Sarandeep Singh Puri. “Benign Giant Cell Tumor of Tendon Sheath

CASE REPORT
BENIGN GIANT CELL TUMOR OF TENDON SHEATH: BENIGN SYNOVIOMA -
A RARE CYTOMORPHOLOGY IN PRACTICE
Sarandeep Singh Puri 1
HOW TO CITE THIS ARTICLE:
Sarandeep Singh Puri. “Benign Giant Cell Tumor of Tendon Sheath: Benign Synovioma - A Rare
Cytomorphology in practice”. Journal of Evolution of Medical and Dental Sciences 2013; Vol. 2, Issue 52,
December 30; Page: 10284-10288.
ABSTRACT: Giant Cell Tumor of Tendon Sheath is a benign soft tissue tumor, common on the flexor surface of the hand, where tenosynovial tissue predominate. It slowly enlarges, has the potential to envelop tendons, invade bones and joints and to surround neurovascular structures. We present a case of 47 year female patient with a single swelling over the course of tendon of the Right Index
Finger-Distal Phalanx. Radiograph revealed an eccentric, well defined, soft tissue radio-opacity noted at the lateral aspect of the Distal Interphalangeal Joint of the Index Finger. Fine Needle
Aspiration Cytology (FNAC) of the swelling on the Right Index Finger- Distal Phalanx showed plenty of multinucleated giant cells and exclusion of the other Giant cell containing lesions confirmed the
Cytodiagnosis of Benign Giant Cell Tumor of Tendon Sheath: Benign Synovioma. Subsequent
Histopathological evaluation supported the cytodiagnosis. Rarity of these lesions to be diagnosed at
FNAC, makes it a case of presentation, as its preoperative Cytodiagnosis by FNAC is rarely reported in the literature.
KEYWORDS: Giant Cell Tumor of Tendon Sheath, Fine Needle Aspiration Cytology, Multinucleated
Giant cells.
INTRODUCTION: A giant cell tumor of tendon sheath is a soft tissue tumor consisting principally of a proliferation of synovial cells arising from a tendon sheath. Only 2% of all giant cell tumors occur in the hand. Only 1% to 2% may be synchronously or metachronously multicentric. Giant cell tumour of the tendon sheath, fibrous histocytoma of synovium, pigmented nodular synovitis, tenosynovial giant cell tumour, localised nodular tenosynovitis, benign synovioma, and fibrous xanthoma of the synovium are all names for the same disease .(1, 2, 3, 4)
CASE REPORT:
Clinical Presentation- A 47 year old female presented with Swelling over the course of tendon of the Right Index Finger Distal Phalanx since two years, increased from 0.5cm to present size of 1.5 cm. Previously took medical advice for the lesion, which were inconclusive in nature. Hematological evaluation was normal. On physical examination, the swelling was firm, nodular, non tender, circumscribed, with smooth lobulated contours, overlying skin was normal in appearance. Clinical
Diagnosis- Foreign body granuloma/ Necrobiotic granuloma/ Tendinous xanthoma.
Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 52/ December 30, 2013 Page 10284
CASE REPORT
FIG. 1: SWELLING OVER RIGHT INDEX FINGER- DISTAL PHALANX.
Radiological findings- There was evidence of reduced joint space with eccentric soft tissue swelling and also eccentric growth of distal carpel bone along the lateral surface of index finger with increased sclerosis along the articular surface.
FIG. 2: RADIOGRAPH SHOWS
REDUCED JOINT SPACE
AND ECCENTRIC SOFT TISSUE with polygonal cells appearing like synoviocytes. Few spindle nuclear cells also seen with sparse lymphocytes. Present cytomorphology was suggestive of BENIGN GIANT CELL TUMOR OF TENDON
SHEATH- BENIGN SYNOVIOMA. No Malignant cells seen.
Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 52/ December 30, 2013 Page 10285
CASE REPORT
FIG. 3: CYTOLOGY SMEAR- 40X VIEW SHOWS
MULTINUCLEATED GIANT CELLS.
FIG. 4: CYTOLOGY SMEAR- 40X VIEW SHOWS
MANY ISOLATED SYNOVIOCYTES.
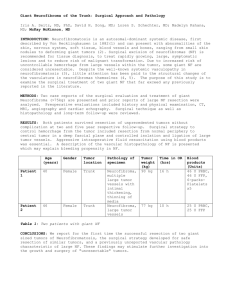
Histopathology- On Gross examination, tissue showed papillary villous projections and nodular structures. Cut surface showed variable coloring, including yellow and red areas, depending on lipid and hemosiderin Content. Microscopic examination revealed cellular infiltrates of mononuclear cells.
These cells showed oval nuclei with vesicular or clumped chromatin and prominent cytoplasm.
Hemosiderin-laden mononuclear cells, multinucleated giant cells and foam cells were present. The histopathological features were consistent with cytological diagnosis.
FIG. 5: HISTOPATHOLOGY SMEAR 40X VIEW SHOWS MONONUCLEAR CELLS,
MULTINUCLEATED GIANT CELLS AND HEMOSIDERIN LADEN MONONUCLEAR CELLS.
