EUS and acute Pancreatitis

EUS and Acute Pancreatitis
Robert Kavitt
March 16, 2011
Definition of IAP (Idiopathic acute pancreatitis)
Imaging modalities in IAP
Review of literature regarding use of EUS in IAP
EUS and gallstone pancreatitis
EUS images
EUS and autoimmune pancreatitis
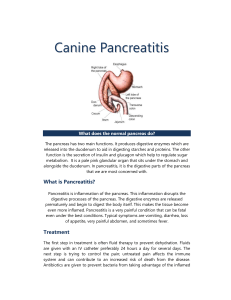
EUS of a Normal Pancreas
BP: Body of pancreas
PD: Pancreatic duct
SV: Splenic vein
Defining
Idiopathic Acute
Pancreatitis (IAP)
Idiopathic Acute Pancreatitis
Cause of acute pancreatitis unidentified in >10%, after abd u/s, CT, and labs
Patients often undergo ERCP, especially when they have recurrent bouts of pancreatitis
ERCP establishes etiology in 30-60% of these patients
Predominant findings include biliary calculi, chronic pancreatitis, pancreatic tumors, and SOD dysfunction
EUS should also be useful as it can diagnose missed biliary tract disease, chronic pancreatitis, and small pancreatic tumors
EUS carries less risk than ERCP
Idiopathic Acute Pancreatitis
In many cases the possibility of finding a cause of the pancreatitis depends directly on how deep the etiological search is made
Can find gallbladder microlithiasis, SOD dysfunction, pancreas divisum, chronic pancreatitis, pancreatic tumors or cysts, long pancreatiobiliary junction, annular pancreas, choledococele, duodenal duplication cyst, or periampullary diverticulum as cause of acute pancreatitis
In patients under 40 without mechanical or anatomic causes, check gene mutations (mutations of cationic trypsinogen gene, serine protease inhibitor Kazal type 1, or mutation in CFTR)
If not corrected, up to 70% of acute pancreatitis episodes may recur, depending on the cause
Mortality rate 4-9% for acute pancreatitis
Imaging Modalities in Idiopathic Acute
Pancreatitis
ERCP
Has been the 1 st choice of diagnostic procedures in patients with IAP for the past 3 decades
10-15% rate of potentially severe complications
Able to perform therapeutic maneuvers necessary in up to 75% of these patients
Some authors advise ERCP only after 2 nd episode of IAP or after the 1 st episode if severe
Others support systematic use of ERCP after 1 st IAP episode
MBE (Microscopic Bile Examination)
Microlithiasis present in up to 80% of IAP patients with gallbladders
MBE sensitivity 65-90%, specificity 88-100% in diagnosis of microlithiasis
MBE is falsely negative in 29-50% of patients with known gallbladder lithiasis
Not feasible in up to 20% of patients (due to inability to place nasoduodenal probe in 2 nd portion of dudodenum, aspiration of inadequate material, or patient intolerance)
MRCP
May diagnose chronic pancreatitis, SOD dysfunction, anatomic anomalies, and choledocholithiasis
May be useful, especially when combined with secretin test, showing a PPV for diagnosis of SOD dysfunction of
100% (NPV 64%)
EUS vs. MRCP
49 patients with dx of idiopathic acute pancreatitis, evaluated prospectively with EUS and MRCP, then diagnoses compared between the 2 modalities
In 28 patients (57%), EUS and/or ERCP diagnosed at least 1 possible cause
Diagnostic yield of EUS higher than MRCP (51% vs. 20%, p=0.001)
Cholelithiasis and biliary sludge (24%) most frequent EUS dx
Pancreas divisum (8%) most frequent MRCP dx
Only in 3 cases (6%) did MRCP identify additional features in patients etiologically undiagnosed using EUS
EUS yield lower in patients with prior cholecystectomy
(11% vs. 60%, p=0.008)
EUS
Diagnostic accuracy of 60-80% in patients with IAP
Offers ability to FNA and analyze cyst fluid for tumor antigens, fluid viscosity, mucin staining, amylase concentration, analysis of genetic mutations associated with tumors, and cytology
GIE 2009 (Artifon et al): Report of performing sphincterotomy on EUS
If microlithiasis is diagnosed, a cholecystectomy reduces the recurrence of pancreatitis from 66-75% in untreated patients to 10% in patients who undergo cholecystectomy
EUS in Idiopathic Acute Pancreatitis
Aim to determine utility of EUS in patients with idiopathic acute pancreatitis and whether subsequent
ERCP is needed
Review of prospectively collected database, with follow-up telephone interviews
EUS diagnosis compared with final diagnosis and outcome
EUS in Idiopathic Acute Pancreatitis
• EUS revealed etiology of pancreatitis in
21/31
• Microlithiasis in 5
• Chronic pancreatitis in 14
• Pancreas divisum in 2
• Pancreatic cancer in 1
• Not diagnostic in 10 (32%)
EUS in Idiopathic Acute Pancreatitis
Mean follow-up period of 16 months; Dx changed in 4; 9 had ERCP because of persistent symptoms or recurrent pancreatitis
Conclusion: EUS determined etiology in two-thirds, and most did not require ERCP during follow-up period. EUS can be alternative to ERCP in patients with unexplained acute pancreatitis.
