3 Hour Training
advertisement

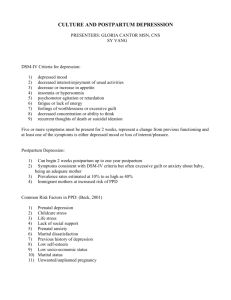
Perinatal Mood Disorders Michigan Statewide PMD Coalition 3 Hour Training Objectives: 1. 2. 3. 4. 5. Differentiate between the Symptoms of the 6 Perinatal Mood Disorders Describe at least 6 Risk Factors for Perinatal Mood Disorders Identify recommended Screening Measures for Perinatal Mood Disorders State at least 3 different Treatment Options for Perinatal Mood Disorders Describe Resources available to persons interested in Perinatal Mood Disorders 2 3 • Mary Taber-Lind, Photographer Introduction • 20% of WOMEN and 10% of MEN will experience clinical depression in their lifetime • PMD occurs in 10-20% of all new mothers who give birth • One out of every 7-8 mothers • 400,000 per year reported nation wide • An estimated 50% of cases go undetected •PMD knows NO boundaries: it affects all races, all ages, all professions, all economic status levels. Strong, intelligent women have PMD. • Often “Missed”: Misunderstood/misdiagnosed/mistreated •2003 Study- 86% of depressed pregnant mothers did not receive treatment (stigma, no screening, etc.) •Gotlib IH, Whiffen VE, Mount JH et al. J Consult Clin Psychol 1989:57:269 Prevalence rates assoc with depression in pregnancy and postpartum. • Brown, MA, Slochany JE. Nursin Clin North Am 2004:39:83 Two Overlooked Mood Disorders in Women •Marcus SM, Flynn HA, Blow FC, et al. Depressive symptoms among pregnant women screened in OB settings. J Womens Health 2003: 12:373 4 The Myth 5 The Reality 6 Epidemiology of Postpartum Episodes 70 Psychiatric Hospital Admissions per Month 60 50 40 30 20 Pregnancy 10 0 –2 Years – 1 Year Childbirth +1 Year +2 Years Kendell RE et al. Br J Psychiatry. 1987;150:662-673. 7 Professional Importance ■ Nursing: •AWHONN - Association of Women's Health, Obstetric and Neonatal Nurses Clinical Position Statement •Best Practice Guidelines - Registered Nurses Association of Ontario. Interventions for Postpartum Depression. www.rnao.org ■ Physicians: •American Academy of Family Physicians - 2006 National Congress of Student Members Resolution #206 adopted for PPD screening •American College of Obstetricians and Gynecologists – 2015 Clinical guidelines to screen once perinatal. •American Academy of Pediatrics – 2010 Established screening guidelines at well child appointments. 8 PMD Legislation ■ State of New Jersey - Senate Bill 2908 April 2006 - Signed by Governor Corzine Requires licensed HCPs to provide information and screening for PMD Required hospitals and birthing facilities to comply with screening and education Similar bills pending in other states ■ Federal Government - Melanie Blocker Stokes PPD Bill / Mothers ACT - PASSED 2010 Part of the Healthcare Reform. Allocates 3 Million for research, education and screening. ■ State of Michigan - Governor declared May 2010, 2015 as Postpartum Depression Awareness Month. Senate Resolutions declared in 2011,2012, 2013, 2014 9 Maternal Effects- Untreated PMD ■ Poor prenatal behaviors-nutrition, prenatal care, substance abuse ■ Poor parenting behaviors ■ Longer persistence of symptoms ■ Increased risk of PPD with subsequent children ■ Increased risk of relapse ■ Poor pregnancy outcomes: insufficient weight gain, decreased compliance with prenatal care, premature labor, small for gestational age infant • Muzik, M., Marcus, S., Heringhausen, J., Flynn, H. Primary Care: Clin in Office Practice 36:1:March 2009 Depression in childbearing women: When depression complicates pregnancy. 10 Effects on Maternal Attitude • • • 11 Guilt and anxiety about parenting Loss of love for baby Difficulty enjoying baby, negative or disinterested toward baby, less active interactions, inability or lack of attempt to soothe baby, refusal to look at or hold baby, hostile expressions •“I have spent the last 10 years of my career worrying about the impact of medications. I’ve been wrong. I should have been worrying more about the impact of the illness.” • Nuero Psychiatry Reviews, June 2001 12 What about the children? •“There is significant evidence that maternal depression can have a negative impact on the cognitive social and behavioral development of children, including infants and toddlers.” •Linda Chadron, MD, MS, Pediatrics in Review Vol. 24 No. 5 May 2003 13 Effects on Infant and Children ■ Poor mother-infant attachment Irritability, lethargic, poor sleep ■ Language delays ■ Behavioral difficulties ■ Lower cognitive performance ■ Mental health disorders ■ Attention problems ■ Withdrawn/fussy/crying/temper ■ Sleep/feeding/eating disruptions •Kahn, et al. AJPH 2002:92:1312-1318 •Infant Behav Dev 2004:27:216-229 •Psychiatry 2004:67:63-80 •Bonari et al. Can J Psychiatry 2004:49:726-735 14 Dads get Postpartum Depression too! • • • • • • • Virginia Medical School Study 5/10 28,000 New Dads screened - Meta Analysis of 43 published studies 10.4% Scored positive