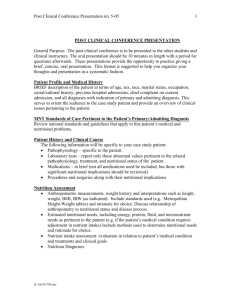
Nutritional Analysis Form - Eastern Illinois University
advertisement

Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Dear Nutritional Analysis Participant: Thank you for your interest in the Health Education Resource Center’s (HERC) Nutritional Analysis program! I look forward to providing you with a very pleasant and educational experience, and am excited to work with you towards healthy nutrition and lifestyle goals. Included in the Nutritional Analysis packet are several forms that need to be filled out and returned to the HERC or EIU Health Service at your earliest convenience. These forms include a Confidentiality Consent, Nutritional Analysis Form, and a 3-Day Food Record. Confidentiality Consent: This gives Eastern Illinois University and the Nutrition Education Coordinator or Registered Dietitian permission to perform the Nutritional Analysis. This form also gives us permission to send your analysis results to the Eastern Illinois University Health Service, Counseling Center and/or Eating Disorder Team depending on your results, while keeping your information confidential. Nutritional Analysis Form: This gives us some basic information about you, your nutrient intake, and physical activity patterns. This form will provide the Nutrition Education Coordinator or Dietitian with pertinent information needed to complete the analysis. This form also gives us information about any nutrition-related health conditions you may have. Based on the results, you may be referred to one of the EIU Health Service medical providers or Registered Dietitian. 3-Day Food Record: This form is included in the Nutritional Analysis Form and is used to assess your current nutrient intake and provides us with general information about your eating patterns. The more detailed your record is, the more accurate the analysis is. Please be very detailed when filling out the record. Be sure to include all measurements, condiments, cooking methods, and beverages consumed. At the end of each food log there is also a place to track your physical activity for the same days. I am excited about working with you and look forward to helping you achieve your nutrition goals! If you have any questions, feel free to contact the Nutrition Education Coordinator at 217-581-7786. Thanks, Caroline Weber Nutrition Education Coordinator Health Education Resource Center Phone: 217-581-7786 Fax: 217-581-8330 Email: herc-nutritioned@eiu.edu Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 To: Nutritional Analysis Participant From: Nutrition Education Coordinator Please make sure to sign and date this form and return it with the nutritional analysis packet to the HERC, EIU Health Service, or place it in campus mail in the envelope provided. This form must be filled out and returned in order to participate in the Nutritional Analysis Program. CONFIDENTIALITY CONSENT Nutritional Analysis Program Any information that is obtained in connection with the Nutritional Analysis Program and that can be identified with you will remain confidential. This packet will be given to the Nutrition Education Coordinator or the Registered Dietitian at the Health Education Resource Center. A copy of the results from the Nutritional Analysis will be added to your medical record at Eastern Illinois University Health Service. Depending on your analysis results, you may be referred to the Eastern Illinois University Counseling Center and/or Eastern Illinois University Eating Disorder Team. If you have any questions, please feel free to contact the Nutrition Education Coordinator at 217-581-7786 or herc-nutritioned@eiu.edu. I voluntarily agree to participate in the Nutritional Analysis Program. ________________________________________ Printed Name of Participant ________________________________________ Signature of Participant _________________________ Date I, the undersigned, have defined and fully explained the confidentially consent to the above participant. ________________________________________ Signature of Nutrition Education Coordinator Or Registered Dietitian ________________________ Date For Office Use Only ______________HS ______________CC ____________Other ____________________________________________________________________Provider/Counselor Copy To_____________________________________________________________________________ Nutritional Analysis 2 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Nutritional Analysis