1st and 2nd Lectures

PHL 616
Drug Discovery & Development
First and second lectures
By
Abdelkader Ashour, Ph.D.
Phone: 4677212 Email: aeashour@ksu.edu.sa
Drug Discovery & Development,
Overview
A drug target can be a receptor/ion channel, enzyme, hormone/factor, DNA, RNA, nuclear receptor, or other, unidentified, biological entity
Once drug targets are identified, they are exposed to a large number of compounds in an in vitro or cell-based assay
Compounds that elicit a positive response in a particular assay are called “hits.” Hits that continue to show positive response in more complex models rise to “leads” (lead identification)
A selected few of the optimized leads (candidate drugs) are then advanced to preclinical testing and clinical testing and therefore passed along to the product development staff
Drug Discovery,
Definitions
Drug
“A chemical substance of known structure, other than a nutrient or an essential dietary ingredient, which, when administered to a living organism, produces a biological effect”
Drugs may be synthetic chemicals, chemicals obtained from plants, microorganisms or animals, or products of genetic engineering
Medicine
“A chemical preparation, which usually contains one or more drugs, administered with the intention of producing a therapeutic effect”
Medicines usually contain other substances (excipients, stabilisers, solvents, etc.) besides the active drug, to make them more convenient to use
To count as a drug, the substance must be administered as such, rather than released by physiological mechanisms
Many substances, such as insulin or thyroxine, are endogenous hormones but are also drugs when they are administered intentionally
Many drugs are not used in medicines but are nevertheless useful research tools
The word drug is often associated with addictive, narcotic substances-an unfortunate negative implication that tends to bias opinion against any form of chemical therapy
Drug Discovery,
Definitions
Effects (therapeutic effects)
“The desired results of administration of a medication”
Side Effects (adverse effects)
“Effects that are harmful and undesired, and that occur in addition to the desired therapeutic effects”
Indications
“The reasons for administering a medication or performing a treatment”
Contra-indications
“Factors that prevent the use of a medication or treatment (e.g., allergies)”
Drug Nomenclature
Chemical name represents the exact description of the drug’s chemical composition
Generic name (non-proprietary)
simpler than the chemical name and
derived from the chemical name itself
easier to remember
Example 1: the chemical name 2-methyl-5-nitroimidazole-l-ethanol is condensed to the generic name metronidazole . The word methylnitro is condensed to metroni and dazole is due to its imidazole ring
Example 2: Metoclopramide is the condensed form of the word methoxychloroprocainamide: where Me is retained and th is written as t ; chloro is written as clo : and procainamide is written as pramide
Brand or trade name (proprietary) is developed by the company requesting approval for the drug and identifies it as the exclusive property of that company.
Example 1: Metrogyl ® is the trade name for metronidazole .
Example 2: Reglan
® is the trade name for metoclopramide .
Example 3: Amoxil
® is the trade name for amoxycillin .
Example 4: Celebrex
® is the trade name for celecoxib .
Drug-Body Interactions
Pharmacokinetics
Pharmacokinetics (in Greek: "pharmacon" meaning drug, and
"kinetikos" meaning putting in motion)
The study of the movement of drugs in the body, including the processes of absorption, distribution, localization in tissues, biotransformation and excretion
Pharmacodynamics
The study of the action or effects of drugs on living organisms
Pharmacokinetics vs Pharmacodynamics
What the body does to the drug What the drug does to the body
Drug Sources
Many therapeutic agents originate from natural products
Until about 1950, when synthetic chemistry really came into its own as a source of new drugs, most of the pharmacopoeia consisted of natural products, and they continue to be important drug source, e.g. paclitaxel
Such ready-made, highly evolved biomolecules are supposed to have a better chance of interacting with selected drug targets than do random synthetic molecules
Exploiting such compound library is seen as an attractive strategy which has led to some important therapeutic breakthroughs, such as:
The anti-malarial drug artemesinin
Immunosuppressants such as tacrolimus
[fujimycin or (FK506)]
Paclitaxel and other recently introduced anticancer drugs
Many therapeutic agents originate from natural products
In practice, the theoretical advantages of natural products are balanced by several practical disadvantages:
Access to source material in remote places can be troublesome for geographical reasons
The continuing availability of the active compound, if it cannot be synthesized on a commercial basis, may be uncertain
Purification and structure determination of natural products is often difficult and timeconsuming
Many antibiotics originate from microorganisms
Fosfomycin is produced by several Streptomyces species
Cycloserine is an antibiotic produced by Streptomyces orchidaceous
Bacitracin is a polypeptide antibiotic produced by strains of Bacillus subtilis and
Bacillus licheniformis
Vancomycin is an antibiotic produced by Streptococcus orientalis
Benzylpenicillin (penicillin G) is produced by Penicillium chrysogenum
Cephalosporins were first obtained from a filamentous fungus “ Cephalosporium”
The intrinsic antimicrobial activity of natural cephalosporins is low, but the attachment of various groups has yielded drugs of good therapeutic activity and low toxicity
Imipenem was discovered in 1980 via a lengthy trial-and-error search for a more stable version of the natural product thienamycin, which is produced by the bacterium Streptomyces cattleya . Thienamycin has antibacterial activity, but is unstable in aqueous solution, so impractical to administer to patients
MOA of inhibitors of cell wall synthesis
Creation of a new drug
The creation of a new drug can be divided into three main phases:
I.
