State of the Division - Department of Family and Community Medicine

DPC Grand Rounds June 14, 2012
STATE OF THE DIVISION:
An Update on the past, present & future of the DIVISION OF PALLIATIVE CARE
Jeff Myers MD, CCFP, MSEd
W. Gifford-Jones Professorship in Pain and Palliative Care
Head and Associate Professor - Division of Palliative Care,
Department of Family and Community Medicine
Faculty of Medicine, University of Toronto
DIVISION OF PALLIATIVE CARE
Who are we?
What does being a DPC Member mean?
What do we do?
Why do we matter?
Where are we going?
How will we get there?
What can each of us do?
DPC: WHO ARE WE?
“ The core purpose of the DPC is to create and support a community of learners, teachers, innovators, researchers and practitioners working together to improve the quality of palliative and end of life care for patients and their families.
”
DPC Strategic Plan, 2009
DPC: WHO ARE WE?
The values serving to guide all DPC activities are:
Interprofessionalism
Community
Innovation
Advocacy
DPC Strategic Plan, 2009
DPC: WHO ARE WE?
The largest academic palliative care division in Canada!!!
DPC: WHO ARE WE?
2002: Residency Program
2007: Formal status as an academic Division
(Head, Dr. Larry Librach, 2007-11)
2009: Inaugural Strategic Plan: Long Term Vision
Every health care professional trained through the U of T will be able to demonstrate basic competencies in the provision of quality palliative and EOL care
DPC will be a leader in developing, measuring and teaching advanced competencies in palliative care in Canada
DPC: WHO ARE WE?
Long Term Vision
A robust and collaborative research program will be credited with discoveries that challenge current best practice in care provision and education and explore innovative interventions that improve the quality of palliative and EOL care
Professionals seeking a location for clinical practice, research and/or education in palliative care within an expansive, dynamic environment will choose Toronto and the DFCM ’ s DPC
DPC: ORG STRUCTURE
DPC: COMMITTEE LEADS
CPD Lead: Monica Branigan
RPD: Giovanna Sirianni
Interim RPD: James Downar
Education Co-Leads: Anita Chakraborty &
Monica Branigan
Research Co-Leads: Amna Husain &
Paolo Mazzotta
Admin Lead: Heather Huckfield
DPC: PROFESSION / DISCIPLINE LEADS
Social Work: Susan Blacker
Nursing: Sharon Reynolds
Pediatrics: Adam Rapaport
DPC: SITE REPS
Baycrest: Daphna Grossman
CVH: Manisha Sharma
Markham Stouffville: Gina Yip
Mt Sinai: Russell Goldman
NYGH: Niren Shetty
PMH: Julia Ridley
Scarborough: Larry Zoberman
SickKids: Adam Rapaport
DPC: SITE REPS
Southlake: Cindy So
St. Joseph ’ s: Carol Hughes
St. Michael ’ s: Ignazio LaDelfa
Sunnybrook: Dori Seccareccia
TEGH: Kevin Workentin
TGH/TWH: Sharon Reynolds
Trillium: Tony Hung
DPC: MEMBERS
Membership Assembly
Current composition:
Over 60 Faculty Members
Over 60 Associate Members
DPC: WHAT DOES BEING A
MEMBER MEAN?
FACULTY MEMBERS
Clinicians who have pursued and achieved a U of T faculty appointment
Available to all professionals who are members of a U of T affiliated institution and actively involved in palliative care and teaching, education, research, creative professional activity and/or leadership
DPC: WHAT DOES BEING A
MEMBER MEAN?
ASSOCIATE MEMBERS
Clinicians without a formal clinical or faculty appointment with the U of T who have an interest and/or a clinical practice involving palliative care
DPC MEMBERSHIP: WHY?
• Participate in DPC related activities, initiatives and committees (eg. PD, teaching/education, research, clinical, operations, administrative, social networking)
• Contribute to building a sense of academic community
• Be informed about DPC related activities and initiatives
• Connect/collaborate with colleagues across the DPC
• Cultivate a profession specific community
• Gain exposure to and develop skills related to professional and/or academic activities
• Collaborate on profession specific projects/initiatives
• Opportunities to explore formal and informal mentorship
DIVISION OF PALLIATIVE CARE
WHAT DO WE DO?
DPC: WHAT DO WE DO?
We Educate
95% of DPC Members are involved in teaching and education activities
DPC: WHAT DO WE DO?
