Occupational poisoning
advertisement

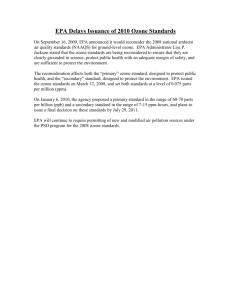
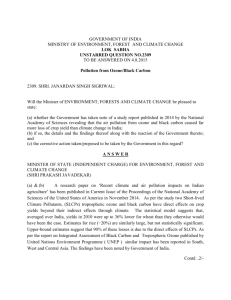
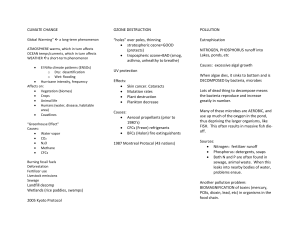
Occupational poisoning By: Sotoudeh manesh MD Occupational medicine specialist Introduction Poison: – Any substance that, when administered to a living organism, causes a harmful effect. Poisoning: – The morbid condition produced by a poison. Toxic: – Term used to describe a chemical that has the ability to cause harmful or fatal effects upon exposure to humans, animals, or plants. • Toxicity: – The capacity of a substance to induce damage to living tissue. Toxicity can be acute, chronic, local, or systemic. (Lewis Dictionary of Occupational and Environmental Safety and Health) Introduction • Common occupational toxic substances can be divided into 4 groups: 1. Heavy metals 2. Pesticides 3. Organic solvents 4. Gases, vapors and particulates Particulates Classification of particles by size: 1. Non-inhalable particle – Larger than 200 μm (0.2mm) 2. Inhalable particle (nasopharyngeal region) – Smaller than 200 μm (0.2mm) – Deposit in nose or trachea 3. Respirable particle (alveolar region) – Smaller than 10 μm (0.01mm) – Deposition in alveolar area (e.g. pneumoconiosis) Water Solubility gases Example Site of injury High Ammonia,formaldehyde Upper airway Moderate Chlorine,sulfur dioxide Lower airway Low NOx ,phosgene Lung parenchyma >10 Dust Upper airway 2.5 – 6 Fire smoke particle Lower airway < 2.5 Fume ,asbestos fibers Lung parenchyma Particle size Gases, vapours and particulates Definitions: • gas is a term usually applied to a substance that is in the gaseous state at room temperature and pressure • vapour is applied to the gaseous phase of a material that is ordinarily a solid or liquid at room temperature and pressure • aerosol is applied for a relatively stable suspension of solid particles in air, liquid droplets in air or solid particles dissolved or suspended in liquid droplets in air • mists and fogs are aerosols of liquid droplets formed by condensation of liquid droplets on particulate nuclei in the air • fumes are solid particles formed by combustion, sublimation or condensation of vaporised material • dusts are solid particles in air formed by grinding, milling or blasting • fibres are solid particles with an increased aspect ratio (the ratio of length to width); they have special properties because of their ability to be suspended in air for longer periods than dusts and other aerosols. Smog : Toxic gas General consideration Odors Asphyxiant solubility Factors affecting the dose of inorganic gas delivered to the respiratory system Physicochemiacal factors Concentration Duration Minute of exposure ventilation Toxicity of Gases and vapours • Asphyxiation: simple asphyxiation – ability of a gas or vapour to displace oxygen from air by dilution • Carbon dioxide • Nitrogen (N2) • Inert gases such as helium, argon and neon. toxic asphyxiants – by interfering with the ability of the body to transport oxygen. • Carbon monoxide • Cyanides • Hydrogen sulfide • Irritation to the tissues in respiratory system – Ammonia – Chlorine • Sensitisation – asthma CASE1 آقاي 26ساله با سردرد يك ماهه در آذرماه مراجعه كرده.دو مرتبه توسط متخصص مربوطه با تشخيص سردرد ناشي از استرس و تشديد در اثر فيومهاي محيط كار بررسي شده است. : PHx سابقه يك مرتبه سردرد در نوجواني مي دهد.سردرد اخير در حدود4ماه قبل شروع شده كه به تدريج از نظر شدت و تواتر بيشتر شده و بهOTCپاسخ مناسب نمي دهد.سردرد رترواربيتال با انتشار به پشت سرهمراه باحساسيت به نور و سروصدا و گاهي تهوع مي باشد. OHx شغل نجار و كار بر روي محصوالت روكش داربه مدت 6ماه10.نفر همكار ديگر هم دارد.فضاي کارگاه 100*25مترمي باشد.در داخل كارگاه يك اتاقك كوچك باز جهت اسپري كردن و استفاده از مواد جال دهنده با تهويه و يك بخاري گازي وجود دارد.