Perception Attention Memory Dr A Hooper 7th Nov 2014
advertisement

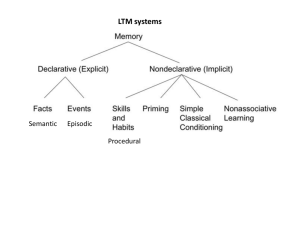
Dr Alexandra Hooper Clinical Psychologist CAMHS Information received through the sensory organs is vast and constantly changing - therefore we must establish some form of order. We have a preference for whole objects “the whole is greater than the sum of the parts” Proposes the brain organises itself in regular and predicable ways – largely innate Perceptual grouping eg squareness Look for organised wholes in figure ground differentiation Rubin – visual separation of an object from its setting Visual field can be divided into two basic parts; figure and ground. Only able to focus on one at a time – the figure and ground cant be seen simultaneously as ground becomes figure when the focus is shifted Law of Closure – we fill in the blanks in order to complete a regular figure / object: Law of Similarity – Organised together if they look similar. This might depend of relationships of form, colour, size or brightness Law of Proximity – the closer two figures are to each other the more we will group them together perceptually: Law of Symmetry – Symmetrical images are perceived collectively: Law of Continuity – we group with as few interruptions as possible: Law of Common Fate – elements seen moving together are perceived as belonging together. The ability to perceive an object as unchanging and constant under changing conditions ◦ Size / depth constancy: Object is same size regardless of distance (as object recedes it is not seen as decreasing in size) Appearing in infants only a couple of weeks old, although not believed to be innate. ◦ Shape Constancy: we perceive the shape of the object more or less independently from the angle from which it is viewed ◦ Brightness constancy: enable us to view object as being the same apparent lightness and colour despite change. Objects appear the same colour at sunset even though proportionally there is far more red light in the sun-light. Example of object constancy: http://www.youtube.com/watch?v=RyFPfsxT18&feature=relmfu GIBSON Perception is a sensation that occurs primarily within the CNS with little further processing Directly determined by the information presented to the sensory organs. Primary function of perception is to facilitate interactions between individual and environment. ◦ Optic flow: the point which we appear motionless while other parts of the optic field move more rapidly (pilot take off/land) ◦ Textual gradients: This gives information about depth. Objects which are closer can be seen in greater detail than objects further away ◦ Affordances: Objects afford (offer) us information about their function and the opportunity to use them in some way. How we use them depends on a combination of information from the optic array, the physical surroundings and the person’s psychological and physiological state. GREGORY Perception involves analysis of sensory information. We only attend to some information and then fill in the gaps according to what we know and expect to see according to our prior knowledge of the world Actively construct our own perception Problem solving – hypothesis testing when sensory input is unusual. GIBSONS THEORY What is the role of stored knowledge? Where is visual perception studied? Is perception inbuilt or constructed? GREGORYS THEORY Misrepresentations of external stimuli ◦ Gregory took illusions as evidence of his theory Gregory and Allport Directly relevant to Gregorys view that perception is an active process involving selection, inference and interpretation We select what we perceive and then interpret it according to different factors ◦ context ◦ previous instructions ◦ personality ◦ previous experience ◦ cultural factors ◦ perceptual accentuation (like)/ defence (dislike) Factors which influence or induce set include: ◦ Motivation ◦ Emotion ◦ Values ◦ Beliefs ◦ Cognitive styles ◦ E.G. Hungry people more likely to see pictures which are neutral or ambiguous as food. ◦ Anxious people respond more quickly to the presentation of threatening material. (clinical implications) Babies can perceive light in the womb Colour seen by 4/12 Depth perception is innate and develops early but avoidance takes 4-6/12 Blind since birth – receives successful corneal transplant ◦ Certain aspects of visual perception were innate such as detection (scanning of a shape such as a triangle, however figural identity (recognising and naming shape as a triangle) is learnt through experience. ◦ Patient S.B. Relevant clinically ◦ E.g. Depth perception may be abnormal in those with schizophrenia ◦ Illusions are real objects or stimuli that have been distorted (e.g. dark shadow in a bush) ◦ Hallucinations are perceptions which are not related to any external stimuli and are internally generated But are perceived as actually external Can be found in schizophrenia, personality disorder and epilepsy Also in Charles Bonnet