The End Stage Renal Disease - End Stage Renal Disease Network
advertisement

Fistula First
A Seminar for The Nephrology Community
Corpus Christi, Texas
July 31, 2004
Co Provided By:
Alamo City & Heart of Texas Chapters
of The American Nephrology
Nurses Association
Agenda
Noon Welcome & Introductions:
Alan Saltarelli , RN, ANNA Alamo City Chapter -President
Balbi Godwin, RN, ANNA Heart of Texas Chapter -President
12:15 Fistula First Overview: Alex Rosenblum, RN, CNN
12:45 Vascular Access Surgery 101: Pho DO, MD
{Supported with a unrestricted educational grant from Bard }
1:30 Interventional Techniques 101: Anwar Gerges, MD {Supported with a
unrestricted educational grant from Cordis }
2:15 Break/Exhibits
2:45 The ABCs of AV Fistulas: Janet Holland, RN, CNN
4:00 Nurse to Nurse: Moderators-Janet Holland, Alex Rosenblum &Bobbie Knotek
A special opportunity to listen, learn and ask questions of nurses from facilities who have met the
Fistula First Goals of attaining 40% + AVF rates at their dialysis facility.
4:45 Adjourn
Goals of Today’s Conference
•Expand awareness of the Centers for Medicare &
Medicaid Services sponsored Fistula First Quality
Improvement Initiative.
•Review advanced surgical/endovascular
techniques for placement and/or rescue of the AVF.
• Share practice experiences that appear to
positively impact of AVF placement and patency
rates.
• Empower participants to have confidence that they
can & do play an active role in meeting project
goals.
Reminder: Fistula First Resources in the Back of the Room
What are the
ESRD
Networks?
•18 regional agencies under contract with the Centers for
Medicare & Medicaid Services
•Developed in 1978 to assess/improve quality of care for
ESRD patients
26,397 patients (2/2004)
24,254 In-Center HD patients
Who does the
ESRD Network
of Texas serve?
84 Home HD patients
2,055 PD patients
~ 7,000 Transplant patients
• Quality Improvement
• Information Management
• Consumer Services
End Stage Renal Disease Network of Texas Committees
Medical Review Board
Nephrologists
Robert Hootkins, MD, Chair
Jim Cotton, MD
Stuart Goldstein, MD
Denise Hart, MD
Donald Molony, MD
Fernando Raudales, MD
Mouin Seikaly, MD
Ruben Velez, MD
Patients
Cynthia Hays
Nurses
Molly Itty, RN, CNN
Jeanne Nishioka, RN, CNN
Executive
Committee
Richard Gibney, MD, Chair
Dietitians
Alice Chan, RD, LD
Eileen Mauk, PhD
Dionicio Alvarez, MD
John Bell, MD
Pat Dubose, RN
Amy Hackney, MBA
Social Workers
Mary Beth Callahan, LMSW
Linda Schacht, LMSW
Robert Hootkins, MD
Melvin Laski, MD
Marlon Levy, MD
Transplant Surgeons
Ingemar Davidson, MD
Charles Van Buren, MD
Susan Raulie, RN
Project Surgical/Interventional Radiology
Advisory Committee
Alan Lumsden, MD, Chair
Gerald Beathard, MD
Cary Munschauer
Mary Brandt, MD
George Nassar, MD
Ronald Blumoff, MD
Greg Pearl, MD
Ingemar Davidson, MD
Eric Peden, MD
Hector Diaz-Luna, MD
Wade Rosenberg, MD
Greg Jaffers, MD
Stephen Settle, MD
Edward Gomez, MD
Michael Silva, MD
Why is CMS Focusing on
Hemodialysis Vascular Access?
Quality of Care/Public Health Concerns:
• Fewer infectious complications:
AVFs: 4.4 - 12 x less infection rates than AVGs
• Fewer interventional procedures to keep patency:
AVFs: 2.4 - 7.1 x less salvage procedures than AVGs
• Better 1 year primary patency in incident HD patients:
68% for AVFs & 49% for AVGs
Allon and Robbin. Kidney Int. 62:1109-1124, 2002.
Nassar and Ayus . Kidney Int. 60:1-13, 2001.
Pisoni RL, et al. Kidney Int. 61:305-316, 2002.
Why is CMS Focusing on
Hemodialysis Vascular Access?
• Cost Containment:
• Estimated costs for VA related complications = $1-2 billion
(~8k per patient) 200-250K procedures per year
• 20% of hospitalizations related to VA dysfunction
• ESRD = ~0.5% of Medicare population & 5% of budget
• Doubling of dialysis population by 2010 (50k in Texas)
VA Practice variations:
•AVF variation between states, Networks and countries
(80% AVF in Europe/Asia)
Message for the Surgeon - By a Surgeon
Why only AV Fistulas?