درب كارگاه در فصل زمستان كامال بسته مي شود. :Task استفاده از مواد جال دهنده :MSDS حدود %70متيلن كلرايد،تولوئن،متيل اتيل كتون،ايزوپروپيل الكل،اتيل استات ،ايزوپروپيل الكل CO poisoning Colorless, odorless and non irritant 40000 emergency visit in USA CoHb:0.5%in nonsmoker adult and 1% in adult that typically exposed in environment CO poisoning Exposure setting Incomplete combustion Smoking:400ppm(0.04%) PEL:50 ppm CoHb:3-8% occasionally up to 15% Inadequate ventilation Methylene chloride CO poisoning Environmental measurement Colorimetric device Electronic short testing devices CO2 measurement(in home) CO poisoning Biologic monitoring CoHb COHb=[Co]air*KT 220 times affinity co for Hb as O2 Half time=320min CO poisoning pathophysiology Reduce the oxygen-carrying Alter arterial oxygen tension and hemoglobin saturation Cytochrome effect Reoxygenation and demyelination CO poisoning Acute clinical effect Non-specific =viral infection COHb 5%:visual perception , +hypoxia without hyeperventilation COHb>5%:tissue hypoxia,vasodilation ,…syncope….lactic asidosis and hyperventilation…..seizure,coma,cardiac arrhythmia,MI,Sudden death Cherry red lips Retinal hemorrhage Erythematous lesions with bullae over bony prominences Sweat gland necrosis Lab:PaO2,Pulse oximetry,CO oximetry CO poisoning Delay effects Incidance:10-30% 2-40days Mental deterioration, mood dis,unusual behavior, gait and other movement disturbance, parkinsonian deficit ,focal neurological sings CO poisoning Chronic effects Erythrocytosis Angina Atherosclerosis??? CO Poisoning Signs and symptoms closely resemble those of other diseases. Often misdiagnosed as: Viral illness (e.g., the “flu”) Acute coronary syndrome Migraine Estimated that misdiagnosis may occur in up to 30-50% of CO-exposed patients presenting to the ED. Source: Raub JA, Mathieu-Holt M, Hampson NB, Thom SR. Carbon Monoxide Poisoning: A Public Health Perspective. Toxicology 200;145:1-14 Cherry red skin Signs and Symptoms color is not always present when Severityand, CO-Hb Signs & Symptoms present, Level is often COHb levels do not Mild a late finding. < 15 - 20% Headache, nausea, vomiting, dizziness, blurred always correlate vision. symptoms nor Moderate 21 - 40% Confusion, syncope,with chest pain, dyspnea, weakness, tachycardia, tachypnea, rhabdomyolysis. predict sequelae. Severe 41 - 59% Fatal > 60% Palpitations, dysrhythmias, hypotension, myocardial ischemia, cardiac arrest, respiratory arrest, pulmonary edema, seizures, coma. Death CO poisoning Clinical evaluation Clinical suspicion COHb measurement or CO measurement in exhaled air Neurology neuropsychology evaluation CO poisoning Management Remove O2 100% Mechanical ventilation Hyperbaric oxygen therapy any period of unconsciousness COHb>40% Pregnancy and COHb>15% Sign of cardiac ischemia and arrhythmia PHx of IHD and COHb>20% Symptom don’t resolved after 4-6h with 100%O2 RECURRENT SYMPTOM after 3W case2 آقاي 40ساله با شرح حال تماس با پودر و مواد جواهرسازی توسط همكاران به اورژانس آورده مي شود.وي داراي يك مغازه طالسازي و پرداخت كننده طال مي باشد.در روز حادثه در هنگام كار با مواد صيقل دهنده fanباالي سرش را روشن مي كند و پودر در داخل مغازه پراكنده مي شود.بالفاصله فرد سريعا دچار تهوع ،استفراغ و احساس سوزش در سراسر بدن مي شود .توسط همكاران به بيمارستان ارجاع مي شود .در هنگام مراجعه فرد هوشيار و اورينته PR=80و .BP=100/60معاينه شكم و ريه نرمال است 4.مرتبه LOOSE STOOLداشته است .سرگيجه تنگي نفس و خونريزي و تشنج نداشت.بعد از 2ساعت BPكاهش مي يابد. pH 7.30, pO2 50, pCO2 23, HCO3=11.6, ABGبود .