Form Please answer the following: Demographic Information ______________________________ PLEASE COMPLETE IN PEN ___________________________ __________ E Number Date Name ______________________________ _____________ __________ __________ Local Address Local Phone Date of Birth Age ______________________________ _____________ __________ __________ Height Gender EIU E-mail Address Current Weight Academic Information PLEASE COMPLETE IN PEN _________________________________ Major __________________________________________________ ___________ GPA Minor □ Freshman □ Sophomore □ Junior □ Senior □ Graduate □ Faculty/Staff □ Other 1. On average, how many hours per week do you spend studying? ________________________________ 2. As a result of any nutrition related health concerns have you: • Missed any classes within the past month? Circle One Yes / No ~If yes, how many? ________________ • Performed poorly on class related tasks? Yes / No • Failed an exam? Yes / No 3. Do you have any nutrition-related health conditions for which you would like to be referred to a Dietitian? (i.e.- diabetes, digestive disorders, etc.) If yes, please list: Yes / No Nutritional Analysis 3 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Nutritional Information PLEASE COMPLETE IN PEN 3. What is your reason for completing the Nutritional Analysis? __________________________________ _________________________________________________________________________________ _________________________________________________________________________________ 4. What nutritional goal(s) do you hope to reach as a result of the Nutritional Analysis? _________________________________________________________________________________ _________________________________________________________________________________ If your goal(s) include weight change, what is your desired body weight? _________________________ 5. Who prepares most of your meals? _____________________________________________________ 6. How many times per week do you eat out? Exclude Dining Halls. ______________________________ Circle One Yes / No 7. Are you a smoker? 8. Are you currently taking any prescription medications? Yes / No If so, please list and be specific: _______________________________________________________ _________________________________________________________________________________ 9. Are you currently taking any non-prescription medications (i.e. supplements, vitamins, etc.)? Yes / No If so, please list and be specific: _______________________________________________________ _________________________________________________________________________________ 10. Are you currently following any special diet(s)? Yes / No If so, please describe diet: ___________________________________________________________ _________________________________________________________________________________ 11. Do you follow a vegetarian diet? Yes / No 12. Do you feel your diet is nutritionally balanced? Yes / No 13. Do you normally eat breakfast? Yes / No 14. Who referred you for a nutrition analysis? Place an “X” in the box that applies. □ Physician □ Dietitian □ Professor/Instructor □ Self referral □ Counselor/Mental Health Professional □ Eating Disorder Team □ Other:______________ 15. Has anyone recommended you see a Dietitian or referred you to a Dietitian? If yes, Name: ______________ Title: ______________ Relationship: __________ Yes /No Nutritional Analysis 4 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Physical Activity PLEASE COMPLETE IN PEN 15. What is your current physical activity level? (Place an “X” in the box that best describes your daily activity level) Sedentary: o This activity level consists of the bare minimum; most time is spent at rest, lying down or sitting with minimal movement (i.e.; watching TV, reading, studying…). Lightly Active: o This activity level includes most office workers, professionals, and students; daily activities consist of approximately 8 hours of sleep and 16 hours awake, including 3 hours of light activity (i.e.; walking, house chores, cooking…) and 1 hour of moderately intense activity (i.e.; running, rollerblading, walking briskly…) Active: o This activity level includes most people who work in manual labor fields (i.e.; carpentry, construction, or building trades) and/or those people who average 1 ½ - 2 hours of moderate exercise 3 or more times per week (i.e.; elliptical machine, weight lifting, running…) Very Active: o This activity level includes most full-time athletes or others who are involved in very strenuous activity on a daily basis. 