Six Sigma for Performance Improvement
advertisement

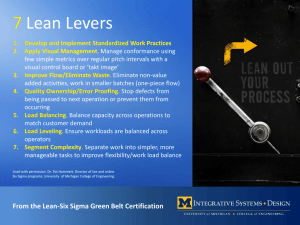
Six Sigma for Performance Improvement Duke University Hospital THEF November 29, 2007 Why Six Sigma? • • Six Sigma is a disciplined, datadriven approach to process improvement aimed at the nearelimination of defects from every product, process, and transaction. The purpose of Six Sigma is to gain breakthrough knowledge on how to improve processes to do things BETTER, FASTER, and at LOWER COST. Six Sigma can be used for any activity that is concerned with cost, timeliness, and quality of results. Years 2 What is the Six Sigma Methodology? • Six Sigma is based on . . . – Statistical process control techniques – Data analysis methods – Systematic training of all personnel involved in the activity or process targeted by the program • The Six Sigma goal is to . . . – Eliminate defects, waste and/or quality problems – Improve bottom-line results, and customer satisfaction • Six Sigma can be applied to . . . – – – – Manufacturing Sales and customer service Management Any process 3 Six Sigma Focal Points • • • • Focus on the customer Focus on teamwork Focus on reducing variation Focus on results 4 Focus on Customers CTQ’s (Critical To Quality) 5 Focus on Teamwork • Leads Team • Partners with Process Owner • Part Time • Works Projects Black Belt • Breaks Down Barriers • Owns Project Cluster Project Champion Process Owners • Manages Day to Day Operations • Controls Resources Green Belt Team Members • 3-5 Process/Product Experts 6 Focus on Reducing Variation • Highly variable processes result in a high number of defects • If an ADE is a defect and DUH administers 5 meds to each patient per day on average, at: – 2 Sigma – 1,001 ADE’s would occur each day (69.2% good) – 3 Sigma – 217 ADE’s would occur each day (93.3%) – 4 Sigma – 20 ADE’s would occur each day (99.4%) – 5 Sigma – 3 ADE’s would occur every 4 days (99.98%) – 6 Sigma – 1 ADE would occur every 3 months (99.9997%) 7 Hand Tools • Brainstorming • Cause-and-effect Diagrams • Graphs and Charts – – – – – – Box Plot Dot Plot Histogram Pareto Chart Run Chart Scatter Plot • Process Flow Diagrams • Statistical Process Control • Stratification 8 Power Tools • • • • Value Stream Analysis Analysis of Variance (ANOVA) Correlation & Regression Design Of Experiments – Full Factorial Designs – Fractional Factorial Designs – 2k Designs • • • • • FMEA Hypothesis Testing Measurement System Analysis Process Capability Studies Response Surface Methods 9 Focus on Results Y = f(X) 10 Focus on Results Patient Safety Cost Avoidance Cost Savings Revenue Generation Quality Care Public Confidence Include hidden cost 11 Technical Definition of a Six Sigma Process Off-Target A Six Sigma Process LSL USL 6σ Too Much Variation 6σ Process is centered around the target with 6 standard deviations between the mean and upper and lower specification limits. 12 What does a Six Sigma Program look like? Structure • Leadership • Direction • Resources Strategic Alignment Tools • Business Objectives • Customer Requirements • • • • DMAIC FMEA Workout LEAN 13 The Tools of Six Sigma • Analysis Tools – The Scientific Method (DMAIC) – LEAN • Improvement Tools – Mistake-Proofing – Design of Experiments – FMEA • Process Monitoring Tools – Audits – Control Charts • Facilitation and Project Management Tools – Workout and Kaizen – Brainstorming 14 DMAIC – Scientific Method Define Project goals and boundaries are set, and issues are identified that must be addressed to achieve an improved quality level (i.e., defect rate). Measure Information about the current situation is gathered in order to obtain baseline data on current process performance and identify problem areas. Analyze Root causes of quality problems are identified and confirmed with appropriate data analysis tools. Improve Solutions are implemented to address the root causes of problems identified during the analyze phase. Control Improvements are evaluated and monitored. 