Comprehensive Geriatric Assessment
advertisement

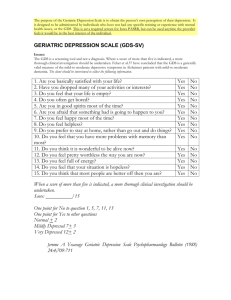
Comprehensive Geriatric Assessment John E Morley St Louis University St Louis VAMC GRECC “Old age is like a plane flying through a storm. Once you are aboard there is nothing you can do about it.” - Golda Meier Typical medical evaluation and intervention: • 85 year old woman has uncontrolled hypertension on one blood pressure medication (185/80) • Plan: Add a second blood pressure medication Typical medical evaluation and intervention: 2 weeks later…. Comprehensive Geriatric Assessment • 85 year old woman has uncontrolled hypertension on one blood pressure medication 1. 2. 3. 4. 5. 6. 7. 8. Lives alone Gait and balance abnormality Osteoporosis Mild memory impairment Incontinent of urine Vision impairment OTC meds Difficulty with cleaning Comprehensive Geriatric Assessment • 85 year old woman has uncontrolled hypertension on one blood pressure medication 1. 2. 3. 4. 5. 6. 7. 8. Lives alone (daughter will help with meds) Gait and balance abnormality (home therapy) Osteoporosis (treated) Mild memory impairment (eval for dementia) Incontinent of urine (treated) Vision impairment (fix or find glasses, ophtho. appt) OTC meds (discard) Difficulty with cleaning (Home OT-eval fall risk) Comprehensive Geriatric Assessment • 85 year old woman had uncontrolled hypertension on one blood pressure medication (2nd visit): • Daughter came, helping with meds, BP fine • Gait and balance is better-no falls • No longer rushing to the bathroom (not incontinent) • Discussion about dementia and best options to keep her living independently Comprehensive Geriatric Assessment (CGA) • Older patients may have multiple problems, that interact • Looks at these interactions (i.e. whole patient) • Identifies current and potential problems Comprehensive Geriatric Assessment • GEMU 1.68 (1.17 - 2.41) • Hospital 1.49 (1.12-1.98) • Home assessment 1.20 (1.05 – 1.37) LIVING AT HOME Comprehensive geriatric assessment: a meta-analysis of controlled trials Stuck et al, Lancet 342:1032, 1993 Comprehensive Geriatric Assessment • • • • • • • • • • • 7 or more medicines Fatigue Cannot climb stairs or walk one block Sadness Memory problems Weight loss Falls Urinary incontinence Uncontrolled pain Help with managing money or shopping Unhappy with physicians treatment The I’s of Geriatrics The Modern Geriatric Giants Instability (frailty) Incontinene Intellectual impairment Iatrogenesis Incoherence (delirium) Insulin resistance (diabetes) Immobility Inanition (malnutrition) Impoverishment Lawton’s IADLs • • • • • • • • Telephone Shopping Food Preparation Housekeeping Laundry Transportation Taking medicine Managing Money Status Post Fall is a Delirium Equivalent Vowel test Confusion Assessment Methodology Families and physicians fail to recognize dementia. Mini-Mental Status Examination Folstein et al. 1975 1. Educationally dependent 2. Both false positives and false negatives 3. Minimal testing of visuospatial system 1.0 1.0 0.9 0.9 0.8 0.8 0.7 0.7 0.6 0.6 Sensitivity Sensitivity ROCs For SLUMS &MMSE for MCI > HS Education 0.5 0.4 0.5 0.4 0.3 0.3 Area Under Curve = 64.3% 0.2 Area Under Curve = 94.1% 0.2 0.1 0.1 0.0 0.0 0.0 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 0.1 0.2 0.3 0.4 1-Specificity SLUMS 0.5 0.6 1-Specificity MMSE 0.7 0.8 0.9 1.0 Depression • Are you sad? • Beck Depression Inventory • Yesavage Geriatric Depression Scale FRAILTY DEFINITION OBJECTIVE Fried et al J Gerontol 56A M146,2001 •Weight Loss(10 lbs in 1 year) •Exhaustion(self-report) •Weakness (grip strength;lowest 20%) •Walking speed(15 feet; slowest 20%) •Low Physical Activity(Kcals/week;lowest 20%) Female > Male 6.9% FRAILTY • • • • • Fatigue Resistance (Climb stairs) Aerobic (Walk one blocK) Illnesses Loss of weight Gait and Balance • Get up