اقدامات ساپرتيو موثر نبود و فرد در نهايت فوت نمود Hydrogen cyanide is a colorless or pale blue liquid or gas with a faint bitter almond like odor Cyanide Hydrogen cyanide is formed during the incomplete combustion of nitrogen- containing polymers, such as certain plastics, polyurethanes, and wool. Hydrogen cyanide is present in cigarette smoke HUMAN EXPOSURE: Cyanides are well absorbed via the gastrointestinal tract or skin and rapidly absorbed via the respiratory tract. Once absorbed, cyanide is rapidly and ubiquitously distributed throughout the body, although the highest levels are typically found in the liver, lungs, blood, and brain. Cyanide Usage Insecticides & rodenticide Electroplating Nylon Metal cleaning PEL:10PPM, IDHI:50PPM Cyanide measurement Difficult BM:thiocyanate level in blood or urine Cyanide pathophysiology Cytochrome oxidase enzyme Cyanide clinical features Mild: bitter almond taste, irritation of mucous membrane, dyspnea,headache, dizziness, nausea and vomiting, agitation Severe:hypotention ,arrhythmias, cardiogenic and non-cardiogenic pulmonary edema,lactic acidosis,seizure,coma, Cherry red skin color Acute cyanid exp :hyperpnea,respiratory arrest Delay effect:leukoencephalopathy Cyanide chronic clinical effects Skin and MM irritation and ulcer Thyroid gland enlargement Rash, bitter almond ,headache Smokers amblyopia Cyanide management Sodium nitrate: 10ml of 30%solution(300 mg) over 5-20 min Amyl nitrate:0.3ml ampoule crushed every minute inhalation Sodium thiosulfate:50ml 25%solution(12.5g)IV over 10 minute Hydroxycobalamine:10ml of 40% solution(4g) iv over 20 min Case3 آقاي 27ساله –كارگر دامپروري -به منظور تميز كردن پمپ داخل گودالي از كود به عمق 6متر مي شود.پس از پايين رفتن در حدود 3متر داخل گودال سقوط مي كند.همكار فرد داخل گودال مي شود تا وي را نجات دهد كه او نيز به داخل گودال سقوط مي كند20.دقيقه بعد نيروي امداد مي رسد و با كمك آپارات هردو را خارج مي كند ولي هردو نفر در مسير بيمارستان فوت مي كنند Hydrogen sulfide general consideration Irritant Asphyxiant in cellular level and inactive cytochrome oxidase Odor threshold: 5ppm :rotten eggs Irritant threshold: 10ppm >100ppm: toxic effect on the olfactory nerve Hydrogen sulfide exposure Decay of organic sulfur-containing material: sewer gas Petroleum process Hydrogen sulfide acute clinical effects CNS abnormality :rapid loss of consciousness“knockdown” Respiratory paralysis Tachycardia and hyperpenea,cv collapse Irritation effects: from MM to pulmonary edema Hydrogen sulfide chronic clinical effects Irritation Loss of odor sensation Cognitive and personality H2S Awareness Concentration Health Effects 10 ppm Beginning eye irritation 50-100 ppm Slight respiratory tract irritation after 1 hour exposure. 100 ppm Coughing, eye irritation, loss of sense of smell after 2-15 minutes. Altered respiration, pain in the eyes, and drowsiness after 15-30 minutes followed by throat irritation after 1 hour. Several hours exposure results in gradual increase in severity of these symptoms and death may occur within the next 48 hours 200-300 ppm Severe respiratory tract irritation after 1 hour of exposure. Possible pulmonary edema (fluid in the lungs). Loss of consciousness and possibly death in 30 minutes to 1 hour. Rapid unconsciousness, loss of respiration, and death after 1-3 minutes. Unconsciousness at once, loss of respiration and death in a few minutes. Death may occur even if individual is removed to fresh air at once. 500-700 ppm 700-1,000 ppm 1,000-2,000ppm Hydrogen sulfide clinical evaluation Awareness of the circumstances: patients breath , clothing Urinary thiosulfate?? Hydrogen sulfide management O2 100% nitrate CASE4 آقاي 49ساله تكنسين تعميرات يخچال با تنگي نفس شديد ،سرفه و ويز مراجعه كرده است.نامبرده عنوان مي كند در هنگام جوشكاري بر روي لوله هاي پشت يخچال دچار اشك ريزش و احساس سوزش در دهان و گلو شده است كه به تدريج بدتر شده است.در هنگام جوشكاري بوي سبزي گنديده به مشامش رسيده است.در هنگام مراجعه ديسپنه و ويز بازدمي دارد.