• You should do this because: • You will like:
• Patients with AVFs live
• High patient and
longer
nephrologist satisfaction
• Patients with AVFs have 8x • Simple, safe outpatient
fewer access complications
procedures
Avoid or markedly decrease hospital admissions and
emergency operations for infection, bleeding, steal
syndrome, and thrombosis.
William Jennings, MD, Tulsa Vascular Access Surgeon
What Do We Know About
Hemodialysis Vascular Access
Utilization in the US?
Percent of Prevalent Patients
with AV Fistula As of Feb 2004
60
52.4
50
% of Patients
43 42.8 42.1
40
38.9
37.3 37.1 36.3
36
34.5 33.6 33.1
30
31.8 31.4 30.7
30 29.4
28
26.7
20
10
0
16 15 1
2 18 3 17 10 7 US 4 12 6
Network
CMS FF Dashboard
9
5 11 8 13 14
What Do We Know About
Hemodialysis Vascular Access
Utilization in the World?
Top 10 City AVF Prevalent Rates
As of April 2004
New York
44%
Los Angeles
41%
Chicago
NR
Houston
25.7%
Philadelphia
28.5%
Phoenix
37.5%
San Diego
39.1%
San Antonio
22.1%
Dallas
36.9%
Detroit
18%
Data Source: Network #14 Data base collected informally from regional ESRD Networks
AVF Utilization Among Prevalent HD Patients By Country
As of Sept. 2003
100
90
91
86
84
% of Patients
80
79
78
71
70
68
60
60
58
54
50
40
30
30
20
10
0
JPN
IT
GE
SP
FR
ANZ
Country
UK
BE
SW
CA
U.S.
AVF Utilization Among Incident HD Patients By Country
As of Sept. 2003
90
80
79
% of Patients
70
60
49
50
49
40
30
19
20
16
10
0
JPN
EUR
ANZ
Country
CA
U.S.
What Do We Know About
Hemodialysis Vascular
Access Utilization in Texas?
Vascular Access Utilization
Texas Prevalence Trends: December 2000-May 2004
100
90
80
December 2002
December 2002
May 2004
U.S. 2004
December 2003
% Patients
70
60
49.4
50
41
35.5
40
30
28.6
27
20.2
20
10
0
Fistula
Graft
Catheter
Percent Fistula Utilization By County
as of March 2004
Fistula Utilization
10-19%
20-29%
30-39%
40-49%
El Paso
37.5%
(39.9%)
( ) = November 2003 AVF rates
Tarrant
34.1%
(32.7%)
Dallas
37.6%
(38.0%)
Lubbock
26.6%
(15.4%)
McLennon
21.0%
(21.4%)
Smith
10.7%
(13.5%)
Bell
39.6%
(41.0%)
Liberty
23.0%
(22.2%)
Jefferson
13.3%
(13.0%)
Harris
24.7%
(25.2%)
Travis
27.0%
(28.0%)
Hays
27.9%
(23.8%)
Bexar
22.1%
(17.4%)
Fort Bend
30.2%
(27.8%)
Webb
20.1%
(19.1%)
Counties with 2 or less facilities censored
Nueces
22.1%
(22.9%)
Hidalgo
19.3%
(20.6%)
Cameron
36.3%
(31.4%)
Brazoria
25.7%
(22.8%)
Galveston
32.6%
(30.9%)
Percent Fistula Utilization By City
as of March 2004
City
Abilene
Amarillo
Arlington
Austin
Beaumont
Brownsville
Corpus Christi
Dallas
Edinburg
El Paso
Fort Worth
Garland
# Patients
% Fistulas
202
217
301
798
317
323
586
1444
194
1004
884
189
35.3
14.8
44.8
27.0
13.6
30.3
23.8
36.9
18.5
37.5
27.1
46.6
Cities with less than 80 patients excluded
City
Harlingen
Houston
Huntsville
Laredo
Longview
Lubbock
McAllen
Mission
San Antonio
Temple
Tyler
Weslaco
# Patients
% Fistulas
311
3518
204
382
182
407
371
207
2297
225
227
283
42.3
25.7
43.1
20.1
21.8
26.6
19.6
28.3
21.2
40.9
10.7
13.3
Texas Facilities with 40% or More Prevalent AV Fistulas
N = 50 Facilities* as of March 2004
Facility
# Patients
83
GAMBRO - BRYAN/COLLEGE STATION
143
TDC MONTFORD MEDICAL UNIT PRISON
