Practice Theory
advertisement

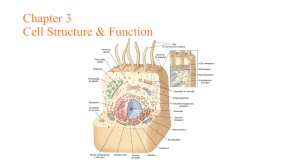
Clinical Social Work and Use of Practice Theories plus Models SOW6425 Clinical Assessment and Intervention Planning Professor Nan Van Den Bergh, PhD, LCSW Definition of Practice Theory • A coherent set of ideas about human nature, including concepts of : – Health and illness – Normalcy and deviance – The nature of change • Practice theory provides: – verifiable or established explanations for behavior – rationales for intervention. Types of Theories • Case theories: explain behavior of one client – What is your “theory” about the causes of a client's behavior? • Mid-range theories: explain a set of behaviors – Explanation as to why unemployed males can demonstrate domestic violence • Grand theories: explain human development, as well as “causes” and “cures” for maladaptive states, which can be generalized across populations – Freud’s theory of psychosexual development – Erickson’s “developmental crises” theory of human development – Piaget’s theory of cognitive development Practice Theory Functions • Simplifying complex phenomena into a focus on client’s thoughts, feelings and behaviors • Identifying our knowledge gaps about clinical situations • Explaining and predicting client cognitions and behavior • Bringing order to the selection of intervention targets and strategies • Bolstering professional self-discipline by protecting against irrational procedures • Promoting generalization among clients by cumulative practice knowledge • Mobilizing social energy to coordinate the work of other service providers • Enhancing our status within our agencies and among our peers Benefits of Theory Theory Focuses Attention • When the social worker “knows” what to do, assessment and intervention activities make better use of time and other therapeutic resources • Commitment to a body of thought “greater than oneself” bolsters professional self-discipline. • In “naive eclecticism” our choices for intervention might emerge outside of awareness and be influenced by irrational factors Theory Protects the Client • The worker can maintain a healthy distance from the client. • Without a theoretical base, “clinical skepticism may be subverted in the service of empathy”. Challenges of Using Theory • There is a potential harm of rigidly adhering to any practice theory. • Since theories simplify complex human behavior, they: • Are reductionist • Can be anti-humanistic • Create self-fulfilling prophecies by biasing perceptions of the client • Blind us to alternative understandings of behavior. THE RELATIONSHIP OF THEORY TO PRACTICE “Primary” Practice Theory (for Assessment) (Fits the practitioner’s assumptions about human nature) Practice Model (( A guiding strategies for working with certain types of clients) Practice Strategies (A guiding strategy for approaching a specific client) Interventions (The implementation of practice strategies; what we actually do to facilitate the change process) Relationship Between Theory and Intervention Strategies • Not every theory has unique intervention strategies – i.e. relaxation exercises or mindfulness practices could be use by both a behaviorist as well as an ego psychologist – Ego psychologist may see psychodynamics at root of addiction; but, use behavioral methods for changing selfdestructive behavior Theory and Practitioner’s “Practice Model” • Practice model: guiding strategy for working with certain types of clients – i.e. Begin with behavioral techniques to extinguish destructive and encourage constructive behavior – Then, undertake reflective interventions for insight development (person-situation reflection) • Practice Strategy is the individualization of a practice model” to a specific client’s personal and environmental characteristics – One client may be receptive to mindfulness practices whereas another is not Curative Factors in All Practice Interventions • Perception of practitioner, by client, as competent and caring – Therapeutic alliance • “Special setting” of seeking therapy promotes client’s sense of safety and expectation of help • Interventions and procedures are based on an rationale which is understandable(to the client), and theyn include an optimistic view of human nature. • Practitioner is “congruent” with client’s perception of problem and world view – Practitioner’s ongoing attention too client’s frame of reference • Client is given new opportunities for enhancing mastery Curative Factors in Practice (cont.) • Miller, Duncan and Hubble (2005): – Client characteristics associated with clinical outcome (account for 40% of outcome): • Nature of the problem • Motivation • Participation – Quality of therapeutic alliance (30%) – Guiding theory or model (15%) – Placebo effect (15%) Curative Factors in Practice (cont.) • Carkoff and Truax: Predictors to client retention in treatment: – Empathy – Congruence – Genuineness Practitioner’s Reasons for Theory Selection (both rational and irrational factors) • The theory’s research support • Belief that theory produces positive results (with the least expenditure of time and money) • It’s provision of useful intervention techniques • It’s consistent with practitioner's values, knowledge, skills and worldview • Personal habit • It’s use by co-workers or supervisor/s Selecting a Theory for Practice • A good theory for practice should be: – Coherent (internally consistent) – Useful with the practitioner's current clients – Comprehensive (applicable across a range of clients) – Parsimonious (uncomplicated to use) – Testable and able to withstand scrutiny (there are a variety of methods for doing this CLINICAL PRACTICE THEORIES • Focus on Reflection/Insight: Psychodynamic Theories • Ego Psychology (for individuals and groups) • Object Relations (for individuals and groups) • Self Psychology (for individuals and groups) • Family Emotional Systems: Bowen (can be applied to individuals and couples as well as families) CLINICAL PRACTICE THEORIES (cont.) • Focus on Conscious Thought / Observable Behavior • Cognitive Theory (for individuals and groups) • Behavioral Theory ((for individuals and groups) • Structural Family Theory: Minuchin CLINICAL PRACTICE THEORIES (cont.) • Focus on Relationship: – Relational Theory and Cultural Relational Theory – Interpersonal Therapy (a model) – Feminist Therapy (a model) – Afrocentric Therapy (a model) CLINICAL PRACTICE THEORIES (cont.) • Models and “Newer” Theories: – – – – Crisis Theory and Intervention Solution–focused therapy Narrative Theory and Therapy Motivational Interviewing