South London and Maudsley (SLaM)
IAPT-SMI Demonstration Site for Psychosis
Professor Philippa Garety
Clinical Director, Psychosis Clinical Academic Group
Thursday 7 March 2013
Service users want equal
access to psychological
therapies
Rethink survey (2010)
Research suggests that
only 1 in 10 access CBT,
despite NICE guidance
(Schizophrenia Commission,
2012)
The Abandoned Illness
The Schizophrenia Commission
“Research has led to a range of evidence-based
psychological treatments. We know much more about
‘what works’ than we used to. . . The committed
individuals who went into the mental health profession
to improve lives should be helped to do exactly that.”
Prof Sir Robin Murray
This is where IAPT-SMI comes in
Obstacles to access
Dolly Sen, Service User Consultant
“I always asked for some kind of psychological therapy
or talking therapy but was told, no, it was too
dangerous. I had to wait 20 years for something that
was the most beneficial thing. [Therapy] has changed
my life basically.”
Talking to Norman Lamb on 19 December 2012
69% of Trusts have funding
challenges for providing
access to psychological
therapies for people with a
diagnosis of schizophrenia
94% have encountered
obstacles in making
psychological therapies
available, including
insufficient skilled staff
Delays in accessing CBTp
Peters et al 2009
(N=74)
• Mean length of illness was 8 years (range 0-32)
• Mean of 2.8 in-patient admissions (range 0-20)
• 96% were on antipsychotic medication
South London and Maudlsey NHS
Foundation Trust: the context
• Core population - 4 South
London Boroughs
1.3million; inner city, very
high indices of social
deprivation
• Substantially raised rates of
psychosis
• Psychosis Care Pathways
SLaM Psychosis Demonstration site:
Increasing access in two care pathways
IAPT-EI
Early Intervention Pathway
(Southwark, Lambeth, Croydon & Lewisham)
IAPTPICuP
IAPTSHARP
Promoting Recovery Pathway
(Lambeth)
Promoting Recovery Pathway
(Southwark, Croydon & Lewisham)
SHARP
What IAPT-SMI offers for service users
CBT for psychosis:
• weekly or fortnightly individual 1 hour sessions
• 6-9 months therapy
• Therapists receive weekly-fortnightly group
supervision
FI for psychosis:
•
•
•
•
Fortnightly 1 hour sessions with client and carer(s)
Up to ten sessions, over a period of 3-9 months
Therapy delivered by two trained therapists
Therapists receive weekly-fortnightly group
supervision
Overcoming obstacles to access
Work we have already done in SLaM
• Ten point charter addressing
barriers and facilitators:
– Service user involvement
– Quality criteria and staff
training
– Data gathering, data
systems and outcomes
– Care pathways, ensuring
integrated effective care in
Early Intervention &
Recovery pathways
Psychological treatments are
not a quasi - medication
=
Quality
• One key challenge has been a lack of clarity about quality –
psychological therapy is different from a chemical compound
• Lack of criteria have resulted in an ‘anything goes’ approach to
psychological therapy in MH services, and inflated estimates of
provision
• We need nationally agreed criteria for training and
competencies in CBTp and FI
• IAPT-SMI is doing this
• Locally we have already developed criteria and standards and
established a portfolio of training opportunities
Training and Supervision
Training and Supervision
• Portfolio of training opportunities in psychological
therapies for psychosis, in partnership with KCL
• Span the workforce from non-clinical to
managerial/supervisory
• Academically accredited training and in-service courses
• Short courses and modules build to an award
• Supervised practice strongly emphasised
• Supervision and support for supervisors
Training structure in the SLaM site
Service user and caregiver
involvement & co-production
•
Involvement in development, design and evaluation of
psychological therapy services
•
Training design and delivery
•
Co-produced workshops at SHARP and in the SLaM Recovery
college
•
Co-working in group interventions: Hearing Voices; Mindfulness;
Acceptance & Commitment Therapy
•
Training, supervision and support (practical, financial and
emotional)
•
Personal development – CPD, co-authorship, conference
attendance
SLaM demonstration site strategic
approach to improving access to therapy
• A 50% increase in access with the funding provided
• Reduced waiting times
• Implementation of our 10 Point Charter, with highly
trained staff, and care pathways
• Clear referral pathways, including self referral
• Regular assessment of progress in therapy
• Close and frequent supervision
• Assessing improvement in a range of outcomes and
in health economics
Effectiveness
Clinical outcomes:
Service-user reported symptoms
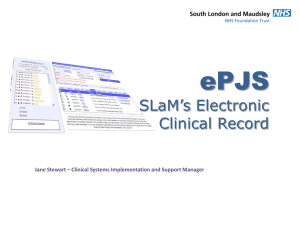
Evidence of clinical outcomes with
medium-large effect sizes
– voices and delusions
89% (voices) & 90% (delusions) have paired data at end of therapy
30
16
Voices
Delusions
25
Voices
12
10
20
Delusions
14
8
15
6
Assessment (N=96,
125)
Before therapy (N=70, End of therapy (N=85,
80)
113)