Undergraduate Medicine
Pre-clerkship:
“ Pain Week ” ; MMMD course
“ Approaching End Of Life ” ; ASCM
Clerkship:
Anesthesia, General Surgery, Family
Medicine, Transition to Residency, FMLE
DPC: WHAT DO WE DO?
Postgraduate Medicine
DPC: WHAT DO WE DO?
Postgraduate Medicine: Enhanced Skills
• Clinical Palliative Care Enhanced Skills Program
St. Joseph ’ s Health Centre Site
12 graduates since 2005
North York General Hospital Site*
• Conjoint Palliative Medicine Residency Program
*Recently implemented
CONJOINT RESIDENCY PROGRAM
Annual Growth in # of Positions and Applicants
CONJOINT RESIDENCY PROGRAM:
GRADUATES
DPC: WHAT DO WE DO?
CE & PD
DPC: WHAT DO WE DO?
We Educate - Innovations
• Centre for IPE - Case Based Session
• PGCoreEd
• Social Work Interest Group - Susan Blacker
• National Learner Assessment Collaborative
• CVH/Trillium - collaboration with FHT (LEAP)
• Collaboration with Cicely Saunders Institute:
Medical Student Exchange Fellowship
(Dr. Robert Buckman)
DPC: WHAT DO WE DO?
We Discover
Over 50 publications in last five years
Dr. Amna Husain PI for
CIHR Grant: Ranked #1
DPC: WHAT DO WE DO?
A few examples…
DPC: WHAT DO WE DO?
A few examples…
DPC: WHAT DO WE DO?
We Are Acknowledged
2011 Undergraduate New Teacher Award: Dr. Jean Hudson
2010 Helen P. Batty Award: Dr. James Meuser
2010 DFCM Awards of Excellence: Dr. Monica Branigan
2010 PD Program Excellence Award: Dr. Kevin Workentin
2010 PD Program: Dr. Pauline Abrahams
2009 John W. Bradley Educational Admin: Dr. Dori Seccareccia
2009 Postgraduate Education Program: Dr. Leah Steinberg
A few examples…
DPC: WHAT DO WE DO?
We Are Acknowledged
Senior Promotion to the Rank of Associate Professor:
2012: Dr. Albert Kirsen & Dr. Vince Maida
2011: Dr. Monica Branigan, Dr. Amna Husain & Dr. Jeff Myers
2010: Dr. Jamie Meuser
A few examples…
DIVISION OF PALLIATIVE CARE
WHY DO WE MATTER?
DPC: WHY DO WE MATTER?
The MOH says so…
DPC: WHY DO WE MATTER?
The care we provide makes a difference…
DPC: WHY DO WE MATTER?
We are catching on in other settings…
DPC: WHY DO WE MATTER?
Conclusions:
“ Our prospective study shows that dementia is a terminal illness and furthers our knowledge of the clinical complications characterizing its final stage.
”
This was the first time this statement was made
We are catching on in other settings…
DPC: WHY DO WE MATTER?
CLINICAL COURSE – DEMENTIA
LETTER TO THE EDITOR
“Classifying all seniors affected by advanced dementia as terminally ill … can become a gateway to therapeutic neglect ."
We are catching on in other settings…and familiar challenges lie ahead
DPC: WHY DO WE MATTER?
A request was recently made of me to speak to the topic:
“ How to initiate and have end-of-life discussions in the office for patients with palliative conditions?
“
DPC: WHY DO WE MATTER?
A request was recently made of me to speak to the topic:
“ How to initiate and have end-of-life
discussions in the office for patients with palliative conditions?
“
How might this be more precisely worded?
DPC: WHY DO WE MATTER?
A request was recently made of me to speak to the topic:
“ How to initiate and have goals of care
discussions in the office for patients with advanced and/or incurable “
DPC: WHY DO WE MATTER?
A request was recently made of me to speak to the topic:
“ How to initiate and have goals of care
discussions in the office for patients with advanced and/or incurable “
Propose this to be a primary solution to effectively addressing the “ tsunami of chronic disease ”
40
20
0
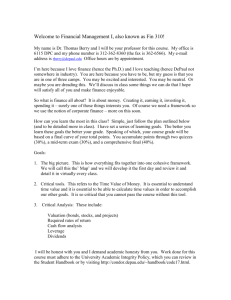
Actual and Projected Deaths in Ontario: 1996-2036
160
140
120
100
80 80 80 80 81 81 81
83 84 85 84
86
89
92 94
96 98
100 102
104 106
108 110
112 114
116 118
120 122
124
127
129
131
134
137
140
143
145
152
148
Total Number of Deaths projected to increase:
By 20% in 10 years from 2010-11 to 2020-21.
