Presentation - Families USA
advertisement

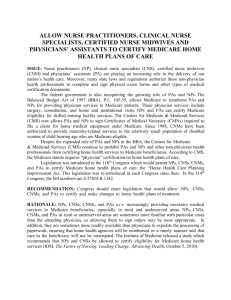
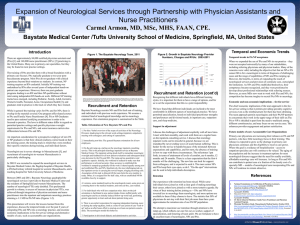
Addressing Provider Access Barriers in Communities of Color Opportunities and Challenges in the Affordable Care Act Nadia J. Siddiqui, MPH Senior Health Policy Analyst Texas Health Institute January 23, 2015 | Washington, D.C. | Families USA Health Action Conference Setting the Context Working to advance health equity is central to the ACA. Over 3 dozen provisions directly address health disparities, diversity, cultural/linguistic competence. Dozens of other general provisions that work to advance racial/ethnic health equity. 60+ Provisions on Advancing Health Equity Health Equity Provisions Cut Across 5 Primary Priorities: Health Insurance Health Care Safety Net Health Care Workforce - Culturally & linguistically appropriate marketing, outreach, and education - Medicaid/CHIP - Primary Care Provider Supply - NurseManaged Clinics - Loan & Scholarships for Underserved - Nondiscrimination - School Based Health Clinics - Pipeline Programs - Special provisions for American Indians - Community Health Needs Assessment - MinorityServing Institutions - DSH Payment Cuts - Cultural Competency Marketplace - Community Health Centers Public Health & Prevention Research, Quality & Innovation - Prevention & Public Health Fund - National Quality Strategy - CTGs - NIH/NIMHD - Obesity - CMS Innovation - Cancer - ACOs - Diabetes - Medical Homes - Oral Health - Agency OMHs - American Indian Health - Race/Ethnicity Data Standards - PCORI Overall Realization of ACA's Health Equity Provisions (56 Provisions) Last Updated: December 2013 Not Realized 23% More Fully Realized 48% Partially Realized 29% “Realization” measured in terms of the extent to which a provision received funding or was implemented through regulations, taskforces, or other activity. Source: Texas Health Institute, Research Last Updated December 2013. Funded by W.K. Kellogg Foundation Implementation Progress of ACA’s Health Equity Advancing Provisions by Topic (56 Provisions) Lasted Updated: December 2013 N = 19 6 N = 11 N = 10 6 1 9 Health Insurance Reforms 4 N=5 1 3 1 Access to Care & Safety Net More Fully Realized 1 4 3 7 Workforce Supply & Diversity N = 11 4 Research & Innovation Partially Realized 6 Public Health & Prevention Not Realized Source: Texas Health Institute, Research Last Updated December 2013. Funded by W.K. Kellogg Foundation Multi-Pronged Approach to Addressing Provider Shortages Provider Incentives • Financial support (e.g., loan repayment, scholarships) Systems Support • Advance practice professionals (e.g., NPs, PAs) • Interdisciplinary, team-based care models • Other: telemedicine, HIT, extended hours, transportation Community-Wide Initiatives • Pipeline education programs • Regional collaboration • Essential community providers & network adequacy Provider Incentives National Health Service Corps o Reauthorized by ACA through FY 2015, $1.5 Billion; FY 2015 budget invested an additional $3.9 Billion through FY 2020 Up to $50,000 in loan repayment and scholarships for health professionals who work 2 years in HPSA Students to Serve (S2S) Loan Repayment Program: $120,000 over 4 years to medical students in exchange for 3 years in underserved area Matching funds to states for loan repayment programs o Grown 3 times: 9,200 NHSC providers, serving 9.7 mil patients; One-third non-white providers Provider Incentives Other Incentivizing Strategies o Visa Waivers for Foreign Medical Graduates to serve in underserved communities o Partnering with community settings—e.g., health centers, clinics, and hospitals in rural or underserved areas—to serve as “rotation sites” for medical residents & providing stipends o e.g., Rural Physician Associate Program o Recruitment financial incentives – e.g., signing bonuses o Career development support and opportunities Systems Support Advanced Practice Professionals Systems Support Advanced Practice Professionals o ACA Support: PAs: $30 million for 700 new PAs by 2015 NPs: $31 million for 600 new NPs by 2015; $15 million for 10 nurse-managed health clinics to support training of 900 NPs and serve 94,000 patients State workforce development: $5.6 million to help states increase primary care workforce by 10-25% o HRSA estimates that projected increases in NPs and PAs between 2010-2020 could potentially reduce the expected shortage of primary care providers in 2020 by about two-thirds Systems Support Advanced Practice Professionals Primary care provided by NPs is “as safe and effective as care provided by doctors”1 NPs can provide up to 80% of care that primary care physicians currently provide 2 NPs/PAs are often more reflective of communities NCQA medical home recognition standards permit NPs and PAs to lead medical homes where allowed by state law NPs/PAs associated with smaller or rural community health centers as well as those with highest uninsured rate 3 NPs/PAs more involved with preventive patient education vs physicians who are more involved with complex care 3 1. 