Expansion of Neurological Services through Partnerships with
advertisement

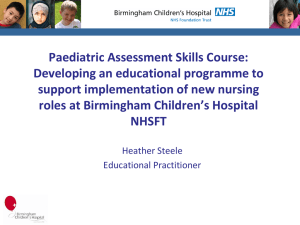
Expansion of Neurological Services through Partnership with Physician Assistants and Nurse Practitioners Carmel Armon, MD, MSc, MHS, FAAN, CPE. Baystate Medical Center /Tufts University School of Medicine, Springfield, MA, United States Introduction Figure 1. The Baystate Neurology Team, 2011 There are approximately 84,000 certified physician assistants and (PAs) [1] and 148,000 nurse practitioners (NPs) [2] practicing in the United States. Many are in primary care specialties, but they may be found in most practice settings. The training of PAs provides them with a broad foundation with a primary care focuses. PAs typically graduate a two-year postbaccalaureate program. Most PAs do not graduate with clinical experience beyond their rotations as students. In contrast, NP training requires an RN credential. Initially NP training was undertaken by RNs after several years of independent hands-on patient care experience. However, there are post-graduate programs leading to an RN and then NP qualification without intervening independent RN hands-on work. Different NP training tracks have emerged, including Pediatric, Family, Adult, Geriatric, Women's health, Neonatal, Acute, Occupational health [3], and graduates tend to practice in the track in which they have trained. While in general the training varies for PAs and for NPs, there is overlap in the material covered. One program offer shared courses to PAs and Family Nurse Practitioners [4]. PA or NP Graduates need to pass national certifying examinations in order to be licensed to practice. The laws in different states differ in regards to permitted practice settings and specific physician oversight requirements for PAs and NPs, and some insurance carriers also differentiate between PAs and NPs. An important consideration for a prospective employer of new PA or NP graduates is that their clinical readiness varies based on their pre-training career, the training track in which they were enrolled, their specific rotations during training, and individual factors. Neurologists are in severe shortage in Massachusetts [5], and recruitment of neurologists to western Massachusetts is particularly challenging. In 2003 I was recruited to expand the neurological services in Baystate Medical Center, the flagship hospital of Baystate Health, a 650-bed tertiary referral hospital in western Massachusetts, and a teaching hospital for Tufts University School of Medicine. Between 2003 and 2011, Baystate Neurology quadrupled the neurological services it provides to Baystate Medical Center and the residents of Springfield and western Massachusetts. The number of neurologist FTEs only doubled. This preferential growth in volume, in excess of increase in physician FTEs, was achieved through integration of physician assistants and nurse practitioners into the inpatient and outpatients neurology practices attaining a 1:1 MD to PA/NP ratio (Figures 1-2). This presentation will review the lessons learned from this experience, discuss the temporal trends over the past 8 years of integrating PAs and NPs into a neurology practice, and examine economic implications in fee-for-service settings and alternative models of care, such as accountable care organizations. Figure 2. Growth in Baystate Neurology Provider Numbers, Charges and RVUs: 2003-2011 Recruitment and Retention (cont’d) Seated L to R: Edith Zive; Lacy Florentino, Practice Manager; Kate Kogut NP; Molly Cahill-Kert NP Standing middle row, L to R: Philip Hsu MD; John Wojcik PA; Carol Zimmermann NP; Kayla Martin MA; Carmel Armon MD, Chief; Leigh Felton; Gladys Davis; Chandranni Quinones PA; May Yang MA; Maria Ferreira Standing back row, L to R: George Baquis MD; Elaine Reich RN; David Runge NP; Karen Lawson; Jeanne Smigiel; Jennifer Reardon; Ann Powers RN; Anant Shenoy MD; Ela Zlobicka DNP; William House MD; Sandra Godin [6] Recruitment and Retention Baystate Neurology recruits NPs and PAs fresh out of training, and individuals with previous work experience. We assume a minimal fund of neurological knowledge and no neurology experience. Our orientation program is summarized in the Table. Table. Orientation of New Baystate NPs and PAs 1. Pre-hire: Verbal overview of the scope of activities of the Neurology Division; shadowing in the relevant work settings (inpatient, outpatient); meeting with colleagues; and setting of expectations. 2. Immediately post-hire: The general Baystate orientation for all new employees. 3. On-the-job ramp-up, starting on the neurology inpatient consulting service. This is the principal neurology inpatient service at Baystate Medical Center. The inpatient setting lends itself to immediate neurologist oversight and feedback for all new patient evaluations and subsequent daily care decisions by the PAs and NPs. The ramp-up has quantitative and qualitative aspects. Initially, the workload is reduced to make sure that performance is safe and accurate. Once accuracy is established the workload is ramped up gradually till the work is shared equally among new and established PAs and NPs. Qualitatively, the most challenging task on the inpatient service is carrying the service beeper, triaging incoming calls. Assumption of this task is delayed till the team feels the new member is ready. Often, it is assigned first for half a day, with an established NP/PA available close by to support. 4. Lectures, some standard (such as the neurological exam), some given on a rotating basis to the medical students, and some ad-hoc, case-related. 