Syndrome in which patients with visual loss and a lack of normal nerve impulses reaching the brain, have complex visual hallucinations – when the brain attempts to interpret the signals it may generate spontaneous nerve activity which causes the hallucinations. http://www.youtube.com/watch?v=vJG698U2Mvo http://www.youtube.com/watch?v=lHd_L7dg3U4 Information Processing ◦ Information is any input – tactile, visual, auditory etc. ◦ Processing refers to any action or function carried out on this information. E.g. visual information is processed to provide derivative information about depth, contour etc. Information processing is mostly automatic “It is the taking possession by the mind, in clear and vivid form, of one out of what seems several simultaneously possible objects or trains of thought. Focalisation, concentration of consciousness are of its essence. It implies withdrawal from some things in order to deal effectively with others.” To cope with the vast amount of information, we must selectively attend to only some information and somehow ‘tune out’ the rest. ◦ Focussed attention: Attending solely to one source of info whilst being distracted by another (e.g. cocktail party phenomenon – listening to one of two voices in a hubbub of others) ◦ Divided attention: Attending to two or more sources of attention simultaneously (E.g. driving and answering your phone) 1. 2. 3. Eyesnck & Keane (1995) identified 3 factors which affect our ability to perform two tasks at one: Difficulty - Generally the more difficult the task the less successful dual task performance is (subjective) Practice – Practice improves dual task performance. This could be because people develop new strategies for performing each task minimising interference between them Similarity – When people are asked to attend to two different stimulus modalities it is more successful Broadbent’s (1958) Filter Model Schizophrenia: Attention difficulties due to the lack of early filtering and a consequent overload at the late stage of processing Attention focus: anxious subjects search for threat-congruent material, detecting it more quickly than controls – which is maintenance factor in anxiety disorders “Without the capacity to remember and to learn it is difficult to imagine what life would be like, whether it could be called living at all. Without memory, we would be servants of the moment, with nothing but our innate reflexes to help us deal with the world. There would be no language, no art, no science, no culture. Civilisation itself is the distillation of human memory.” Refers to the way in which we record the past and utilise it for later so it can affect the present: ◦ The SENSORY STORE: very brief store for the first level of observation including visual iconic (up to 0.5 second) and auditory echoic memory (up to 2 seconds) ◦ The SHORT TERM MEMORY: Suggested to be 0-18s long where information that is processed is either sent to the long term memory or lost. The short term memory is proposed to have a capacity of 7 (+/- 2) ◦ The LONG TERM MEMORY: ‘indefinite’ storage consisting of episodic and semantic memories. 1. DECLARATIVE (EXPLICIT) MEMORY: Refers to memories which can be consciously recalled such as facts and knowledge: 1. Semantic Memory: Stores factual information – memory of meanings, understandings and other concept based knowledge unrelated to specific experiences. (E.g. Are wrenches pets or tools? – you can answer without remembering any specific event in which you learnt that wrenches are tools. 2. Episodic Memory: Stores specific personal experiences – Memory of autobiographical events that can be explicitly stated. Events that are recorded in episodic memory may trigger episodic learning (e.g. bitten by a dog results in fear of dogs is episodic learning) Conscious, intentional recollections of previous experiences and information – use explicit memory throughout the day e.g. remembering time of appointment or recollecting an event from years ago. 2. PROCEDURAL (IMPLICIT) MEMORY: The memory of how to do things. Guides the processes we perform without the need for conscious control or attention. Automatically retrieved and used for the execution of the integrated involved in both cognitive and motor skills (e.g. tying your shoes or reading) Implicit memory in which previous experiences aid in the performance of a task without conscious awareness of these previous experiences. Encoding: Refers to the registration of the information. The information processing system codes the new/incoming information – can be affected by the ‘serial position effect’ (primary and recency effects) which means information presented first is remembered best and information presented last is remembered second best. ◦ Coding affected by characteristics of the individual – an unknown language will be coded as sounds (phonemically), while one familiar with the language will code it as language – extracting meaning from the