using standardized depression tools (EPDS, CES-D, BDI, etc.) Tx: Same as for Mom. Couples therapy. Meds. Self Help Local Resources: Dads Monthly Support group 4th Tuesday Websites: www.postpartumdads.org 10.40% www.postpartumdadsproject.org 89.60% www.postpartummen.com www.bootcampfornewdads.org PSI chat with Dads - First Monday each month at www.postpartum.net JAMA, Prenatal and Postpartum Depression in Fathers and its Association with Maternal Depression. A Meta-Analysis By James F. Paulson; Sharnail D. Bazemore 15 Mental illness during Pregnancy ■ Pregnancy is not protective ■ Prevalence: 9.4%-12.7% Prenatal Mental Illness 12.7% Wellness ■ Existing psychological disorders either stay the same or worsen during pregnancy (especially anxiety and OCD) ■ Women with mental illness during pregnancy have increased risk for Pre-term delivery, Cesarean Section, Low birth weight, NICU infants •2003 Study- 86% of depressed pregnant mothers did not receive treatment (stigma, no screening, etc) •Whitlock, American Journal of Psychiatry 2007 •Marcus SM, Flynn HA, Blow FC, et al. Depressive symptoms among pregnant women screened in OB settings. J Womens Health 2003: 12:373 16 “Whispers” Artprize 2015 Pam Coven 17 Video “Speak Up When You’re Down” New Jersey 2007 5 min Contact nancy.roberts@spectrumhealth for copies in English and Spanish Baby Blues Onset: First 2 – 3 weeks Prevalence: 50 – 80% Etiology • Hormones • Adjustment period Subsides in time with support Possible risk factor for PPD Symptoms • Crying, tearfulness • Fatigue • Mood swings • Anxiety 19 100 50 0 Baby Blues Withou t Blues Postpartum Depression Onset: Anytime in the first year Prevalence: 10 %– 21.9% PPD Prevalence PPD **Twice the rate of gestational diabetes and gestational hypertension- of which universal screening for both of these illnesses occurs routinely with ALL pregnancies Etiology: A biologic and life stressors illness Prognosis: Favorable with appropriate treatment Treatment: Meds, psychotherapy, support, self help 20 PMD Symptoms Depressive mood Sadness/crying Anxiety / insecurity Sleep disturbances Appetite changes Poor concentration Confusion Irritability Unable to take care of self /family 21 Numerous Losses, ie: self, spontaneity, body image, sexual, etc. Isolation Worthlessness Shame Guilt Anger “I finally told my husband that he and my daughter would be better off without me —that I was not a good mother or wife. I felt like things were never going to get better — that I would never feel happy again” “…I am going to act as though everything is fine although I am terrified of what lies ahead.” 22 Postpartum Panic/Anxiety Disorder Onset: first month Prevalence: 10-15% Etiology: unknown Treatment: meds, therapy, support 23 Symptoms: Panic attacks Anxiety Agitation Insomnia Self doubts Extreme worries Symptoms of Anxiety/Panic Attacks •Chest pain •Muscle tension •Shortness of breath •Hot and cold flashes •Tingling hands and feet •Extreme worries and fears •Fear of dying •Fear of going crazy •Fear of being alone 24 •Faintness •Irritability- anger and rage •Feeling trapped •Racing heartbeat •Hyperventilating/ Difficulty breathing •Nausea /Vomiting •Dizziness Postpartum Obsessive Compulsive Disorder Onset: first month Prevalence: unknown Etiology: unknown Treatment: meds, therapy, thought stopping techniques, support Intrusive thoughts, fears, images Person cannot control thoughts The person understands that to act on these thoughts would be wrong Often misdiagnosed as psychosis 25 OCD ■ Intrusive Thoughts: Recurring, persistent and disturbing thoughts, ideas or images (scary images of accidents, abuse, harm to self or baby) ■ Hyper vigilant (i.e. can’t sleep for fear that something awful will happen to baby, constantly checking on baby) ■ Ritual behaviors done to avoid harming baby ( put away knives) or to create protection for baby ( will not leave the house) 26 Post Traumatic Stress Disorder (PTSD) Due to Childbirth Onset: soon after birth Prevalence: 1.5%-6% Etiology: birth trauma, recent or past trauma Treatment: meds, counseling-debriefing, support 27 Re-experiencing over and over in one’s mind (sensations of “being in the trauma” now) Nightmares/Flashbacks Increased arousal/anxiety/anger Emotional numbing/detachment/ isolation During Delivery: 3 critical concepts ■ Offer good communication- allowing the mother to feel as much in control of the situation as possible. Fostering trust and offering choices when possible. Respect the mothers wishes, her dignity and privacy. Keep them well informed. ■ Provide pain relief- pain is a significant factor in trauma. Offer options for pain relief: Epidurals, meds, labor support, etc. ■ Provide comfort with the delivery room environment. 