5. For individuals who will have outpatient roles: their on-the-job orientation is facilitated in new patient intake clinics staffed jointly with neurologists and by an initially reduced follow-up work load, permitting greater opportunity to learn and ask about patients being seen. 6. There is an explicit expectation for ongoing independent learning, more so during the ramp-up phase, both as a time-of-care /point of care “look-itup” and as an after hours effort to read-up on at least one patient scenario daily. The neurologists model this behavior. 7. Participation in divisional didactic and administrative activities. Recognizing that different individuals have different learning styles, it is important for them to have a range of options, and for us to set the expectation that this is a joint responsibility. We have found that different individuals are inclined to be most comfortable in different aspects of neurological practice. We have permitted specialization, based on individual practitioner strengths and preferences and divisional needs, in inpatient care, outpatient care, and sleep medicine. Support in adjustment I discuss the challenges of adjustment explicitly with all new hires. I meet with them monthly, and work with them on a regular basis on the inpatient consulting service. I discuss that neurology inpatient work can be stressful in general, because we are inundated by never-ending waves of acute human suffering. This is harder for the novice to handle because of the mismatch between expectations and capabilities, and for most, the absence of training in how to cope with these circumstances. The milestones I put forth, in terms of attainment of levels of comfort, are 6 months, 12 months and 24 months. There is a clear expectation that the first 6 months will be challenging. The new hire can look for support from colleagues, and is expected to seek it. The more senior NPs and PAs keep their eyes open, as do I. “On-the-spot” interventions can be used to help individuals decompress. Temporal and Economic Trends Temporal trends in PA/NP acceptance When we expanded the use of PAs and NPs in our practice – they were not accepted universally by many of our stakeholders, including referring physicians and physician leaders. Many of the concerns were valid, including the objective fact that an NP or PA cannot fill in for a neurologist in terms of diagnosis of challenging cases and the range of capabilities of NPs and PAs ramping up. However, the benefits, in terms of expanding the reach of neurological services and provision of continuity care, outweighed the limitations. As NPs and PAs established themselves, their competency became recognized, and they were positioned to develop direct professional relationships with referring sources. However, as more MDs now want to work with PAs and NPs, the competition has become tougher to recruit PAs/NPs to neurology. Economic and non-economic implications – fee-for-service The chief economic implication of the team approach in the feefor-service setting is that it permits providing specialty cognitive services even as the reimbursement for them has been shrinking. The team approach permits neurologists and their PA/NP partners to concentrate their work in the upper range of their skill set.The PA or NP is shielded in part from the need to multitask among different constituencies, and may focus on one service area. This enhances provider engagement and patient satisfaction. Future models of care: Accountable Care Organizations Primary care physicians are increasing their reliance on PA and NP partners, who have little neurology focus in their training. This reliance is expected to grow as the shortage in primary care physicians continues and the eligibility to receive care grows. Where the goal is avoidance of hospitalization – access to outpatient specialty care will continue to be valued. The aging of the population and the increase in treatment options for most neurological diseases suggest that the need for readily available, affordable neurology care will increase. As long as PAs and NPs can contribute to patient care at a fraction of the hourly cost of a specialty MD -- models of neurological care incorporating PAs and NPs will continue to remain attractive. References Retention Our experience with retention has been mixed. While some individuals have joined us with a clear goal of making neurology their career, others have joined us with a more tentative agenda. By virtue of their training before joining us -- PAs and NPs have invested less in neurology than neurologists, and more options are available to them if they choose to leave. The statistic that 50% of physicians do not stay with their first job more than three years approximates the retention rate of our PA/NP population. We attempt to maximize our retention through attention to the ramp-up, which reflects our care for our co-worker, support of specialization, and fostering of team spirit. We are fortunate to have an excellent team of neurologists, NPs and PAs. 1. 2. 3. 4. 5. 6. National Commission on Certification of Physician Assistants. http://www.nccpa.net/Public.aspx. Accessed 3-18-2012. American Academy of Nurse Practitioners. http://www.aanp.org/AANPCMS2/AboutAANP Accessed 3-18-2012. Education Portal. Com. http://educationportal.com/nurse_practitioner_education_requirements.html Accessed 3-18-2012. UC Davis School of Medicine. Family Nurse Practitioner and Physician Assistant Program. Physician Workforce Study. Massachusetts Medical Society. October 2010. http://www.massmed.org/AM/Template.cfm?Section=Research_Reports_and_Stu dies2&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=36166. Accessed 3-18-2012. http://baystatehealth.com/Baystate/Main+Nav/About+Us/Locations/Baystate+Med ical+Practices/Specialty+Care/Neurology. Accessed 3-25-2012. www.postersession.com