Chapter 61 - shiftingparadigms
advertisement

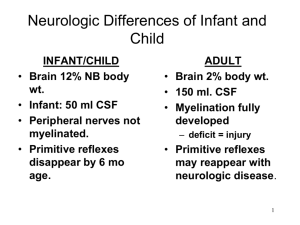
Chapter 61 Level of Concsiouness Headache Intercranial Pressure Seizure Level of Conscoiuness • Can be any spot on a spectrum from normal to coma • Full Conscoiuness would be orineted x’s 4 – Person, place, time, and sitution – Coma – Akinetic Mutism – Vegetative State – Locked-in Syndrome Level of Consciousness • PATHOPHYS – LOC is not a disease in an of itself but instead a symptom of another condition • Manifestations – Rememeber the GCS • Diagnostics – Full neurological assessment – Labs (cbc,cmp,NH3, LFT, Ca++, urine) – Test (MRI, EEG, CT) Increased Intracranial Pressure • Normal level is 0-15 • Monro- Kellie Hypothesis – the sum of volumes of brain, CSF, and intracranial blood is constant (Morki, 2001) – If one expands or decreases then the other need to compensate Morki, B. (2001). The Monro-Kellie Hypothesis. Neurology. 56(12). Pathophysiology of ^ ICP • Commonly associated with head trauma but also seen with tumors, metabolic acidosis, edema and herniation. • Decreased blood flow – Cell death +/- ischemia causes system pressure rises • This can produce a slow bounding pulse with respiratory irregulatories Pathophysiology • Cerebral Edema – Abnormal association of water and fluid in the intra and extra areas with an associated an increased volume of Hisse – Autoregulation occur as blood vessels constrict and diliate to keep the blood flow • Cerebral response to increase ICP – CPP= MAP-ICP – Normal CPP= 70-100 mmHg Cerebral response to ICP • Steady perfusion continues with ICP <40 & SBP 50-150 • CPP<50 = irreversible neuro damage • If CPP=ICP No cerebral circulation Ceberbral Response Cushing Response • Widening pulse pressure • Increased SBP • Decreased heart rate • Considered a late sign but still may be treated Cushing Triad • Decreased Heart Rate • Increased SBP • Decreased Respiration Clinical Manifestations • #1 sign of increased intercranail pressure is changes in LOC • Any sudden changes in the neuro status is significant • As ICP increases becomes stuporous, only reactioning to only loud painful stimulus Posturing Assessment of ICP • CT, SPECT, cerebral angiography • LP’s are contrindicated if the person is believed to have increased intracrainal pressure Seizure Disorder Abnormal motor sensory autonomic, or or pysch disorder Due to excessive discharge of neurons Can have 2 classifications partial(simple/complex) general SEE BOX ON PAGE 1881 Epilepsies • Known as a reoccuring seizure • May be primary or secondary • Pathophysiology – Neuron discharge by electrochemical energy to perfer a task – When they are supossed to stop they continue to firing the impluse which lead to a seizure Eplisies Clinincal Manifestations • Depends on what neurons are firing • Could be a small twitch that doesn’t stop or could include decrease level of consciousness Assess & Diagnosis • Detailed Health History • Family History • Physical and Neuro Status • MRI/EEG- localizes the area better; they may also need to do telemtry EEG • In the elderly epilpsey can present as an CVA • Status Epilipticus Headache • Most common neuro problem • May be primary but for unknown reasons • 3 types – Migrane – Tension – Cluster – Arteritis Pathophysiology • S&S of a migrane result from dysfunction of the brain stem pathways that modulate sensory input • Caused usually by vasodilation • May have many different triggers • Tension-usually associated with stress • Cluster-????? • Arteritis-migrane response when complex are deposits in the blood vessels walls Migrane manifestions Migrane Manifestation • • • • Prodrome Aura Headache Recovery Cluster • Unliateral small and frequent • May 1-8 x’s/day • Last 15 min- 3hr Tension • Constant steady pressure feeling state @ temple, front of head, or back of neck Arteritis • Very general start malise, fatigue, wt loss, fever, may swollen tender Assess & Diagnostics • Detailed history • Must be very detailed • Need to determine if the cause is something