قرمزي HR=95 BP=110/60 چشم و به نظر كانژكتويت دارد. O2sat=98%مي باشد CBC.و بيوشيمي خون طبيعي است. تشخيص: Phosgene general consideration Synonyms: carbonic acid dichloride ,carbonyl chloride,chloroformyl chloride, carbon oxychloride Colorless ,low solubility, oxidant gas, odor rotting vegetables Phosgene exposure Usages: isocyanate ,coal tar, dyes, pharmaceuticals,insecticidesd Chlorinated hydrocarbon are heated: welding of metals degreased with solvent(trichloroethylene &trichloroethane) or carbone teracholoride as a fire fighting Phosgene measurement IR spectrophotometry , GC, phosgene indicator badges Phosgene clinical effects acute Irritation of MM, Alveolar injury: acute pneumonitis , pul edema Delay?? Chronic PFT abnormalities Phosgene managements Observe at least for 24h Patent of airway O2 Positive pressure ventilation Corticosteroids Supportive: theophylline, salbutamol CASE5 آقاي 59سال شاغل در كارخانه استحصال مس به علت ضعف عمومي ،دردشديد عضالني ،تعريق شديد ،لرز همراه با ادرار تيره(شبيه خون)همراه با تهوع،استفراغ صفراوي توسط همكاران آورده شده است.هوشيار است و هرگونه درد شكمي و تروماي شكم،سابقه بيماري خوني و يا كليوي را انكار مي كند.سابقه گاستريت مزمن دارد كه گاهي اومپرازول مصرف مي كند. T=36.8 HR=78 BP=130/80 RR=18 Hb=13.8 WBC=18000 PLAT=109000 Cr=1.55 Urea=80 Pro(+3) WBC=80 RBC=1-2 Epi=more سونو:مختصر ادم اطراف كليه راست.ساير موارد،مثانه و پروستات نرمال به بخش ارولوژي منتقل شد.ولي بعد از چند ساعت وضعيت عمومي فرد بدتر شد.يرقان،تب،اسهال،كاهش سطح هوشياري پيدا كردHb=8 Bill=5.8(indirect) . WBC=20000 Cr=3.59 urea=188 تشخيص؟ اقدام؟ Arsine gas (AsH3) A colorless & odorless gas at low concentration but smell of “garlic” at high concentration • Generated when arsenic containing metals contact with strong acid • Intravascular hemolysis ( abdominal pain, vomiting, hemoglobinuria, renal failure) Arsine gas (AsH3) Acute effect of arsine Abdominal pain,oliguria,jaundice Headache,vertigo,hemathemesis,EKG change Laboratory findings Anemia,LDH ,reticolositosis,billirobin hemoglobinuria Arsenic (As)• Three forms: Inorganic, organic, arsine gas • Used as insecticides and herbicides, in glassware, alloy and pigment production, and in the semiconductor industry • Occupational exposure mostly to inorganic arsenic: – those involved in the processing of copper, gold, and lead ores. – Agriculture (pesticides) • The organic arsenic[V] forms are less toxic than the inorganic arsenic[III] forms Acute Arsenic Poisoning May follow the ingestion of deliberately or accidentally contaminated food or drink • Gastrointestinal: metallic or garlic taste, dry mouth, dysphagia, abdominal pain, profound vomiting, and diarrhea with rice water stools – Shock → multi organ failure → death • Survivors often develop: • Bone marrow suppression (anemia, leukopenia) – Hemolysis – Hepatomegaly – Melanosis – Polyneuropathy Chronic arsenic poisoning • More common form of arsenic poisoning • Skin : pigmentation, depigmentation, cancer • Peripheral nerves: sensorimotor neuropathy • Liver: Cirrhosis • CVS: hypertension • Blood: Megaloblastic anemia • Others: nasal perforation Ozone’s Effects on Health: A Story of Good and Bad Where Healthcare Meets Policy We Must First Understand Ozone to Understand the Effects It Has on Our Health Ozone: Discovered in a lab in the mid 1800s From the Greek ozein – “to smell” A pungent blue gas, detectable in small amounts Chemical Formula: O3 Highly reactive with many chemicals Source: Fahey DW. Twenty Questions and Answers About the Ozone Layer. Available at: http://www.epa.gov/ozone/science/unepSciQandA.pdf. Accessed February 9, 2005. What Are the Differences Between Ozone in the Stratosphere and the Troposphere? Stratospheric Ozone • 90% of all ozone exists in “ozone layer” – Naturally forms