60
WE ARE HERE!!!
DIVISION OF PALLIATIVE CARE
WHERE ARE WE GOING?
DPC: WHERE ARE WE GOING?
SUB-SPECIALTY STATUS
• Currently, the RCPSC application process for formal recognition of Palliative Medicine as a
Sub-Specialty is in Stage 2 (Consultation Phase)
• New two-year medical training program
• Routes of entry are IM, Neuro, Anesth for
Adults stream and Peds
• Uncertain what the current one-year program will evolve in to as per CFPC
DPC: WHERE ARE WE GOING?
• If/when a Sub-Specialty is formally created, the route of “practice eligibility” will likely be made available to physicians who have both completed the current one-year program and entered from a
RCPSC specialty as well as current RCPSC members who maintain a clinical practice focused in Palliative Medicine
• Discussions at the CFPC are currently underway to determine if a certification and/or designation process will be instituted for the one-year program
DPC: WHERE ARE WE GOING?
• Based on what is determined, a practice eligible route is likely to be made available to current
CFPC members who maintain a clinical practice focused in Palliative Medicine (with or without having completed the one-year training program)
• Family physicians who do not hold certification can acquire certification until December 31, 2012 via
“Alternate Route to Certification” - see cfpc.ca
DPC: WHERE ARE WE GOING?
Curative / Remissive Therapy
CG Support &
Bereavement
Presentation
Hospice & Palliative Care EOL Care
Model of Collaborative or Shared Care
Death
DPC: WHERE ARE WE GOING?
Curative / Remissive Therapy
CG Support &
Bereavement
Presentation Death
Hospice & Palliative Care EOL Care
Model of Collaborative or Shared Care
Its time to move beyond this
Pt E
Pt D
Pt C
Pt B
Pt A
LEVELS OF PALLIATIVE CARE
Complex palliative care-related needs
Basic palliative care-related needs
Most will have needs requiring only basic PC skills (Pt A )
Others will occasionally require specialty level PC
(Pts B , D )
A small number with highly complex needs will indefinitely require specialty level PC
(Pts C , E )
Illness trajectory EOL
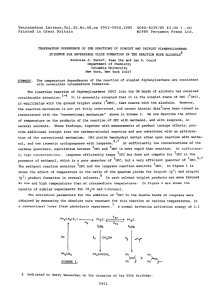
PROVISION OF PALLIATIVE CARE
Academic
Mandate
Patient
Volumes Patient Needs
• Complex needs unresponsive to basic care or established protocols;
• Require highly individualized care plans
• PC needs exceed those available from primary care;
• Pt/families ability to cope is compromised
• Largest group of patients;
• Most needs met through primary care providers (i.e. non-PC specialists
Expertise
Tertiary
Level
Secondary
Level
PC Expertise
Primary Level
PC Expertise
Description of
Provider Role
• Experts in PC; consults to secondary and primary level providers; Leaders in
PC research & education
Care
Setting
• All care settings require at least access to tertiary level expertise generally hospital based
• Extensive PC knowledge in PC; model of care may be consult only to direct care; most often share care with primary team
• Basic or primary level PC related clinical skills (pain and Sx Mx; basic psycho-social care)
• Required in all care settings
(home, acute care, LTC, CCC ambulatory clinics)
• All care settings
PROVISION OF PALLIATIVE CARE
Academic
Mandate
Patient
Volumes Patient Needs
• Complex needs unresponsive to basic care or established protocols;
• Require highly individualized care plans
• PC needs exceed those available from primary care;
• Pt/families ability to cope is compromised
• Largest group of patients;
• Most needs met through primary care providers (i.e. non-PC specialists
Expertise
Tertiary
Level
Secondary
Level
PC Expertise
Primary Level
PC Expertise
Description of
Provider Role
• Experts in PC; consults to secondary and primary level providers; Leaders in
PC research & education
Care
Setting
• All care settings require at least access to tertiary level expertise generally hospital based
• Extensive PC knowledge in PC; model of care may be consult only to direct care; most often share care with primary team
• Basic or primary level PC related clinical skills (pain and Sx Mx; basic psycho-social care)
• Required in all care settings
(home, acute care, LTC, CCC ambulatory clinics)
• All care settings
DIVISION OF PALLIATIVE CARE
WHERE ARE WE GOING AND
HOW WILL WE GET THERE?
