Report of the APhA-ASP Resolutions Committee
advertisement

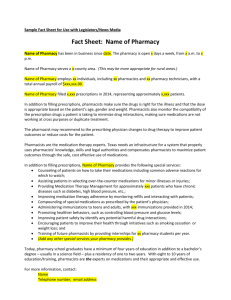
APhA Academy of Student Pharmacists – House of Delegates Report of the 2016 APhA-ASP Resolutions Committee PROPOSED RESOLUTIONS 2016.1 – Increasing the Security of Pharmacies APhA-ASP calls upon all stakeholders to take measures that create an environment that prioritizes the safety and security of patients and pharmacy personnel. These include: 1. The development and implementation of strategies and technologies to deter pharmacy robberies, such as time-delayed safes, panic buttons, stock bottle tracking devices, physical pharmacy design, and video surveillance. 2. The development and implementation of relevant procedures and programs to train all personnel on actions to take during a pharmacy robbery. Background Statement: In the first five months of 2015, U.S. law enforcement agencies reported 382 armed pharmacy robberies, putting 2015 on track to break the record of pharmacy robberies in a year. 1 As a result of this all too common incidence, some pharmacy personnel feel unsafe at work. In fact, student pharmacists have already been victims of these assaults. A pharmacy should be a safe haven for patients and the professionals caring for them. When this space is violated or left vulnerable to attack, patients and personnel no longer feel that their safety is the priority. To foster an environment where pharmacy personnel feel safe, it is pharmacy management’s responsibility to invest in deterrence strategies and training in robbery response designed to mitigate risk. Multiple technologies exist to help discourage a pharmacy robbery by making it more difficult to commit or harder to escape capture and conviction. For example, something as simple as signage indicating that the pharmacy area is under surveillance has been known to serve as a deterrent. Accordingly, the Drug Enforcement Agency (DEA) recommends video surveillance on top or behind registers, as this may discourage potential robbers by capturing their faces on camera.2 Time-delayed safes may also be used to store controlled medications. The time from code entry to opening is variable, decreasing the would-be robber’s ability to plan the theft and increasing the time they must remain in the pharmacy. Walgreens has implemented these safes and signage throughout their pharmacies indicating the use of these safes in several areas of the country. After implementation of this technology, Walgreens reported a decrease in pharmacy robberies, and other chains have since also begun incorporating them in areas of higher crime.3 Additional technologies may also be of service if a pharmacy robbery does occur, such as stock-bottle tracking devices and silent panic buttons. Stock-bottle trackers, invisible to the robbers, can lead law enforcement directly to the perpetrators after the crime has occurred. Silent panic buttons can be activated in stealth to alert law enforcement of a dangerous situation in a pharmacy, allowing for emergency rescue teams to come to the aid of the pharmacy as soon as possible. Finally, pharmacy design can be enhanced to play a role in the safety of personnel during a pharmacy robbery while maintaining an appropriate environment to interact with patients. Examples include more secure points of entry and emergency exits. Educating pharmacy personnel should encompass both prevention and safety protocols. These include measures such as discouraging working alone when possible and acknowledging patients as they come into the pharmacy space. By doing so, the pharmacist indicates their alertness and decreases the amount of time available to commit a crime.4 Some schools and colleges of pharmacy are beginning to take it upon themselves to ensure that students are adequately aware and prepared for the dangers related to pharmacy crimes. Notably, Husson University has hosted an Interprofessional Pharmacy Robbery Prevention seminar for the past 3 years. The seminar has been centered around educating students on how to protect themselves, their businesses, and to aid law enforcement professionals in the event of a pharmacy robbery.5 Report of the 2016 APhA-ASP Resolutions Committee – Page 1 of 6 In most pharmacies, there are more safeguards in place for inventory than for the staff. Ultimately, the culture of pharmacy safety must encompass both the protection of product and the protection of people. The primary responsibility must be to proactively protect our patients and personnel from physical harm and emotional trauma related to a robbery in the pharmacy. Currently, there are no minimum standards for training or preventive measures. This resolution hopes to start the conversation and advance the culture of safety within the pharmacy profession. References: 1. Barker, A. Top 20 States for Pharmacy Robberies. July 21, 2015. http://www.pharmacytimes.com/ contributor/alex-barker-pharmd/2015/07/top-20-states-for-pharmacy-robberies. Accessed January 6, 2016. 