and Go • One leg stand • Tinetti Gait and Balance • Dual Tasking • Dancing • Strength (Cybex) • Muscle Pain (Polymyalgia Rheumatica) Objective Measures of Physical Function • Get-Up-and-Go • >30 sec fall risk • 6 Meter walk • <5.8 sec • Gait Speed • >6.0 sec • 6 Minute Walk • <300 m mortality <400 m functional impairment Fear of Falling Measure Blood Pressure Standing in ALL Older Persons ORTHOSTATIC HYPOTENSION POSTPRANDIAL HYPOTENSION (“BIG MAC ATTACK”) VARIABLE • • MORE COMMON IN AM • PREVALENCE 26% • falls syncope stroke myocardial infarction death • STIMULATED BY CARBOHYDRATE • DUE TO CGRP RELEASE PSEUDOHYPERTENSION OSLER MANEUVER (Messerli) PREVALENCE 7.2% Poor predictive value Predicts cardiovascular disease WHITE COAT HYPERTENSION PREVALENCE 7.1 TO 21% No LVH AMBULATORY MONITORING BMD • Done in all women by 50 years or at menopause • Done in men by 70 years • Repeat in 2 year in same season to see rate of fall S.N.A.Q 1) 1. 2. 3. 4. 5. 3) 1. 2. 3. 4. 5. My appetite is Very poor Poor Average Good Very good Food tastes Very bad Bad Average Good Very good < 15 predicts significant weight loss within 6 months 2) 1. 2. 3. 4. 5. 4) 1. 2. 3. 4. 5. When I eat, I feel full after Eating only a few mouthfuls Eating about a third of a plateful Eating over half a plateful Eating most of the food Hardly ever Normally I eat Less than one full meal a day One meal a day Two meals a day Three meals a day More than three meals a day, including snacks SNAQ Sensitivity (%) Specificity (%) 81.3 76.4 10% weight 88.2 loss 83.5 5% weight loss Malnutrition Universal Screening Tool Weight Loss Score (unplanned wt loss in 3-6 mo) BMI Score BMI >20-0 (>30 obese*) BMI 18.5-20.0 BMI <18.5 =0 =1 =2 Wt loss <5% Wt loss 5-10% Wt loss >10% =1 =2 Acute Disease Effect Score = 0 Add a score of 2 if there has been or is likely to be no nutritional intake for >5 days Add all scores Overall Risk of Malnutrition and Management Guidelines 0 Low risk Routine clinical care •Repeat screening Hospital – weekly Care homes-monthly Community-annually for special Groups (e.g. those >75yrs) 1 Medium Risk 2 or more High risk Observe Treat* •Document dietary intake for 3 days if subject in hospital or care home •If improved or adequate intake, little clinical concern; if no improvement, clinical concern – follow local Policy •Repeat screening Hopital –Weekly Care home – at least monthly Community – at least every ____ •Refer to dietician, nutrition support team or implement local policy •Improve and increase overall Nutritional intake •Monitor and review care plan Hospital – weekly Care home – monthly Community – monthly •Unless detrimental or no benefit is expected from nutritional support e.g. imminent death The Mini-Nutritional Assessment (MNA) Scale Anthropometric Parameters • • • • • • • • • • • • • Weight change BMI Arm span Mid-arm or Calf Circumference Triceps skinfold MAMC and MAMA Waist Circumference Bioelectrical impedance Dual photon absorptiometry (DEXA) CT/MRI Ultrasound Underwater weighing Stable isotopes Abdominal Adiposity: The Critical Adipose Depot A little poison now and then makes for agreeable dreams, and much poison in the end for an agreeable death Nietzche: Thus Spoke Zorathiestra Approach to Drug History 1. What is the target problem being treated? 2. Is the drug necessary? 3. Are nonpharmacologic therapies available? 4. Is this the lowest practical dose? 5. Could discontinuing therapy with a medicine help reduce symptoms? 6. Does this drug have adverse effects that are more likely to occur in an older patient? 7. Is this the most cost-effective choice? 8. By what criteria, and at what time, will the effects of therapy be assessed? Elementary, My Dear Watson Other Tests • • • • • • • • • Hearing Vision Sleep apnea Advance Directives Health Promotion Hallpike-Dix Driving Guns Sex (ADAM)