29
GAMBRO - BRENHAM
43
RCG - IRVING DIALYSIS
105
TARRANT DIALYSIS - ARLINGTON
72
RCG - HARLINGEN
46
SCOTT & WHITE - TEMPLE
188
RCG - EL PASO EAST
102
SCOTT & WHITE - ROUND ROCK
55
LEWISVILLE DIALYSIS CLINIC
107
FMC - SWISS AVENUE
153
DAVITA - ELMBROOK KIDNEY CENTER
94
DAVITA - MESA VISTA DIALYSIS
96
FMC - INGRAM
12
TDC HUNTSVILLE MEDICAL UNIT PRISON
145
DAVITA - LOMA VISTA DIALYSIS
198
GAMBRO - DALLAS EAST
86
GAMBRO - UT SOUTHWESTERN
179
FMC - GRAPEVINE
19
HARLINGEN DIALYSIS
127
FMC - DALLAS EAST
32
FMC - TOWN GATE
189
RCG EL PASO KIDNEY CENTER - WEST
65
FMC - ENNIS
44
DAVITA - DENISON
% AVFs
69.9
67.8
58.6
58.1
57.6
54.2
52.2
52.1
51.0
50.9
50.5
50.3
50.0
50.0
50.0
49.0
48.0
47.7
47.5
47.4
47.2
46.9
46.6
46.2
45.5
Facility
AUDI MURPHY VAMC HOSPITAL
TEXAS CITY DIALYSIS
THE DIALYSIS COTTAGE
DAVITA - CENTRAL CITY DIALYSIS
GAMBRO - OAKCLIFF
RCG - BROWNSVILLE
NORTH TEXAS DIALYSIS SERVICES
SCOTT & WHITE - KILLEEN DIALYSIS
DAVITA MONCRIEF DIALYSIS
DAVITA - PEARLAND DIALYSIS
FMC - CORSICANA
FMC - RICHARDSON
UNIVERSITY DIALYSIS - WEST
FMC - COLLIN COUNTY
CHRISTUS CHILDRENS KIDNEY CENTER
SOUTH ARLINGTON DIALYSIS
AMERITECH KIDNEY CENTER - HEB
FMC - TERRELL
TARRANT DIALYSIS - GRAND PRAIRIE
SHANNON DIALYSIS SERVICES
FMC - CLEBURNE
GRAND PRAIRIE DIALYSIS CENTER
DENTON DIALYSIS
DAVITA - HEB DIALYSIS CENTER
FMC - WAXAHACHIE
Note: *Facilities w ith a prevalent AVF rate of 40% or higher for tw o consecutive months
# Patients
31
38
18
90
188
93
14
70
61
40
59
114
110
139
12
149
92
61
61
22
59
32
85
65
70
% AVFs
45.2
44.7
44.4
44.4
44.1
44.1
42.9
42.9
42.6
42.5
42.4
42.1
41.8
41.7
41.7
41.6
41.3
41.0
41.0
40.9
40.7
40.6
40.0
40.0
40.0
Facility Variation In the % of Prevalent Patients with AVF
% of Facility Patients
<10
10-19
20-29
30-39
> 40
All Texas Facilities
# of Facilities
11/03
3/04
21
16
77
74
120
118
50
52
47
54
315
314
% of Facilities
11/03
3/04
6.7
5.1
24.4
23.5
38.1
37.6
15.9
16.5
14.9
17.1
100.0
99.8
The Network MRB has identified facilities with an AVF rate in this range as having an improvement opportunity!
The MRB has identified facilities with 40% AVF rate for 2 + months as "Benchmark"
Page 2
Suggested Strategies to
Increase AVF Rates
Fistula First Change Concepts
1. Routine CQI review of
vascular access
6. Secondary AVFs in AVG
patients
2. Early referral to
nephrologist
7. AVF placement in catheter
patients
3. Early referral to surgeon
for “AVF only”
8. Cannulation training
4. Surgeon selection
10. Continuing education: staff
and patient
5. Full range of appropriate
surgical approaches
9. Monitoring and surveillance
11. Outcomes feedback
Please refer to handouts
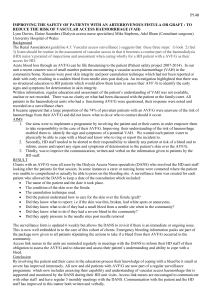
Proven Strategies
To Increase Fistula Rates
Fa ci l i t y S el f -A ssessm en t
Use this self-assessment guide to rate your facility’s use of strategies designed to increase fistula rates
Read the statements below & assign the score that best matches your facility’s current situation
1 = Not under consideration
2 = Under consideration; not started
3 = In start-up process
4 = Working, at least in part
5 = Working well
Does Your Facility . . .
