis and treatment of osteoporosis. Postgraduate Medical Journal, 83(982), 509-517. Brown, D., & Edwards, H. (2008). Lewis's medical-surgical nursing: assessment and management of clinical problems (2nd ed.). St Louis: Mosby Elsevier. Bruckenthal, P. (2008). Assessment of Pain in the Elderly Adult. Clinics in Geriatric Medicine, 24(2), 213-236. Carpenito-Moyet, L. J. (2009). Nursing care plans and documentation: nursing diagnosis and collaborative problems (5th ed.). Philadelphia: Lippincott Williams & Wilkins. Department of Veteran Affairs. (2011, August 16). Homecare and Support: Community Aged Care. Retrieved September 15, 2011, from Department of Veteran Affairs: http://www.dva.gov.au/benefitsAndServices/health/homecare Eoff, J. C., & Lembo, A. J. (2008). Optimal treatment of chronic constipation in managed care: Review and roundtable discussion. Journal of managed care pharmacy, 14(9), S5-S9. Gulanick, M., & Myers, J. (2007). Nursing care plans: Nursing diagnosis and intervention (6th ed.). St Louis, Missouri: Mosby Elsevier. Keramat, A., Patwardhan, B., Larijani, B., Chopra, A., Mithal, A., & Chakravarty, D. (2008). The assessment of osteoporosis risk factors in Iranian women compared to Indian women. BMC Musculoskeletal Disorders, 9(28). Nielsen, D., Ryg, J., Nielsen, W., Knold, B., Nissen, N., & Brixen, K. (2010). Patient education in groups increases knowledge of osteoporosis and adherence to treatment: A two-year randomized controlled trial. Patient Education and Counselling, 81(2), 155-160. Nurit, P., Bar Cohen, B., & Zelker Revital, G. (2009). Evaluation of a nursing intervention project to promote patient medication education. Journal of Clinical Nursing, 18(17), 2530-2536. Ralph, S. S., & Taylor, C. M. (2007). Nursing diagnosis reference manual (7th ed.). Philadelphia: Lippincott Williams & Wilkins. 14 Scherder, E., Herr, K., Pickering, G., Gibson, S., Benedetti, F., & Lautenbacher, S. (2009). Pain in dementia. Pain, 145(3), 276-278. Stansky, M., & Rysava, L. (2009). Nutrition as prevention and treatment of osteoporosis. Psychological Research, 58(1), S7-S11. Ward, M., & Loring, K. (2005). Patient education interventions in osteoarthritis and rheumatoid arthritis: a meta-analytic comparison with Non-steroidal anti inflammatory treatment. 9(4), 292-301. 15