2. Pharmacy Robbery and Burglary: Tips to Protect your Customers, your Business, and Yourself. Drug Enforcement Agency Office for Diversion and Control and National Association of Boards of Pharmacy. http://www.deadiversion.usdoj.gov/pubs/brochures/pharmtheft.pdf. Accessed January 6, 2016. 3. Lowery, M. Walgreens installs time-delayed safes to deter pharmacy robberies. August 6, 2014. http://drugtopics.modernmedicine.com/drug-topics/content/tags/controlled-substances/walgreens-installstime-delayed-safes-deter-robberies?page=0,0. Accessed January 9, 2016. 4. Poquette, J. What to do if your pharmacy is being robbed. February 26, 2015. http://www. thehonestapothecary.com/2015/02/26/what-to-do-if-your-pharmacy-is-being-robbed/. Accessed January 9, 2016. 5. Husson University Sponsors 3rd Annual Interprofessional Pharmacy Robbery Prevention Seminar. November 17, 2014. http://www.husson.edu/news/husson-university-sponsors-the-3rd-annual-interprofessionalpharmacy-robbery-prevention-seminar. Accessed January 9, 2016. 2016.2 – Pharmacist Administration of Injectable Medications 1. APhA-ASP supports pharmacists and student pharmacists administering non-vaccine injectables, including but not limited to, antipsychotics, long-acting contraceptives, and other hormone therapy pursuant to prescription, protocol, or collaborative practice agreement. 2. APhA-ASP supports the development of programs to properly train pharmacists and student pharmacists to administer non-vaccine injectables, such as continuing education and certificate training programs. 3. APhA-ASP encourages all stakeholders, including but not limited to, pharmacies, health-systems, and third party payors, to develop a sustainable and financially viable compensation model for pharmacist administration of non-vaccine injectables. Background Statement: Many patients currently prescribed non-vaccine injectable medications are unnecessarily burdened by not only the lack of accessibility to providers who can administer their medications, but also increased risks and additional costs. For example, if patients are prescribed an injectable medication they must either (1) self-inject, which possess inherent risk for patients with a poor understanding of administration techniques, or (2) return to a physician’s office to receive the injection, increasing overall costs and health care burden. These barriers can cause poor patient compliance and poor overall patient health due to the patient’s desire to avoid these current obstacles in care. In response to these problems, 21 states have granted pharmacists the authority to administer non-vaccine injectable medications. Each state’s board of pharmacy has granted this authority in a variety of ways through laws and regulations. Some states require there to be a mechanism in place like a collaborative practice agreement or protocol-based prescription order for the pharmacist to administer non-vaccine injectables, while others provide the pharmacist broad authority. Additionally, most boards of pharmacy have required these pharmacists to complete approved training courses and obtain appropriate life support training.1 These actions have had direct positive impacts on many patient populations, in particular patients with mental health disorders who are taking injectable antipsychotics and patients taking long-acting reversible contraceptives (LARC). Report of the 2016 APhA-ASP Resolutions Committee – Page 2 of 6 Pharmacists’ role in family planning has greatly increased, and female patients have indicated interest in obtaining contraceptives from pharmacists. In fact, many patients are already acquiring contraceptive medications from pharmacists, demonstrating patients comfort with pharmacists playing a larger role in the contraception medication choices.2 The ability for pharmacists to both dispense and administer LARCs could lead to better overall management, resulting in better outcomes for patients. Pharmacists can also play a greater role in the medication management of patients with mental health disorders. Currently, 1 in 4 Americans over the age of 18 have a diagnosed mental condition. Furthermore, 91% of all mental health patients feel comfortable getting their medications from a pharmacist. This creates an excellent opportunity for pharmacists to further develop their relationships with these patients and offer them additional, more comprehensive services through their ability to administer antipsychotic injectable medications, thereby increasing patient compliance. 