Peripheral Neuropathy
advertisement

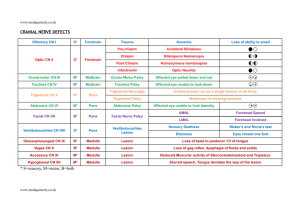
Peripheral Neuropathy Neurology Rotation Lecture Series Last Updated by Lindsay Pagano Summer 2013 Case Presentation You are consulted by the NICU to see a 3500 g newborn male with decreased movement of his right upper extremity. • born at 39 weeks via SVD, vacuum assist • Pregnancy complicated by LGA, mom with IDDM • Complicated by nuchal cord x1, shoulder dystocia with left humeral fracture • Apgars 0, 2, 6 at 1, 5, 10 minutes of life, respectively • Resuscitated, intubated, and brought to the NICU • PE: normal except for – S – Neuro: normal except for • MS: mildly sedated • Motor: RUE with hypotonia, internally rotated, with elbow extension and forearm pronation; no spontaneous motion of RUE • Sensory: no movement of RUE to pain • Reflexes: trace-absent in RUE • Differential? Brachial Plexus Injuries • • Injuries to nerve roots arising from C5-T1 from traction, compression, tear or avulsion 0.5-2 per 100 live births – – – – • More common in term infants More common in RUE Associated with LGA, GDM, AMA, shoulder dystocia, clavicular fractures Also seen in nontraumatic births, and in utero Erb’s Palsy – Injury to superior trunk, C5-6 – “waiter’s tip”: internal rotation and adduction of the shoulder, elbow extension, forearm pronation, finger flexion • Klumpke’s Palsy – Injury to inferior trunk, C8-T1 – Elbow flexion, forearm supination, wrist extension, claw deformity of the hand – +/- Horner Syndrome due to sympathetic fiber involvement • Prognosis – Recovery over 3-6 months is predictive of overall recovery; PT/OT important – May require surgery to reanneal or graft the injured nerves (earlier [by 6 months] is better) Bell’s Palsy • Acute facial nerve palsy of unknown etiology; may be congenital • 2/10,000 per year • Onset over hours of unilateral facial palsy – Includes the ENTIRE face (LMN) – May also include hyperacusis, decreased tearing, loss of taste • May be associated with – – – – OM Lyme Mobïus syndrome (with ocular abduction palsy) Viral infections: varicella, zoster, coxsackie • Diagnosis: clinical • Treatment: No clear evidence for steroids or acyclovir in children (AAP insufficient evidence to recommend treatment) CIDP • • • • • • • Aka Chronic Inflammatory Demyelinating Polyneuropathy – Like a chronic form of Guillan-Barré, which is also known as AIDP (acute inflammatory demyelinating polyneuropathy) Immune mediated demyelinating polyneuropathy Presents with lower extremity weakness and sensory changes, and less commonly, CN neuropathies One of three clinical syndromes: 1. Monophasic illness with symptoms lasting > 2 months 2. Slow progressive course 3. Relapsing/remitting course NCS consistent with demyelination LP with increased protein Treatment: – Scheduled IVIg – Other options: PLEX, steroids Hereditary Motor and Sensory Neuropathy aka Charcot-Marie-Tooth disease type 1A • • • AD, duplication in the peripheral myelin protein 22 (PMP22) gene on 17p11.2-12 Progressive distal polyneuropathy – Begins in intrinsic foot muscles, and then progresses to include proximal weakness, as well as to involve hand muscles – Hammer toes, pronounced arch, thin tapered appearance of legs Onset in first 2 decades – First symptoms include: • • • • Difficulty with heel walking Pes cavus Calf atrophy Decreased reflexes – Progresses to include • Worsening of above • Impairment of vibration and proprioception • • Touch, pain and temperature sensation less commonly involved Diagnosis – EMG/NCS – Genetic testing Other Peripheral Neuropathy Differential Diagnoses • Toxins/heavy metals – Eg arsenic, lead, thallium • Hypothyroidism • Systemic conditions: diabetes, uremia, porphyria, SLE, Churg-Strauss, polyarteritis nodosa, lyme, rabies, sarcoid • Older individual lab screening – CBC, CMP, SPEP, glucose tolerance test, ESR, B12, ANA, ANCA, RF, SSA, SSB, B6, B1, PNP, anti-gliadan Ab • Complication of metabolic disease – Not usually the presenting anomaly – Leukodystrophies, lipid storage diseases (Gaucher, Tay-Sachs), peroxisomal disorders, mitochondrial disorders PREP question A 14 year old boy presents to your office because the side of his face is drooping. His mother states that he complained yesterday of decreased food taste. Today, while at school, he could not use the microscope in science class because he couldn’t close his left eye, and his teacher noted that his smile was crooked. PE reveals no abnormalities and no vesicles in his ears. Mental status on neuro exam is normal, pupil responses are normal, extraocular movements are full, and there is no nystagmus or reported double vision. He is unable to close his left eye or raise his left eyebrow, has decreased left-side nasolabial folds, and cannot close his mouth to puff out his cheeks. His palate and tongue movements are normal. Motor examination reveals normal proximal and distal strength in both arms and normal regular and tandem gait. Of the following, the MOST appropriate initial diagnostic procedure is A. Blood test for antistreptococcal antibodies B. Brain magnetic resonance imaging C. Edrophonium (Tensilon®) test D. No further testing E. Noncontrast head computed tomography scan D. No further testing Evaluating for Bell’s palsy • Localize the weakness • Look for sensory involvement • No clear evidence for steroids or acyclovir in children (AAP insufficient evidence to recommend treatment) Regarding the other choices: A. ASO: typically associated with abnormal movements, not a fixed deficit B. MRIbrain: doesn’t fit localization C. Edrophonium test: not consistent with MG (UL, ptosis, resp symptoms) E. Noncon CThead: see B