This graph shows a reduction in psychotic symptoms
[voices (effect size: .73) and delusions (effect size: .59)]
following therapy (PICuP)
Evidence of clinical outcomes with mediumlarge effect sizes – anxiety and depression
85% have paired data at end of therapy
24
26
22
22
20
20
18
Anxiety
Depression
24
Depression
Anxiety
18
16
16
14
14
Assessment (N=176) Before therapy (118) End of therapy (148,
152)
This graph shows a reduction in emotional problems
[anxiety (effect size: .47) and depression (effect size: .55)]
following therapy PICuP
Evidence of clinical outcomes with mediumlarge effect sizes – quality of life (QoL) and
recovery
85% (QoL) & 67% (CHOICE) have paired data at end of therapy
54
140
130
52
50
110
48
CHOICE
MANSA
120
QoL
Recovery
100
46
90
44
80
Before therapy (174; 113)
End of therapy (131, 76)
This graph shows an increase in people’s quality of life (measured on the
Manchester Short Assessment of Quality of Life; effect size: .51) and
recovery ratings (measured on the CHOICE; effect size .79)
following therapy
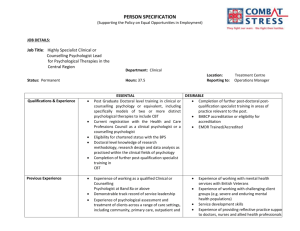
Cost-effectiveness
Mean 9-month cost (2005/6 £s)
Randomised Controlled Trial (Peters et al, 2010) – therapy costs are
off-set by fewer inpatient costs at 3 months follow-up
Therapy
Inpatient care
Non-inpatient care
14000
£12,558
12000
(N = 74)
10000
£9018
8000
£6602
£7236
6000
4000
2000
0
Therapy
(baseline)
Control
(baseline)
Therapy
(follow-up)
Control
(follow-up)
Reduction in service-use costs (admissions & home treatment
team days) in the year following therapy, compared to the year
prior to therapy (Wilcoxon test: p <.05*)
Costs per month (£)
500
451.46
Data obtained from
ePJS, Jan 2012
400
N = 70
300
172.24
200
100
0
1 year prior to therapy
1 year following therapy
Progress and preliminary outcomes
New clients - demographics
Variable
New clients in the service
Age distribution
Mean 38 years (18-70)
Gender
43% male, 57% female
Ethnicity
36% white, 64% BME
Demonstration site CBTp & FIp
referral targets are being achieved
Existing
Projection
Monthly
Referral Target
(over 12m)
Progress at
4 months
CBT
FI
CBT
FI
CBT
FI
CBT
FI
106
15
50
10
14
2-3
95
11
Waiting times are reduced (in days)
Referral
received to
opted-in
Opted-in
to
assessed
Assessed
to
receiving
therapy
35
7
23
Total
57
%
reduction
in waiting
times
60%
Health Utilisation data
Service
Mental health admission
Mean number of days
in 12m before therapy
10.5 (0-126)
Crisis team / home treatment
0.7 (0-23)
Psychiatric liaison (A&E)
0.1 (0-2)
IAPT-SMI: CBT assessments
Pre
3-monthly
Post
PSYRATS – Voices
& Beliefs
PSYRATS – Voices
& Beliefs
PSYRATS – Voices
& Beliefs
WEMWBS
WEMWBS
WEMWBS
WSAS
WSAS
WSAS
EQ-5D
EQ-5D
EQ-5D
Short CHOICE
Short CHOICE
Short CHOICE
CORE-10
CORE-10
CORE-10
Brief IPQ
Brief IPQ
Brief IPQ
Measures Feedback
Measures Feedback
Measures Feedback
Satisfaction with
therapy
Satisfaction with
therapy
Short CHOICE weekly
IAPT-SMI: Carer assessments
Pre
3-monthly
Post
Experience of
caregiving inventory
Experience of
caregiving inventory
Experience of
caregiving inventory
WEMWBS
WEMWBS
WEMWBS
DASS-21
DASS-21
DASS-21
CORE-10
CORE-10
CORE-10
IPQ carer version
IPQ carer version
IPQ carer version
Confidant question
Confidant question
Confidant question
Measures Feedback
Measures Feedback
Measures Feedback
Satisfaction with
therapy
Satisfaction with
therapy
Patient Reported Outcome Measures
Measure
Session by session
short CHOICE
Pre-therapy:
PSYRATS
Questionnaires
Completion rate
81% of attended
sessions
98%
100%
London Tonight report from 19 December 2012 –
visit to SLaM by Norman Lamb, Care and Support
Minister and the official launch of the IAPT-SMI
demonstration sites:
http://www.itv.com/news/london/update/2012-1220/maudsley-hospital-pioneers-mental-healththerapy-scheme/
Operational Group
Dr Louise Johns,
Project Lead
Dr Miriam Fornells-Ambrojo,
IAPT-EI Lead
Dr Suzanne Jolley,
Lambeth Recovery
Psychology Lead
Rosanna Michalczuk
Bina Sharma
Psychology Assistants
Dr Craig Milosh, Clinical
Psychologist, SHARP
Devon Elliott, Business
Intelligence Analyst
Dr Juliana Onwumere, FI Lead
Steering Group
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Lucy Canning, Psychosis CAG Service Director
Prof Philippa Garety, Psychosis CAG Clinical Director
Jonathan Beder, Psychosis CAG Deputy Director, Business and Performance
Dolly Sen and Garry Ellison, Service User consultants
Roger Oliver and Lorna Wilkinson, Carer consultants
Prof Tom Craig, Consultant Psychiatrist, SHARP
Marieke Wrigley, Team Leader, SHARP
Prof Elizabeth Kuipers, NICE Schizophrenia guideline lead
Dr Emmanuelle Peters, PICuP Director
Adrian Webster, CAG Psychological Therapies Lead
Jo Lawrence, Clinical Service Lead, EI
Dr Sarah Dilks, Lead Psychologist, Promoting Recovery pathway
Dr Eric Morris, Lead Psychologist, Early Intervention pathway
Penelope Fell, Head of Business Development
Dorothy Abrahams, Administrator
Thank you for listening!
You are welcome to our SLaM
Demonstration Site Visit
Monday 1 July 2013
1.00-5.00 pm
Louise.johns@slam.nhs.uk
 0
0