3 APhA-ASP Resolutions 2002.2 and 2013.2 affirm pharmacists’ ability to administer immunizations. Additionally, APhA-ASP Resolution 2014.2 acknowledges pharmacists’ ability to administer injections in life-threatening situations such as naloxone and epinephrine. These resolutions highlight the Academy’s belief that pharmacists possess the skills and capabilities required to administer injectable medications. As pharmacists’ role continues to increase clinically in both community and inpatient settings, the profession is not only more qualified, but also more adequately positioned than ever before to positively impact large patient populations by administering nonvaccine injectable medications. The APhA-ASP Resolutions Committee believes that by allowing pharmacists—the most accessible health care providers—to participate in this aspect of patient care, better patient outcomes could be achieved as a result of increased compliance through availability and convenience of care. References: 1. Oji V, McKoy-Beach Y, Pagan T, Matike B, AkiyodeO. Injectable administration privileges among pharmacists in the United States. Am J Health-Syst Pharm. 2012;69(22):2002-05. 2. Rafie S, Mcintosh J, Shealy K, et al. Roles of the pharmacist in the use of safe and highly effective long-acting reversible contraception: An opinion of the Women's Health Practice and Research Network of the American College of Clinical Pharmacy." Pharmacotherapy. 2014; 34(9): 991-99. 3. Papataxiarchis M. Managing Schizophrenia: The Role of Pharmacies in Providing Continuing Care. December 10, 2014. http://www.pharmacytimes.com/publications/ directions-in-pharmacy/ 2014/ december2014/managing-schizophrenia-the-role-of-pharmacies-in-providing-continuing-care. Accessed January 9, 2016. 2016.3 – Establishing Immunization Requirements 1. APhA-ASP affirms the valuable role immunizations play in protecting the public and strongly recommends that all persons receive immunizations currently recommended by the CDC, except when medically contraindicated. 2. APhA-ASP recommends all private and public educational or child-care institutions require enrollees and employees to receive all CDC-recommended immunizations, except when medically contraindicated. 3. APhA-ASP strongly affirms that it is the professional responsibility of all health care personnel to receive CDCrecommended immunizations and supports their employers mandating immunizations as a condition of employment, volunteering, or training, except when medically contraindicated. Background Statement: Immunizations are an important public health tool used to prevent the spread of infectious disease. With the advent of each immunization, there has been a corresponding major decline in that disease over the subsequent years, a product of individual protection and herd immunity. However, amid increasing confusion and misinformation regarding the safety of immunizations, vaccine-preventable diseases are resurging. A recent study published by the Centers for Disease Control and Prevention (CDC) states that the number of measles cases in Report of the 2016 APhA-ASP Resolutions Committee – Page 3 of 6 2014 increased to nearly 1,000 cases, when in 2000, the disease had been declared eradicated within the United States.1 Unlike most medications, the decision to deny or defer immunizations affects more than the person making the decision. By refusing immunization, individuals compromise the protection of entire institutions and communities. As demonstrated by the recent measles outbreak in Disneyland, herd immunity has been compromised. Therefore, all persons who are candidates for immunization should receive all current CDC-recommended immunizations unless contraindicated. Furthermore, there is a need for more stringent immunization requirements to help protect the most vulnerable segments of the population, especially children. To illustrate, since 2010, there have been between 10,000 and 50,000 cases of Whooping cough each year in the United States and about 10 to 20 infants, most of whom were too young to be fully vaccinated, died as a result of a vaccine-preventable disease.2 Current regulation and legislation on immunization requirements differ from state to state. A recent systematic review illustrates the positive correlation between the level of regulation and the percent of immunization rates. The data suggest that adopting more stringent requirements lowers the number of people who choose not to immunize, leading to higher immunization rates and greater protection for the communities. For example, in 2012, states with more effective immunization requirements had 16.45 cases of pertussis versus 54.19 cases per 100,000 in states with weaker regulation.3 In Connecticut, influenza immunization rates of children aged 6 months to 5 years increased from 67.8% to 84.1% within 3 years following the implementation of an immunization requirement. Additionally, influenza associated hospitalization rates decreased by 12%. 