15 What does a Six Sigma Program look like? Structure • Leadership • Direction • Resources Strategic Alignment Tools • Business Objectives • Customer Requirements • • • • DMAIC FMEA Workout LEAN 16 Sources for Nominating Projects • • • • • • Balanced Scorecards Patient complaints, responses to surveys Regulatory Issues Benchmarking shortfalls Critical items in financial reports Strategic business plans 17 Alignment DUH Priority Be a top performing hospital for publicly reported data CSU Measure CMS Evidence-Based Care Score Improvement Opportunity Adherence to AMI Process Measures Research supports that measure adherence drives outcome. Six Sigma Project Improve Time to PCI Outcome 1. Improve median PCI time to 54 min 2. Leadership of State-Wide RACE Project 3. Research Studies 4. Process Recommendations to ACC 18 What does a Six Sigma Program look like? Structure • Leadership • Direction • Resources Strategic Alignment Tools • Business Objectives • Customer Requirements • • • • DMAIC FMEA Workout LEAN 19 The Structure of a Six Sigma Program • Executive/Owner Involvement – Top-level support is the most important factor leading to success – Organizational leaders must • Set the vision for success • Create an environment demanding of improvement • Review all projects and expect results • Resource Allocation – Utilize your best employees – Make time for them to do the work 20 The Structure of a Six Sigma Program • Structured project review process – Review projects regularly – Develop clear guidelines for success and completion • Training – Ensure all involved employees understand their roles in the improvement process – Invest in advanced training for project leaders 21 Resource Model • 45 trained black belts; 123 trained green belts • Centrally placed – – – – Organize and execute the deployment plan Lead organizational projects Support operationally placed black belts Located in Performance Services • Operationally placed – Aligned with Clinical Service Units (CSU) and targeted Departments – Primary reporting relationship with the departmental / CSU leadership 22 Six Sigma Oversight Committee • Accountable to DUH Executive Committee • Oversight of projects and organizational project selection • Structured review format – Approval of projects – Tollgate reviews • Oversight members – COO, CFO, CNO, Director of HR, Director of Accreditation/Clinical Quality/PSO, Senior AOO 23 Six Sigma Black Belt Council • Coordinate and collaborate as a collection of key subject matter experts to review analysis and provide input for other black belt projects • Provide input to Six Sigma Oversight Committee regarding potential black belt projects • Review and recommend improvements to the Six Sigma training programs 24 Project Example Orthopedic Patient Satisfaction CTQs What is “Critical to Quality” (CTQ)? – Patient Outcome – Patient Safety – Positive Experience • • • • • • Appropriate Response to Concerns Inclusion in Decisions about Treatment Address Emotional Needs Sensitive to Inconvenience Attention to Personal Needs Information and Communication 26 Problem and Mission Statements Problem Statement The FY05 average overall patient satisfaction mean score for Duke University Hospital Orthopedics Specialty was a .6 deviation from the target. Orthopedics Specialty ranks in the 65th percentile compared to COTH hospitals. Mission Statement Improve overall mean satisfaction score to 84.1, increasing the specialty ranking to approximately the 74th percentile compared to COTH and orthopedic specialty hospitals, for discharges starting April 2006. Rank based on Jul 04 – March 05 27 Initial Performance Overall Mean Score 