OUR initial strategy will be to
BUILD CAPACITY
DPC: HOW WILL WE GET THERE?
DPC: HOW WILL WE GET THERE?
It should not be advocacy for earlier integration of the PC field in the illness trajectory…
It should be advocacy for earlier integration of both PC philosophy and PC-related clinical skills
DPC: HOW WILL WE GET THERE?
If oncology has just recently integrated palliative care-related clinical skills in to their training programs, what about every other illness known to be incurable and the IP teams who care for them?
…CHF, COPD, Dementia, ND, CKD, cirrhosis, metabolic disorders…
40
20
0
Actual and Projected Deaths in Ontario: 1996-2036
160
140
120
100
80 80 80 80 81 81 81
83 84 85 84
86
89
92 94
96 98
100 102
104 106
108 110
112 114
116 118
120 122
124
127
129
131
134
137
140
143
145
152
148
Total Number of Deaths projected to increase:
By 20% in 10 years from 2010-11 to 2020-21.
60
WE ARE HERE!!!
DPC: HOW WILL WE GET THERE?
HOW WILL WE BUILD CAPACITY?
INTEGRATION
EDUCATION
COMMUNITY BUILDING
DPC: INTEGRATION
•
BEGIN WITH DFCM
• DPC Head: Site Visits
• Faculty Appointments: Collaborative
Model with Site Chiefs
“ DPC: A Resource for DFCM Faculty ”
•
Next four slides outlines possible elements
“ DFCM Site Integration Tool Kit ”
DPC: INTEGRATION
DFCM Site Integration Tool Kit
• Examples of possible standard presentations
•
•
• “
The DPC As A Resource to the DFCM: How to
Have a Discussion with the DFCM Chief
”
“
Strategies for Teaching Your Family Medicine
Colleagues
”
“
The Palliative Care You
’ re Providing But May Not
Know It: Building Capacity Among Family MDs
”
• As well, presentations on topics from brochure
DPC: EDUCATION
Repository of resources:
• Resources for community building through collaborations and sharing
• Resources for Learners
• Resources for Teachers undergrad, postgrad, IPE, CE, other prof
• Resources for Researchers
• Resources for Leaders
• Patient and Family Education Resources
DPC: COMMUNITY BUILDING
• DPC Face to Face Event - Sept/Oct 2012
• DPC New Member Orientation
• DPC FAQs (What, Who, Where, Why, How)
• Value-add vehicle supporting collaboration
DPC:
WHAT CAN EACH OF US DO?
THIS IS A CALL TO ACTION
Each of us MUST consider ourselves an essential resource
Every professional interaction
MUST have two components:
CLINICAL
AND
EDUCATIONAL
DPC:
WHAT CAN EACH OF US DO?
For EVERY professional interaction:
• Contribute thoughtfully
• Be willing to teach
• Be precise & vigilant with your words
DPC:
WHAT CAN EACH OF US DO?
Each of us MUST view ourselves as leaders, ambassadors & educators as well as be thoughtful in:
• How we contribute eg. discussions re: “ Care delivery models ”
• How we view consultations and referrals as more than JUST patient/family care but as opportunities to educate our colleagues
“
What can I teach, to whom, how and will my response differ next time?
”
DPC:
PRECISION WITH OUR WORDS
With vigilance and respect, seek clarification, correct inaccuracies & teach colleagues, learners, family members, friends…
• “ What do you mean by ‘ terminal ’ ?
”
• “ What do you mean by ‘ palliative ’ ?
”
“ Oh you mean her illness is incurable.
”
“ What ’ s her performance status and level of function as well as goals for her care?
”
DPC:
PRECISION WITH OUR WORDS
With vigilance and respect, seek clarification, correct inaccuracies & teach colleagues, learners, family members, friends…
“ Jeff, can I talk to you about a referral we have made to pain clinic?
”
“ Nope. But happy to speak about a referral made to palliative care clinic. Did you tell the pt she was being seen in palliative care clinic?
”
DPC: OUR TIME IS NOW!!!
Who are we?
What does being a DPC Member mean?
What do we do?
Why do we matter?
Where are we going?
How will we get there?
What can each of us do?
jeff.myers@sunnybrook.ca