4 Requiring immunizations protects public health much in the same way that directly observed therapy of tuberculosis medications protects public health. By preventing the spread of disease on an individual level, all are made safer. It is the professional responsibility of all those who seek to heal to protect patients, the age old concept of “first, do no harm.” Not only should health care providers model healthy behavior to their patients, but they should take steps to actively keep their patients healthy. Available evidence indicates that employer requirements substantially increase vaccination rates among health care providers, from around 50% to over 90%. 5,6 Patients should have every assurance that all reasonable precautions are taken to prevent spreading disease in health care institutions. In 2007, the APhA House of Delegates adopted policy that called for all pharmacy personnel to receive all immunizations recommended by the CDC for health care workers. In 2011, the House supported an annual influenza vaccination as a condition of employment, training, or volunteering within an organization that provides pharmacy services or operates a pharmacy or pharmacy department, unless a valid medical or religious reason precludes vaccination. Just as health care professionals protect their patients and themselves through proper hand hygiene, so must we protect our patients and ourselves through immunization. In short, the health of the public should not be at risk from those whose job it is to preserve it. References: 1. Buttenheim A, Sethuraman K, Omer BS, Hanlon LA, Levy M, Salmon D. MMR vaccination status of children exempted from school-entry immunization mandates. Vaccine. 2015;33(46):6250-56. 2. Centers for Disease Control and Prevention. Five Important Reasons to Vaccinate your Child. http://www.vaccines.gov/more_info/features/five-important-reasons-to-vaccinate-your-child.html. Accessed January 9, 2016. 3. Bradford WD, Mandich A. Some state vaccination laws contribute to greater exemption rates and disease outbreaks in the United States. Health Affairs.2015;34(8):1383-90. 4. Hadler JL, Yousey-Hindewy K, Kudish K, Kennedy ED, Sacco V, Cartter ML. Impact of requiring influenza vaccination for children in licensed child care or preschool programs. Center of Disease Control. Last Accessed January 8, 2016. 5. Field RI. Mandatory vaccination of healthcare workers. Health Care and Law. 2009;34(11):615-18. 6. Pitts IS, Maruthur MN, Millar RK, Perl MT, Segal J. A systematic review of mandatory influenza vaccination in healthcare personnel. American Journal of Preventative Medicine. 2014;47(3):330-340. Report of the 2016 APhA-ASP Resolutions Committee – Page 4 of 6 2016.4 – Increasing Patient Access to Pharmacist-Prescribed Medications 1. APhA-ASP encourages legislative and regulatory changes that would enable pharmacists, with appropriate training and working as integral members of the health care team, to assess the patient and prescribe certain medications such as those for contraception, tobacco cessation, and international travel. 2. APhA-ASP encourages the development of sustainable and financially viable compensation models for pharmacist-prescribed medications. Background Statement: With the current shortage of primary care providers, there is an ongoing issue of access to important primary care services, including medications. The safe and effective use of some medications does not require a diagnosis, such as medications for contraception, tobacco cessation, and international travel. Due to the level of education and training provided within the PharmD curriculum, pharmacists are qualified to assess, plan, implement, monitor, and evaluate patient use of these medications. While access to many health care professionals authorized to prescribe medications requires an appointment or emergency room visit, pharmacists are a knowledgeable, accessible, yet underutilized health care professional positioned to fill gaps in care and meet patients’ medical needs. Unintended pregnancy is prevalent nationwide, with more than 50% of pregnancies being unplanned.1 As a result of the high incidence of unintended pregnancy, Oregon passed State House Bill 2879 into law, authorizing pharmacists to prescribe and dispense hormonal contraceptive products to patients without a prescription. 