DISCUSSION: Giant cell tumour of the tendon sheath or pigmented nodular synovitis, is a benign neoplasm that develops in the synovium of joints, tendon sheaths, and bursae. This tumor has a chromosomal translocation, t(1:2)(p13;q37), which results in overexpression of CSF1, a chemoattractant for macrophages. Benign Synovioma are rare and pose problem in diagnosis.
Multiplicity adds on to confusion in its diagnosis.
The present case is rare in diagnostic cytopathology. Pathologist continue to look at it from different angles in an attempt to answer questions such as whether its neoplastic or non neoplastic, its morphological and ultrastructural features have to be studied carefully.
Monaghan et al reported Giant cell tumour of tendon sheath (GCTTS) and studied clinicopathological features of 71 cases. Clinical data, obtained from pathology request forms and in
Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 52/ December 30, 2013 Page 10286
CASE REPORT patient notes, along with the gross and microscopic appearances of 71 cases of GCTTS were evaluated. The hands were involved in 66 of 71 patients, the feet in three patients, and tissues around the knee in two patients. The most common sites in the hands were the fingers. The index, middle finger and the thumb were more commonly involved than the ring and the little finger. The lesion occurred more commonly on the fingers of the right hand (37 patients) than those on the left hand (23 patients).
(5) Our study reported a 45 year old woman with a swelling over the course of tendon of the Right Index Finger-Distal Phalanx, which was diagnosed as giant cell tumor of tendon sheath. The location of the tumor was found to be same in both the studies.
Ueno et al reported a child with giant cell tumor of tendon sheath with a painless nodule on right index finger .(6)
Llauger et al reported a 60 year old woman with localized giant cell tumor of tendon sheath who presented with slowly enlarging mass on the thumb .(7)
Agarwal et al reported cytomorphology of giant cell tumor of tendon sheath in 2 cases. He reported these swellings on the toe. Preoperative diagnosis by FNAC is accurate and is important for two reasons. First, an accurate preoperative diagnosis can minimize the high recurrence rates which range between 10-20%. Second a more extensive surgical procedure can be prevented. (8)
CONCLUSION: In conclusion, Giant cell tumor of tendon sheath is a relatively rare soft tissue tumour of uncertain histiogenesis. Complete local excision is the treatment of choice When both clinical and cytologic features of the case are taken into account, the diagnosis can be usually made with certainty.
REFRENCES:
1.
Darwish F M, Haddad W H. Giant cell tumour of tendon sheath:experience with 52 cases.
Singapore Med J. 2008; 49 (11) : 879.
2.
Martin RC, Osborne DL, Edwards MJ, Wrightson W, McMasters KM. Giant cell tumor of tendon sheath, tenosynovial giant cell tumor, and pigmented villonodular synovitis: defining the presentation, surgical therapy and recurrence. Oncol Rep. 2000 Mar-Apr;7(2):413-9.
3.
Darling J.M, Goldring S.R, Harada Y, Handel M, Glowacki J, and Gravallese E.M. Multinucleated cells in pigmented villonodular synovitis and giant cell tumor of tendon sheath express features of osteoclasts. Am J Pathol. 1997 April; 150(4): 1383–1393.
4.
Athanasou N, Quinn J, Ferguson D, McGee J.Bone resorption by macrophage polykaryons of giant cell tumour of tendon sheath. Br. J. Cancer (1991);63, 527-533.
5.
Monaghan H, Salter D.M, Al-Nafussi A. Giant cell tumour of tendon sheath (localized nodular tenosynovitis): clinicopathological features of 71 cases. J Clin Pathol 2001;54:404–407.
6.
Ueno T, Shin-ichiAnsai, Omi T, Kawana S. A child with giant cell tumor of tendon sheath.
Dermatology Online Journal 2011; 17 (5): 9.
7.
Llauger J, Palmer J, Roson N, Cremades R, Bague S. Pigmented Villonodular Synovitis and Giant
Cell Tumors of the Tendon Sheath:Radiologic and Pathologic features. AJR:1999;172:1087-
1091.
8.
Agarwal P, Gupta M, Srivastava A, Agarwal S. Cytomorphology of Giant Cell Tumor of Tendon
Sheath: A Report of Two Cases. Acta Cytol 1997; 41:587-589.
Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 52/ December 30, 2013 Page 10287
CASE REPORT
AUTHORS:
1.
Sarandeep Singh Puri
PARTICULARS OF CONTRIBUTORS:
1.
Senior Resident, Department of Pathology,
Jawaharlal Nehru Medical College, Sawangi
(Meghe), Wardha, Maharashtra.
NAME ADDRESS EMAIL ID OF THE
CORRESPONDING AUTHOR:
Dr. Sarandeep Singh Puri,
R-12/72, Raj Nagar,
Ghaziabad, Uttar Pradesh,
PIN – 201002, India.
Email- drsarandeep147@gmail.com
Date of Submission: 10/12/2013.
Date of Peer Review: 11/12/2013.
Date of Acceptance: 17/12/2013.
Date of Publishing: 27/12/2013
Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 52/ December 30, 2013 Page 10288