Have an assigned staff member responsible for monitoring facility vascular access (VA) outcomes?
In collaboration with physician, evaluate all non-AVF accesses as part of the CQI process?
In collaboration with physician, develop and document AVF plans for all potentially eligible patients?
Trend vascular placement by surgeon monthly in QA?
Evaluate the status of permanent vascular access placement plans within the first three treatments for new
patients admitted with a “catheter only” and document findings?
In collaboration with your physician, routinely evaluate all AVGs (prior to clotting episodes) for possible
secondary AVF conversion and document findings?
Refer to surgeons that are supportive and skilled in placing secondary AVFs?
In collaboration with physician, refer patients for vessel mapping (if not already performed) to assist surgeon
with access type placement evaluation?
In collaboration with physician, select surgeons based on willingness, skill and outcomes with AVF’s?
In collaboration with physician, indicate in writing on all vascular access surgical referrals that the preferred
permanent access type is an “AVF Only”?
Provide written vascular access history information to surgeons/radiologists when patients are referred for
evaluation?
Discuss specific criteria with interventional radiologists/interventional nephrologists and surgeons for
determining allowable degree of intervention before a new access should be considered?
Request written post-surgical information from surgeon/radiologist – type/results of VA interventions, a
description/drawing of access location, direction of blood flow & care instructions?
Refer to surgeons who are willing to receive and track data on their vascular access rates and outcomes?
In collaboration with physician, refer all AVFs with “failure to mature” at 4 weeks post-op to a surgeon or
radiologist?
Routinely monitor AVF and AVG flow rates/pressures for stenosis using K/DOQI recommended procedures?
Have a vascular access management plan for each patient that facilitates timely referral for complications?
Provide routine in-services for staff on AVF cannulation techniques?
Require that personnel use specific protocols during initial treatments for patients who have a new AVF?
(e.g. needle size, BFR, tourniquet use)?
Assign the most skilled staff to patients who have a new AVF?
Offer the option of self-cannulation to patients willing to pursue this option?
Have a procedure for treating VA infiltrations that includes written patient instructions?
Score
The ESRD Network of Texas Web Site
www.esrdnetwork.org
Welcome to the ESRD Network of Texas Inc.
(#14) Website.
Mission: Support quality dialysis and kidney
transplant healthcare through patient services,
education, quality improvement and data
exchange.
ESRD Network Web Resources
•Fistula First Video and CEU form
•Hemodialysis Access Referral Form To Surgery/Radiology
• Procedure Report Form From Radiology/Surgeon to Dialysis Clinic
• Recommended AVF Cannulation Recommended Protocol
• Use of Clamps on AVFs Recommended Protocol
• Secondary AVF Procedures “Sleeves Up Recommended Protocol”
• Local Medical Review Policy Related to Vascular Access
• List of Facilities with 40% AVF Rate and Associated Surgeon or
Surgical Group
• Physical Examination of the AVF Article
What We Have Learned From the
Project So Far!
•Without a Medical Director/Nephrologist taking an active role in
improving vascular access process, the facility will struggle and
patients may receive sub par care.
•You must have access to one or more surgeons with the experience,
willingness & tenacity to place AVFs in appropriate patients.
• Pre-surgery blood vessel mapping greatly improves the chances of
successful AVF placements.
• Early referral of patients for mapping and surgery improve AVF
placement opportunities.
What We Have Learned From the
Project So Far!
•Comprehensive cannulation training is a necessity
• Delegating a staff member to be responsible for monitoring access
rates and planned procedures is very helpful.
• Educate and motivate patients and their families that AVFs may
help keep them out of the hospital or worse
• Very complicated project!
“We have just begun to fight”
Planned initiatives formally begun in March/April 2004
Distribution of Resources
Distribution of Facility Specific Charts
Distribution of Surgeon Specific Charts
Surgeon Conferences
Nurse Conferences
Next Steps!
Continued
Nurse Educational Conferences/Awareness Campaign
Distributing charts and statewide report highlighting
benchmark facilities, county rates & facility distribution.
Highlighting names of surgeons associated with
“Benchmark” facilities
Distributing resource updates and reminders of
availability
Seeking opportunities to assist/support/encourage use of
Change Package strategies.
Next Steps!
•New
Seek input from EC, MRB, Committees
Market information on Revised Mapping Policy
Focus on largest cities (Houston, San Antonio)
Initiate “collaboratives” with LDOs to mentor laggard
facilities
Nephrologist seminar in Houston
Partnering/educating hospitals to review policy