2 Two years prior in October 2013, California passed state Senate Bill 493 to permit pharmacists to furnish selfadministered hormonal contraceptives.3 In a 2008 study published in JAPhA, pharmacists identified women at risk of unintended pregnancy and prescribed hormonal contraceptives after an assessment. Nearly all patient respondents expressed a willingness to continue to see pharmacist-prescribers and to receive other services from them.4 As a result of increased pharmacist involvement and access to oral contraceptives, it is estimated that there could be as much as a 25% decrease in unintended pregnancy and a reduction in overall health care costs.5 Pharmacists already play a valuable role in tobacco cessation and increasing the quality of life of patients who wish to quit smoking.6 Among patients receiving nicotine replacement therapy (NRT), 46% of individuals reported that meeting with pharmacists would increase their probability of quitting.7 Additionally, in a small scale study performed in a pharmacist-led smoking cessation clinic, patients were treated with NRT, buproprion, or varenicline, and at 6 months 52.4% of all patients and 89% of patients on buproprion or varenicline had quit smoking.8 Currently, pharmacists in New Mexico play a central role on the health care team and provide valuable patient care services by providing tobacco cessation counseling and prescribing medications under a state-wide protocol.9 This expanded privilege increases patient access to care that supports their efforts to quit tobacco products, thereby increasing personal and public health. Pharmacists are also well qualified to provide travel medications to patients given that the choice of those medications is highly guided by factors independent of diagnosis. Evidence has shown that there is an 84.7% acceptance and satisfaction with pharmacists as providers of international travel health services. In addition, there is an inconsistency in medications prescribed for a variety of travel health related prophylaxis and an overall greater acceptance amongst patients when dealing with pharmacists.10 Through legislative action we can practice at a level of health care more appropriate for our training. The comprehensive training pharmacists receive through school curriculum and continuing education prepares the profession of pharmacy for this expanded role. Most importantly, increasing the scope of practice for the pharmacy profession provides increased access to care for patients. References: 1. Mosher WD, Jones J, Abma JC. Intended and unintended births in the United States: 1982–2010. National Health Statistics Reports. No 55. July 24, 2012. National Center for Health Statistics. Report of the 2016 APhA-ASP Resolutions Committee – Page 5 of 6 2. Oregon House Bill 2879. Pharmacy Practice. Effective July 6, 2015. https://olis.leg.state.or.us/liz/2015R1/Measures/Overview/HB2879. 3. California Senate Bill 493, Pharmacy Practice. Approved October 1, 2013. http://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201320140SB493. 4. Gardner JS, Miller L, Downing DF. Pharmacist prescribing of hormonal contraceptives: results of the Direct Access study. J Am Pharm Assoc. 2008;48(2):212-21. 5. Foster DG, Biggs MA, Phillips KA, Gridlay K, Grossman D. Potential public sector cost-savings from over-thecounter access to oral contraceptives. Contraception. 2015;91(5):373-79. 6. Zillich A, Ryan M, Adams A. Effectiveness of a pharmacist-based smoking cessation program and its impact on quality of life. Pharmacotherapy. 2002;22(6):759-65. 7. Hudmon, Karen; Hemberger, Kymberli; Corelli, Robin. The Pharmacist’s Role in Smoking Cessation Counseling: Perceptions of Users of Nonprescription Nicotine Replacement Therapy. J Am Pharm Assoc. 2003;43(50:57382. 8. Philbrick AM, Newkirk EN, Farris KB, McDanel DL, Horner KE. Effect of a pharmacist managed smoking cessation clinic on quit rates. J of Pharm Pract. 2009;7(3):150-56. 9. New Mexico Board of Pharmacy. Protocol for Pharmacist Prescribing for Tobacco Cessation. http://www.rld.state.nm.us/uploads/FileLinks/e3740e56e0fe428e991dca5bd25a7519/protocolofpharmacistp rescribingtobaccocessation.pdf. Accessed January 6, 2015. 10. Hess KM, Dai CW, Garner B. Measuring outcomes of a pharmacist-run travel health clinic located in an independent community pharmacy. J Am Pharm Assoc. 2010;50(2):174-80. Report of the 2016 APhA-ASP Resolutions Committee – Page 6 of 6