16. If you checked that you are either lightly, moderately, or very active, please describe what types of activities you engage in: ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ________________________________________________________ If you have any questions, feel free to contact the Nutrition Education Coordinator at 581-7786. Nutritional Analysis 5 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Food Intake Information: Part 1 PLEASE COMPLETE IN PEN Eating Attitudes Test Part A Current Weight: ________ Highest Weight (excluding pregnancy): _______ Lowest Adult Weight: _______ Ideal Weight: _______ Eating Attitudes Test Part B In the past 6 months have you: Once a Never month or less 2-3 Once times a a week month 2-6 times a week Once a day or more A Gone on eating binges where you feel that you may not be able to stop? B Ever made yourself sick (vomited) to control your weight or shape? C Ever used laxatives, diet pills or diuretics (water pills) to control your weight or shape? D Exercised more than 60 minutes a day to lose or control your weight? E Lost 20 pounds or more in the past 6 months Yes No EAT-26: Garner et al. 1982, Psychological Medicine, 12, 871-878. Adapted by D. Garner with permission. Nutritional Analysis 6 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Part C: Please check a response for each of the following statements: Always Usually Often Sometimes Rarely Never 1 I am terrified about being overweight. 2 I avoid eating when I am hungry. 3 I find myself preoccupied with food. I have gone on eating binges where I 4 feel that I may not be able to stop. 5 I cut my food into small pieces. I am aware of the calorie content of 6 foods that I eat. 7 I particularly avoid food with a high carbohydrate content (i.e. bread, rice, potatoes, etc.). I feel that others would prefer if I ate more. 8 9 I vomit after I have eaten. 10 I feel extremely guilty after eating. I am preoccupied with a desire to be 11 thinner. I think about burning up calories when I 12 exercise. 13 Other people think that I am too thin. I am preoccupied with the thought of 14 having fat on my body. I take longer than others to eat my 15 meals. 16 17 18 19 I avoid foods with sugar in them. I eat diet foods. I feel that food controls my life. I display self-control around food. 20 I feel that others pressure me to eat. 21 22 23 24 25 26 I give too much time and thought to food. I feel uncomfortable after eating sweets. I engage in dieting behavior. I like my stomach to be empty. I have the impulse to vomit after meals. I enjoy trying new rich foods. Nutritional Analysis 7 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 7 Ways to Size Up Your Servings 1 3 ounces of meat is about the size and thickness of a deck of playing cards. = 2 A medium apple or peach is about the size of a tennis ball. 3 1 ounce of cheese is about the size of 4 stacked dice. = = 4 ½ cup of ice cream is about the size of a tennis ball. 5 1 cup of vegetables is about the size of your fist. 6 7 = = 1 teaspoon of butter or peanut butter is about the size of the tip of your thumb. = 1 ounce of nuts or small candies equals the palm of your hand. = Nutritional Analysis 8 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Standard Serving Sizes **Below are the amounts that represent 1 serving from each food group** Dairy 1 cup (8oz) Milk 1 cup Yogurt (size of baseball) 1 cup Soy Milk 1 ½ ounces of cheese (two 9-volt batteries) Vegetables ½ cup cooked, chopped, or raw vegetables (small computer mouse) 1 cup raw, leafy greens ½ cup vegetable juice Fruit 1 medium piece (size of baseball) ½ cup 100% fruit juice ½ cup chopped fresh or canned fruit ½ grapefruit or large banana ¼ cantaloupe ¼ cup dried fruit or raisins Grains ½ bagel, hamburger bun, English muffin 1 cup cereal, cooked cereal (a baseball) ½ cup cooked pasta (size of palm of hand), cooked rice 1 slice of bread, tortilla shell, dinner roll Meat, Meat Alternatives, & Beans 1 ounce of meat (usually eat 2-3 ounces at a sitting or the size of a deck of cards) ½ cup cooked dry beans, peas, or lentils 1 ounce cheese (one 9-volt battery) 2 tablespoons of peanut butter (golf ball) 1 large egg 1/3 cup nuts or seeds Fat 1 teaspoon butter, mayonnaise, oil 1 tablespoon cream cheese, light whipping cream, half & half, regular salad dressing, reduced-fat mayonnaise 2 tablespoons reduced-fat