FRACTURE NECK OF FEMUR
advertisement

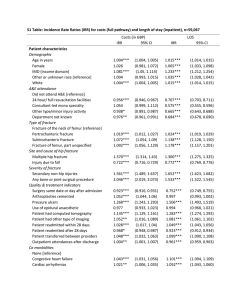
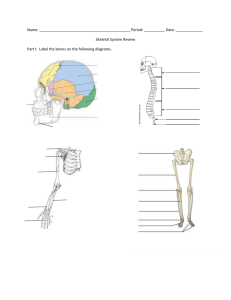
Fracture Neck Of Femur ANATOMICAL FEATURES OF FEMUR • The structure of the head and neck of femur is developed for the transmission of body weight efficiently, with minimum bone mass, by appropriate distribution of the bony trabeculae in the neck. • The tension trabeculae and compression trabeculae along with the strong calcar femorale on the medial cortex of the neck of the femur form an efficient system to withstand load bearing and torsion under normal stresses of locomotion and weight bearing. • In old age, osteoporosis of the region occurs. The incidence of fracture neck of femur is higher in old age. Blood Supply To Head & Neck Of Femur The profunda femoris artery arising from the femoral artery gives off medical circumflex femoral artery. This gives off the lateral epiphyseal and superior and inferior metaphyseal arteries. The lateral epiphyseal arteries are important and supply the laterial 2/3 of the femoral head. The superior metaphyseal artery supplies the superior aspect of the femoral neck. Blood Supply To Head & Neck Of Femur Blood Supply To Head & Neck Of Femur The inferior metaphyseal artery supplies the inferior part of the neck and the adjacent part of the head derived from the metaphysis. The medial epiphyseal artery supplies a circumfoveal sector of the head. It is a continuation of the artery of the ligamentum teres which arises from the acetabular branch of the obturator artery. Summary to Blood Supply to Head & Neck of Femur • The epiphysis and metaphysis receive their blood supply from • • • • • • separate sources. Epiphysial arteries named medial and lateral Metaphysial arteries named superior and inferior. The lateral Epiphysial and both Metaphysial arteries usually arise from the medial femoral circumflex artery. The medial Epiphysial is a continuation of the artery within the ligamentum teres which comes from the acetabular branch of the obturator artery. Lateral Epiphysial arteries predominate in the epiphysis & inferior Metaphysial arteries predominate in the Metaphysis. The artery of the ligamentum teres--a secondary blood source for the femur head-- supplies the medial third of the femoral head Blood Supply To Head & Neck Of Femur Blood Supply To Neck Of Femur Incidence & Mechanism The fracture of the neck of femur is common in the elderly. It does occur occasionally in young adults and even in children. It occurs more frequently in women. The fracture may result either from rotation violence at the hip due to tripping over something on the floor and falling or a direct violence over the lateral aspect of the hip by a fall on the side. Classification of Neck of Femur # (1) Intra capsular fractures (2) Extra capsular fractures. • Intra capsular Fractures from subcapital area to the middle of the neck. This is divided according to the level of the fracture line in the neck as follows. 1) Subcapital 2) Transcervical 3) Basal (at the junction of neck and shaft ) • Extra capsular Fractures from base of the neck to the pertrochanteric region.There are all grouped as Trochanteric fractures of various types. Gardens classification of fracture • This classification relies only upon the appearance of the hip on the AP radiograph. • It is used to determine the appropriate treatment. grade I : Incomplete fracture of the neck (so-called abducted or impacted) grade II : complete # without displacement grade III: complete # with partial displacement: grade IV : Complete femoral neck fracture with full displacement grade -1 grade -2 grade -3 grade -4 Clinical features • Pain • Restriction of movements of the affected hip • On examination : • Tenderness over the anterior hip joint line • Minimal shortening and external rotational deformity of the affected limb due to the fracture being intracapsular • Active straight leg raising is difficult • In impacted # complains : • Groin pain , restriction of hip movement Clinical Features • Inability to walk • The injured leg lies in a position of external rotation and there is shortening of the leg. • The attachment of the capsule to the distal fragment prevents excessive external rotation of the leg. • On palpation, there is tenderness over the anterior and lateral aspects of the hip joint. • The greater trochanter is elevated on the injured side. • All movements are extremely painful except in the rare case of an impacted type of fracture. Investigations X-ray: Anteroposterior (AP) and lateral view of the whole pelvis to show both the hips must be taken. It shows the level and the type of fracture. The subcapital and transcervical fractures are divided into three types according to the obliquity of the line of fracture (Pauwel). This is expressed as the angle formed by the line of the fracture with the horizontal line (Pauwel's angle). Investigations Pauwel's angle Type I: Pauwel's angle is less than 30 degrees (0-30), the fracture line is nearer the horizontal. Type II: The angle is between 30 and 70 degrees. Type III: The angle is