90 89 88 87 86 85 84 83 82 81 80 79 78 77 76 75 85.3 84.9 83.1 83.5 82.8 82.5 81.4 80.8 81 78.9 78.7 76.5 2005-07 2005-08 2005-09 2005-10 2005-11 2005-12 2006-01 2006-02 2006-03 2006-04 2006-05 2006-06 Actual Target Linear (Actual) 28 Measure/Control Hospital Level IP Overall Mean Score SAS Scorecard CSU Level SAS Scorecard Unit Level 6100 Overall Mean Score 6100 Overall Mean Score Nursing BSC Unit Level 6100 Mean Score by Unit and Question Press Ganey Report Detail Patient Surveys and Comments Press Ganey 29 Potential Factors Y=f (x1)+f(x2)+f(x3)+f(x4)+f(Xu) X1 = Age X2 = Gender X3 = Procedure X4 = Race X5 = Timeframe X6 = Discharge Disposition X7 = Procedure X8 = PG Question Process Inpatient Mean Score X8a = Task X9 = Pre-op Education X10 = Staffing X11 = Turnover 30 Productivity Correlation 87.5 Summary of Fit 85 RSquare RSquare Adj Root Mean Square Error Mean of Response Observations (or Sum Wgts) sat 82.5 80 0.227417 0.150159 2.413577 82.32117 12 Analysis of Variance Source Model Error C. Total 77.5 75 75 80 85 90 DF Sum of Squares Mean Square 1 17.147515 17.1475 10 58.253522 5.8254 11 75.401037 95 F Ratio 2.9436 Prob > F 0.1170 prod Satisfaction Increases as Efficiency Increases No correlation between Census and Satisfaction 31 Work-OutTM February 23, 2006 • • • • • • Response to concerns and complaints Include in decisions re: treatment Staff addresses emotional needs Staff sensitivity to inconvenience Nurses kept you informed Attention to special/personal needs A B Staff Chose Option A: More concrete concept, staff able to control, easier to create processes to improve 32 Implementation of Action Items • Communicate with Patient About their Care – – – – Develop process for shift goal ID during assessment (Vanita) Develop call light process (Lisa H & Lisa W) Develop scripting messages (Lisa H) Develop & implement training for basic rehab skills (Jennie & Kathy) – Display mobility on white boards (Kathy) • Communication Between Staff – Communicating assignment in report process (Vanita) – Implement process for posting PRM & PT assignments (Joyce & Kathy) – Identify patients that will be seen early by PT/OT (Kathy) – Develop infrastructure for complaint resolution (Carey) – Communicate recommendations from team related to report process (Vanita) 33 Implementation of Action Items • Expectation Setting for the Inpatient Experience – Create “Welcome to 6100” document (Shane) – Communicate with MDs about classes (Carey & Jennie) – Implement incentive for class (Jennie) • Training/Behaviors for Staff – Communicate performance expectations as outlined in PPS (Linda) – Develop schedule and plan for training (Joyce, Alene, Linda & Shane) • Culture of the Unit – Develop structure and avenue to implement peer feedback (Monica) – Posting Press Ganey Scores and Comments (Carey) – Ensure peer support for breaks (Monica) – Develop award system for staff (Alicia) 34 Control Process • Measure Reviews by Nurse Manager/Clinical Operations Director – Overall Score monthly – Question review monthly – Good/Very Good review monthly • Reaction Point – 2 points below target requires follow-up at Musculoskeletal CSU Executive Meeting • Rounding/Leadership Follow-Up • Staff awareness through storyboards • Pay and performance Link at Management and Staff Level 35 Performance Summary Overall Mean 90 89 87.9 88 87 86 Implementation of Action Items 85.4 86 85.3 84.9 85 Project Start 83.5 85.6 85.2 84.8 Work-Out 83.1 84 83.3 83 82.8 82.7 82.5 82 83.1 81.4 81 80.8 81 81 83.4 82.8 82.7 81.3 80 79 78.9 78.7 78 77 76.5 76 75 Jan-05 Feb-05 Mar-05 Apr-05 May-05 Jun-05 Jul-06 Aug-06 Sep-06 Oct-06 Nov-06 Dec-06 Jan-06 Feb-06 Mar-06 Apr-06 May-06 Jun-06 Jul-07 Aug-07 Sep-07 Oct-07 Nov-07 Dec-07 Jan-07 Feb-07 Actual Target Linear (Actual) 36 Performance Summary Percentile Ranking 37 Questions?