sounds. Storage: Refers to the holding of information ◦ Storage is unlimited and permanent where any ‘memory loss’ is likely due to retrieval problems. The information must be consolidated from the short term memory to the long term memory. Retrieval: Process of returning information from the long term memory to the short term memory. ◦ Most retrieval is unconscious such as from social behaviour and object recognition ◦ Retrieval is not necessarily the same as recall – e.g. ‘tip of the tongue’ phenomenon, where a word has failed to be retrieved properly from memory, combined with partial recall . ◦ Retrieval easier if cues are present. ◦ Retrieval and Emotion: Mood (especially low mood) can affect retrieval. Depressed participants tend to recall more negative personal events and recall more negative words from a word list. Anterograde Amnesia: Refers to sufficient memory for any information before accident, but severe deficits with learning new information. ◦ Normal short term memory, but cant transfer information to long term (or is it a deficit with retrieval?) ◦ No knowledge of current affairs, time of day or family events http://www.youtube.com/watch?v=Vwigmktix2Y ◦ Retrograde Amnesia: Refers to a loss of information / forgetting what happened prior to accident. ◦ Induced with clinical use of electric therapy (ECT) Central Executive: Controls attention and coordinates the actions of the other components, briefly stores information but has limited capacity. Phonological Loop: Consists of two parts: ◦ Articulatory Control System (The inner voice) Rehearses information verbally and has time based capacity of about 2 secs. Mentally rehearses the information by repeating it over and over again. ◦ Phonological Store (The Inner ear) Sound based code to store information, decays after 2 seconds, unless rehearsed by articulatory control system. Receives its input either directly from the ears or from long term memory – if you imagine your favourite piece of music you are using your phonological store. Visuo-spatial Sketchpad: Stores and manipulates visual information, from the eyes or long term memory. If you imagine an object then picture it rotating you are using your visuospatial sketchpad Episodic Buffer: More recent addition to the WMM (Baddeley, 2000) – purpose is to bind together all the information from the other components of working memory with information about time and order. This prepares the memories for storage in episodic long term memory. Semantic Memory: Refers to memory for meanings and may be described as ‘knowing that’, as opposed to ‘knowing how’ Episodic Memory: Memory explicitly recalled and described – this is memory for places, events and so on. Memory for these episodes tend to be fairly sharp Procedural Memory: Often difficult or even impossible to recall explicitly. Memories of this type include ‘knowledge of’ e.g. how to ride a bike. The series of steps required to perform this act may not be explicitly known, but the action may be performed. Another example is language – which is performed according to a set of grammatical rules which most individuals would not be able to articulate and yet clearly follow. Decay Theory: Refers to memory fading merely over the course of time – the memory itself as well as the strength of the memory fades. Interference Theory: ◦ Proactive interference – refers to when previous learning/memories may impair an individuals ability to retain new memories (e.g new phone number) ◦ Retroactive interference –refers to a phenomenon which occurs when information recently learnt interferes with and impedes the recall of previously learnt information ◦ Output interference – refers to when the initial act of recalling specific information interferes with the retrieval of the previous, original information (e.g. creating a list of items to purchase but then forgetting to take the list – it would be proposed that the act of remembering a few items of the list would decrease the probability of remembering the other items. Amnesia: either anterograde or retrograde. Impairment of the ability to form and store new memories. Dementia: serious impairment in cognitive abilities in terms of language, attention and memory, compared to what may be expected at that age. May be the result of a unique, global brain injury or a progressive decline due to damage or a disease in the body. Psychogenic fugue: sometimes referred to as dissociative fugue – refers to a rare psychiatric disorder characterised by reversible amnesia for personal identity including memories and personality and other characteristics of individuality. Often precipitated by severe psychological or social stress. Lasts hours to days. Hippocampus and amygdala involved in the transition between S/T and L/T stores Also used for regulating different hormones and emotional and physical reactions to situations, including emotional stress or trauma ◦ Repressed memory ◦ Intrusive memory