Disadvantages of EUS as Initial
Endoscopic Test
This approach delayed diagnosis in 4 patients, whose diagnoses of pancreatic duct stone, SOD dysfunction, pancreas divisum, and IPMN were not made sonographically
In each of these cases, ERCP was performed because of recurrent symptoms, and demonstrated the correct diagnosis
J Pancreas, March 2009
Retrospective analysis of all biliary EUS studies from
2000-2004
42 patients with negative prior radiological investigations
EUS normal in 17, noted signs of recent acute pancreatitis but not other etiology in 8, noted cholelithiasis or microlithiasis in 9, combined gallstones/microlithiasis and choledocholithiasis in 6
1 patient had calculi in CBD but not the gallbladder
1 patient had signs of chronic pancreatitis
J Pancreas, March 2009
All patients with CBD stones underwent ERCP and sphincterotomy, and stones were confirmed in all
EUS provided additional diagnostic info in 17/42 (40.5%)
Most cases of cholelithiasis can be diagnosed with standard imaging modalities but when these fail to identify a cause, EUS has an important role to play.
J Pancreas, March 2009
Stone pathology identified in 16/42 patients in whom other imaging modalities failed to identify lithiasis
EUS has a reported sensitivity of up to 100% and specificity as high as 95.4%, with a negative predictive value as high as 100% for detection of CBD stones wich are the cause of acute biliary pancreatitis
EUS especially beneficial for detecting stones smaller than 5 mm
Then why not EUS everyone?
“Given the superiority of EUS over other imaging modalities, it may be argued that EUS be used in the investigation of all cases of acute pancreatitis in which no calculi are observed in either the gallbladder or CBD on trans-abdominal US…
However, given the limited availability of EUS and pressures on skilled operators to perform non-biliary investigations, we would suggest that all patients with acute pancreatitis undergo a trans-abdominal US and also have routine biochemical investigations to look for hypercalcaemia and hyperlipidaemia…
A careful drug history is important in particular in relation to statins as these drugs are now widely prescribed as lipid lowering agents, and are associated with acute pancreatitis.
We then perform an MRCP as our next investigation of choice, with EUS limited to those in which no cause for acute pancreatitis has been identified. In the future, as EUS proliferates, it may then become the investigation of choice.”
EUS and
Gallstone
Pancreatitis
Gallstone Pancreatitis
Liu et al GIE 2001: “Detection of choledocholithiasis by EUS in acute pancreatitis: a prospective evaluation in 100 consecutive patients”
Study of 100 consecutive patients with acute pancreatitis who underwent transabdominal u/s, EUS, and ERCP
EUS was more sensitive than transabdominal u/s for detecting gallbladder stones (100% vs. 84%)
Sensitivities of ERCP and EUS for choledocholithiasis were both
97%
EUS correctly identified the absence of choledocholithiasis in
65 of 66 patients (specificity 98%)
Gallstone Pancreatitis
EUS may have a role in reducing uncertainty about whether there is a retained CBD stone in patients with gallstone pancreatitis.
EUS may help clarify the diagnosis in those with apparent idiopathic pancreatitis or abdominal pain in whom a biliary source cannot be firmly excluded.
EUS Images
Choledocholithiasis
Gallstone in Gallbladder
CBD Stones
Elongated stone in CBD
ERCP showing stone in CBD
Stone being removed from CBD with basket after sphincterotomy
EUS and
Autoimmune
Pancreatitis
Autoimmune Pancreatitis
Enlargement of pancreatic gland, diffuse narrowing of
Wirsung duct with an irregular wall
Elevated IgG4
Marked lymphoplasmacytic infiltration and dense fibrosis
IgG4 (cutoff 135 mg/dl)
Sensitivity 95%, Specificity 97%, for distinguishing autoimmune pancreatitis from pancreatic cancer
Type I: W. Europe and U.S. (IgG4 negative)
Type II: Asia
Autoimmune Pancreatitis
Farrell et al, GIE 2004: “EUS findings in patients with autoimmune pancreatitis”
Features of autoimmune pancreatitis on EUS are easily mistaken for malignancy
Diffusely hypoechoic, enlarged pancreas, together with chronic inflammatory cells in aspirated cytologic specimens, is supportive of the diagnosis of autoimmune pancreatitis
When combined with clinical data, EUS and EUS-guided FNA may support this diagnosis, may warrant a trial of steroids, and may prevent unnecessary surgery
Timing: When to EUS?
Reports range from when patients resume food intake, to when acute pancreatitis bout has resolved during admission, to 2-3 weeks after acute phase, to at least 4 weeks after acute episode (in order to ensure that parenchymal changes have resolved)
Likely should wait at least 4 weeks, to avoid misdiagnosis and to differentiate gallbladder microlithiasis related to acute pancreatitis fasting from previously present microlithiasis
But: Delay in EUS has potential risk of losing patient for f/u once asymptomatic, and a small pancreatic tumor could be missed