during chemical reactions between UV sunlight and O2 – 12,000 ozone molecules per billion air molecules – Shields humans from harmful UV rays/stabilizes weather Tropospheric Ozone • 20–100 ozone molecules per billion air molecules • It’s the result of human pollution – Irritates the heart and lungs and traps heat (global warming) Sources: Fahey DW. Twenty Questions and Answers About the Ozone Layer. Available at: http://www.epa.gov/ozone/science/unepSciQandA.pdf. Accessed February 9, 2005. Bell ML, McDermott A, Zeger SL, Samet JM, Dominici F. Ozone and short-term mortality in 95 US urban communities, 1987-2000. JAMA. 2004;292:2372-2378. Some Human-Produced Chemicals Can Destroy Stratospheric Ozone UV protection Weather stabilization Deplete ozone Refrigerants Air conditioning Foam blowing Industrial cleaning Chlorofluorocarbons (CFCs) (Stable in troposphere) Release chlorine Stratosphere CFCs Broken Down by UV Rays Bromine-containing compounds are even more destructive Sources: Fahey DW. Twenty Questions and Answers About the Ozone Layer. Available at: http://www.epa.gov/ozone/science/unepSciQandA.pdf. Accessed February 9, 2005. US Environmental Protection Agency. Ozone Depletion Glossary. Available at: http://www.epa.gov/Ozone/defns.html. Accessed February 9, 2005. Pollution Produces Bad Ozone in the Troposphere Naturally degraded by chemicals, soils, plants Fossil fuel combustion Hydrocarbons + Nitric Oxides + Sunlight Little escape to stratosphere Hospitalization Emergency room visits Respiratory disease Lung function Death rates Ozone Source: Fahey DW. Twenty Questions and Answers About the Ozone Layer. Available at: http://www.epa.gov/ozone/science/unepSciQandA.pdf. Accessed February 9, 2005. High Ozone Levels in the Troposphere Increase the Risk of Premature Death Ozone Limits Maximum 8-hour standard of 80 parts per billion (ppb) Study of 95 U.S. Cities (1987-2000) Average daily ozone concentration: 26 ppb Daily mortality increased .52% per 10 ppb increase in surface ozone Age 65–75 Years: daily mortality increased .70% Sources: Bell ML, McDermott A, Zeger SL, Samet JM, Dominici F. Ozone and short-term mortality in 95 US urban communities, 1987-2000. JAMA. 2004;292:2372-2378. US Environmental Protection Agency. National Ambient Air Quality Standards for ozone, final rule. Federal Register. 1997;62:38855-38896. Cited in Bell ML, McDermott A, Zeger SL, Samet JM, Dominici F. What Do We Now Know About Ozone and Its Effects on Health? Ozone in the upper atmosphere is GOOD • Both are under human control Ozone in the lower atmosphere is BAD • Policy and regulations are needed – to decrease use of ozone-harmful compounds – to control release of hydrocarbons and nitric oxides Ammonia General consideration Soluble, colorless, pungent odor, irritant Ammounium hydroxide with water reaction and necrosis Exposure Cleaning agents Refrigeration equipment, plastic, explosive, fertilizer Ammonia clinical effects Acute Irritation of MM skin: , sever edema of the larynx; upper airway obstruction Chemical bronchitis, bronchospasm, pul edema Blindness and …. Complete recovery to RADS, bronchopneumonia,bronchiectasis,air way stenosis, bronchiolitis obliterans Chronic Reversible eye, nose, throat irritation Ammonia management Observe for24 h Airway patency O2 Bronchodilator Steroids?? Chlorine Yellowish green gas, strong odor,sensory irritation,, Usage & exposure: making paper, bleaching(janitorial cleaning),accidental in transport and spill , sewage treatment Chlorine clinical effects Acute Minor mucosal to pulmonary irritation and edema and RADS Chronic Air flow obstruction Chlorine management Observe for progressive airway and lung injury Evaluation: PFT, ABG, CXR TREATMENT: supportive.steroide??