salad dressing Nutritional Analysis 9 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 Food Intake Information: Part 2 PLEASE COMPLETE IN PEN Please write the number of servings of each food group you consume daily. Refer to 7 Ways to Size up Your Servings handout, Standard Serving Sizes handout, or contact the Nutrition Education Coordinator (581-7786) if you have questions about serving sizes for each food group. Food Group Grains Vegetables Fruit Dairy Meat, Meat Substitutes, & Beans Fats and Oils Convenience Foods Soda Pop & Sweetened Beverages Number of Servings Standard Residence Hall Serving Sizes Chili, soups, stews Rice, noodles, cooked cereal Egg, tuna salad Vegetables Macaroni and cheese Pancakes 1 cup ½ cup 1/3 cup ½ cup ¾ cup 2 Pasta dishes Meat Potatoes (mashed, au gratin) French fries Scrambled eggs 1 cup 3-4 ounces ¾ cup 15 fries 2 eggs Convenience foods are foods that are prepackaged such as chips and candy bars. There are not standard serving sizes for these foods. For these, indicate how many times a day you typically consume these types of foods. For soda pop and sweetened beverages, 12 ounces is a standard amount which is the size of a can of soda pop. Remember, most soda pops come in larger containers. For these, indicate how many times a day you typically consume these types of foods. Nutritional Analysis 10 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 REMINDER For 3-Day Food Intake Record, please record food intake for 2 weekdays and 1 weekend day (for example Sunday, Monday, and Tuesday). This is because eating patterns tend to change during the weekends. Also, please remember to record all beverage intake (including water) and amounts consumed, as well as any condiments and seasonings. Remember, the more accurate your record is, the more accurate your nutritional analysis results will be. Food Intake Information: Part 3 PLEASE COMPLETE IN PEN 3-Day Food Record In order to assist you in reaching your goals with respect to nutrient intake, it is important for us to know your current eating patterns. Please use the attached forms to provide a detailed record of everything you eat and/or drink over a three-day period. Try to record food and drink intake for Two Weekdays and One Weekend Day. If your meals or snacks are from a restaurant, please provide the restaurant’s name and a detailed description of what you ate in the Method of Preparation section. Feel free to attach any recipes, restaurant menus, or nutritional value handouts to this form. Be as specific as possible when listing food and drink items, amounts, and any additional ingredients (i.e. condiments, seasonings, or toppings). Do not try to change your eating habits during the days of record keeping. Refer to 7 Ways to Size up Your Servings for proper serving size information, or feel free to contact the Nutrition Education Coordinator (581-7786) if you have any questions. Daily Food Log Example: Meal Breakfast Food Item Oatmeal, instant apple cinnamon Amount 1 packet Method of Preparation Prepared with water, added 1 tsp of butter Activity Log Example: Type of Exercise Walking Intensity Moderate Duration 20 minutes Nutritional Analysis 11 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 DAY 1 The result of your 3-Day is only as accurate as your measurements. Date: _________________ Amount Food Item (cups, pieces, oz…) Method of Preparation Breakfast: Lunch: Dinner: Snacks: Type of Exercise Activity Log Intensity Duration If you have any questions, feel free to contact the Nutrition Education Coordinator at 581-7786. Nutritional Analysis 12 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 DAY 2 The result of your 3-Day is only as accurate as your measurements. Date: _______________ Amount Food Item (cups, pieces, oz…) Method of Preparation Breakfast: Lunch: Dinner: Snacks: Type of Exercise Activity Log Intensity Duration If you have any questions, feel free to contact the Nutrition Education Coordinator at 581-7786. Nutritional Analysis 13 Health Education Resource Center 5019 Student Services Building 600 Lincoln Ave. Charleston, IL 61920 (217) 581-7786 DAY 3 The result of your 3-Day is only as accurate as your measurements. Date: _______________ Amount Food Item (cups, pieces, oz…) Method of Preparation Breakfast: Lunch: Dinner: Snacks: Type of Exercise Activity Log Intensity Duration If you have any questions, feel free to contact the Nutrition Education Coordinator at 581-7786. Nutritional Analysis 14