Drug discovery: from therapeutic concept to molecule
II. Drug development: from molecule to registered product
III. Commercialization: from product to therapeutic application to sales
Drug Discovery & Development,
Overview
A drug target can be a receptor/ion channel, enzyme, hormone/factor, DNA, RNA, nuclear receptor, or other, unidentified, biological entity
Once drug targets are identified, they are exposed to a large number of compounds in an in vitro or cell-based assay
Compounds that elicit a positive response in a particular assay are called “hits.” Hits that continue to show positive response in more complex models rise to “leads” (lead identification)
A selected few of the optimized leads (candidate drugs) are then advanced to preclinical testing and clinical testing and therefore passed along to the product development staff
Creation of a new drug
Before the start of any new project, the creation plan is judged by the following criteria:
1.
The drug’s scientific strength and originality
2. Development and marketing issues. For example: i.
If the therapeutic target is an ill-defined clinical disorder, e.g., chronic fatigue syndrome, will it be possible to measure clinical efficacy objectively? ii.
Does the project face stiff competition from other companies working in the same area, or from drugs already in clinical use? iii. Is it likely that an esoteric drug delivery system will be required, and if so, can this be developed? iv. If the drug is successfully developed, is the expected market sufficient to justify the cost of development?
It is essential to keep such issues constantly under review, and to adapt the project plan if necessary
Creation of a new drug, contd.
As recently as 25 –30 years ago in most companies, drug creation was much more compartmentalized:
Scientists produced molecules with interesting pharmacological properties
Development functions were responsible for checking their safety and turning them into registrable drugs
The marketing department generated sales and turned them into revenues
At the time, this worked well, and many companies prospered
The drop-out rate was not excessive, because regulatory requirements were less stringent
The failures rate was not unduly expensive in terms of time and resources lost
Creation of a new drug, contd.
In the last two decades, biomedical science has advanced dramatically:
Drug discovery and development have become more technology-driven and, hence, expensive
Regulatory requirements became much more stringent
The competition is more intense
With bigger teams, and more complex multidisciplinary tasks, effective project management has become much more important than it used to be to keep costs and delays to a minimum
The increased amount of work being done in partnership with other companies or with academic groups, adding the need for alliance as well as project management
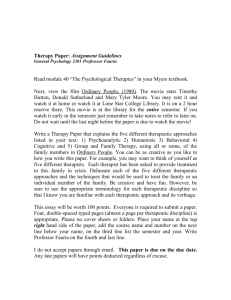
Drug discovery phase of a typical project aimed at producing a new synthetic drug
Drug discovery starts with the choice of a disease area and defining the therapeutic need that is to be met
It then proceeds to the identification of the biochemical, cellular or pathophysiological mechanism that will be targeted, and, if possible, the identification & validation of a molecular ‘drug target’
The next step is the identification of a lead structure
This is followed by the design, testing and fine-tuning of the drug molecule to the point ‘Drug candidate’ where it is deemed suitable for development