2. 3. IOM, The Future of Nursing: Leading Change, Advancing Health, 2010 Santoro & Speedling. Investing in the Future of Health Care Workforce. 2012 Leighton Ku et al, Community Health Centers Employ Diverse Staffing Patterns, Health Affairs, January 2015 Systems Support Embracing Interdisciplinary, Team-Based Care Physician led teams, supported by NPs/PAs, nurses, medical assistants, clerical staff, case managers, social and community health workers Team members performing “top of their license” Physician focus on complex cases; NPs/PAs providing majority of routine, primary, and preventive care Critical role of culturally competent health coaches or community health workers Health literacy Health insurance and systems navigation Addressing social, behavioral, and economic barriers Systems Support Other Systems-Level Facilitators Community-Wide Initiatives Building a Diverse, Health Professions Pipeline o Investment in “pipeline” from K-12 to postgraduate o Targeting traditionally underrepresented minority and economically disadvantaged students o Programs provide: Health career awareness Mentorship Scholarships Shadowing or training in community settings Community-Wide Initiatives Title VII Programs Reauthorized by the ACA o Physicians who graduate from a Title VII Program are 2-4 times more likely than other graduates to serve in an underserved area. o Scholarships for Disadvantaged Students Supports a large number of nurse practitioners 60% underrepresented minorities o Health Careers Opportunity Program Dramatic funding cuts, phased out in FY 2015 2012-13: 7,100 trainees (51% African American, 24% Hispanic) o Centers of Excellence Decline in funding over the years 2012-13: 7,600 trainees (43% Hispanic, 26% African American) Building Regional Collaborations o Partnerships between academic institutions and community-based clinics in urban, suburban, and rural settings to build the “pipeline” o Accountable Care Communities o e.g., UW Accountable Care Network - spans 46 cities and neighborhoods with 700+ primary care providers, 4,000 specialists, 573 clinics, 20 hospitals o e.g., Hennepin Health Social ACO - hospitals, clinics partnering with social service organizations to address broader social determinants that influence health care access and outcomes In Closing… o ACA creates a unique “Window of Opportunity” for expanding and building a diverse, culturally competent health professions workforce to address provider shortages. o BUT Authorized ≠ Appropriated! o Limited funding for many programs, along with active and passive resistance to the law threaten to deflect resources and delay or diminish the law’s vision and potential. Points to Consider Moving Forward Reassessing “Scope of Practice” laws for advanced practice professionals and identify room for flexibility & innovation Advocating for and assuring support for the health professions pipeline, especially targeting students from diverse racial, ethnic, and socioeconomic backgrounds Looking to collaborative solutions that encourage clinical-academic-community partnerships across urban, suburban, and rural settings Building on the ACA’s support to address provider shortages through team-based, medical home, telemedicine, accountable care, and other systems innovations Thank You! Nadia J. Siddiqui, MPH Senior Health Policy Analyst Texas Health Institute nsiddiqui@texashealthinstitute.org http://www.texashealthinstitute.org/health-care-reform.html Texas Health Institute’s ACA & Health Equity Team: Dennis Andrulis, PhD, MPH, Senior Research Scientist Maria Cooper, MS, Health Policy Analyst Lauren Jahnke, MPAff, Health Policy Consultant Anna Schellhase, Graduate Health Policy Intern Nadia Siddiqui, MPH, Senior Health Policy Analyst