more than 70 degrees and the fracture line is nearer the vertical. In the more vertical fractures, the action of the gluteal and adductor muscles produces a shearing force on the fracture line and hence nonunion is common. Thus, prognosis is worse in Type III and good in Type I Pauwels classification however refers to the angle the fracture line makes with the horizontal MANAGEMENT • CONSERVATIVE MANAGEMENT: • Fractures at this level have a poor capacity for union due to the following factors. a) Interference with the blood supply to the proximal fragment. b) Difficulty in controlling the small proximal fragment. c) The lack of organization of the fracture haematoma due to the presence of the synovial fluid. MANAGEMENT CONSERVATIVE MANAGEMENT: • In the very old patient with poor general condition, the only treatment possibly may be to keep the leg between sand bags and attend to the general care of the patient. • As soon as the general condition is restored and the local pain relieved, physiotherapy is started. • Movements of the hip are encouraged and the patient is got up on crutches about three weeks after the injury. Gradual weight bearing will lead to painless nonunion. This end result is practicable and is still useful in our country, in places where good surgical and hospital facilities are not available. Surgical Management • Two essential principles to be followed in the surgical management of this fracture are (a) perfect anatomical reduction. (b) rigid internal fixation. • The earlier method of stabilizing the fracture was by internal fixation with Smith Petersen Trifin nail. • The more recent method of internal fixation of the fracture is the use of multiple compression screws • Dynamic hip screws (DHS) • Total hip replacement (THR ) Dynamic hip screws Dynamic hip screw- DHS • Most commonly used device for both stable and unstable fracture patterns. • Plate angle is variable 130 to 150 degrees. • Has to be positioned centrally in the femoral head. • Use of radiological views to know the exact position. In older patients above 60 years, such fractures are treated by removing the head of the femur and replacing it by metal prosthesis like Austin Moore Joint replacement surgery • In older patients above 60 years, such fractures are treated by removing the head of the femur and replacing it by metal prosthesis like Austin Moore's prosthesis. • This enables the patient to be ambulant and start early weight bearing. Austin moore’s prosthesis Total Hip Replacement Complications of neck of femur fracture • The important complications are: • a) Non-union • b) Avascular necrosis of head of femur. • Non-union Failure of union of this fracture still occurs due to improper reduction of imperfect internal fixation. The patient complains of pain and develops instability on walking. The condition is treated by intertrochanteric osteotomy (McMurray) in the younger age group and replacement arthroplasty in the elderly. Complications of neck of femur fracture • Avascular Necrosis The patient presents with pain in the hip and limping. There is limitation of all movements of the hip with muscle spasm. Radiography shows patchy areas of increased density in the head of the femur. Treatment in the early stages is by rest, traction and weight relieving caliper. When indicated, osteotomy or replacement arthroplasty is done Extra capsular fracture These are also called low fractures and are classified as (i) Stable, (ii) Unstable fractures. In this group, the blood supply to the proximal fragment is not interfered with and there is a greater area of contact between the two fragments; hence the fractures unite easily. While union is the rule, it is common to see these fractures malunited with a coxa vara deformity. Clinical features The injured leg lies externally rotated and is obviously shorter. The degree of external rotation is greater than in the intra capsular fracture. There is marked local swelling. All movements of the hip are extremely painful and limited. Trochanteric Fracture Conservative Management • Skeletal Traction: In cases with marked coxa vara, continuous skeletal traction through the upper tibia is applied and the leg is immobilized in the Bohler Braun splint and the foot end of the bed is raised. Traction with 12 to 15 Ibs is sufficient. The coxa vara gets corrected and the fracture unites in about 12 weeks. • Skin Traction: When the coxa vara is not marked, skin traction in Thomas' splint will be sufficient. Bohler Braun splint Surgical Management • This consists of manipulative reduction and internal fixation. • The internal fixation is done by a nail plate • Compression hip screw and plate system has been used to enable earlier mobilization of the hip and weight bearing • If the Coxa vara is more, it can be corrected by Osteotomy. complications The main complications are Malunion Coxa vara o(It is common to see these fractures Malunited with a Coxa vara deformity) oThe normal neck shaft angle is about 115 degrees. When the angle is reduced to nearer 90 degrees, the deformity is called Coxa Vara Shortening.