28 After Birth ■ Ask mother soon after birth if there is anything they want to know or talk about regarding their birthing experience. ■ Allowing expression of their perceptions and experiences of their birth and the care they received. ■ Websites and organizations: www.tabs.org.nz www.solaceformothers.org www.ptsdafterchildbirth.org 29 Bipolar Disorder •Often presents with Mania first: ■ Feels great ■ High energy ■ Irritability ■ Decreased need for sleep ■ Feeling “speedy” ■ Easily distracted ■ Mind racing ■ Fast speech 30 •85% of bipolar women who go off their medications during pregnancy will have a relapse before the end of their pregnancy . •Increased potential for development of psychotic symptoms. Postpartum Psychosis Onset: first 1 – 3 weeks ( months) Prevalence: 1 – 2 per 1000 births or 4,000 per year nationally Etiology: unknown – 70% have significant history of mental illness 5% commit suicide 4% infanticide Treatment: Inpatient hospitalization for close observation - a true psychiatric emergency Symptoms: • Delusions • Hallucinations • Paranoia • Loss of reality • Agitation • Irrational statements • Mania • Insomnia Spinelli MG. Am J Psychiatry. 2004;161:1548–1557 Spinelli MG. Am J Psychiatry. 2009;166(4):405-408. Nonacs R, Cohen LS. J Clin Psychiatry. 1998;59(Suppl 2):34-40 Jones I, Craddock N. Ann Med. 2001;33(4):248-256. 31 Risk Factors-Postpartum Psychosis • • • • • • • Risk factor Hospitalization for psychotic episode during the pregnancy......... Hospitalization for a psychotic episode prior to the pregnancy..... Any previous psychiatric hospitalization........................................ Previous hospitalization for bipolar mood episode......................... Baseline population risk ................................................................ Harlow BL. Arch Gen Psychiatry. 2007;64:42-48. 32 • • • • • Risk factor % that developed Postpartum Psychosis 44% 14.5% 9.2% 2.0% 0.07% “I heard voices while I was in the shower telling me I should go ahead and just kill myself.” “I thought the devil was living inside of me — that my children would be better in heaven with God than with me.” Andrea Yates 33 Differentiating between OCD and Psychotic Thoughts Postpartum OCD • Thoughts are ego-dystonic • Disturbed by thoughts • Avoid objects or being with baby • Very common disorder • Low risk of harm to baby OCD, obsessive-compulsive disorder Brandes M et al. Arch Womens Ment Health. 2004;7(2):99-110. Postpartum Psychosis • Thoughts are ego-syntonic • Rarely distressed by thoughts • Do not have avoidant behaviors • Not common disorder • High risk of harm to baby Etiology and Risk Factors • Biological • Psychological • Relationship 35 Biological Risk Factors All normal physical changes of pregnancy and childbirth Hormone changes Brain chemical changes Thyroid imbalance ( 5-10% during first postpartum year) Multiple Births (25%) Infertility Hx Family Hx of Mental Illness 36 Hx PMS- PMDD (premenstrual dysphoric disorder) Personal history of mental illness (3-4 times the risk) Hx prenatal depression (33%) Hx PPD (50-70%) Complicated pregnancy or delivery including PTSD Psychological Risk Factors Normal psychological changes that always occur with childbirth Unplanned pregnancy: ambivalence Expectations of motherhood Personality characteristics : “the perfectionist” Significant Lifestyle changes first time mothers Adoptive mothers not excluded 37 Unresolved losses: especially reproductive in nature: miscarriage, abortion,infertility, PP sterilization. Recent stresses: illness, divorce, move, job change, death, finances Negative childhood experiences : Hx abuse, neglect, PTSD Relationship Risk Factors Relationship with the significant other/partner/husband The “Quality “of the partnership Mothers social support system Single mothers at higher risk Quality of relationship with BABY High Need infant: ill, colic, NNICU Mothers relationship with OTHER children 38 Video “Healthy Mom, Happy Family” Postpartum Support International 13 min. Also in Spanish 2010 Assessment and Identification Early detection = Early intervention 40 Assessment • Observation: Use our training, experience, and intuition…. • Her speech? Demeanor? Self care? Interaction with others? • Care of infant: Attentiveness to needs? Interaction? Safety measures? • Input from Significant Other • History 41 Screening Recommendations: US Preventive Services Task Force • 2 Question Screener: (PHQ-2) •1. “During the past month have you been bothered by feeling down, depressed or hopeless?” •2. “During the past month, have you often been bothered by having little interest or pleasure in doing things that you previously enjoyed?” •*A window of opportunity exists for screening because this is the time of life when women are under the care of a healthcare provider and entering medical systems. 42 ACOG: Screening for PMD • May 2015 • ACOG (The American College of Obstetricians and Gynecologists) • New Committee Opinion Report Published! • Finally! • http://m.acog.org/Resources-And-Publications/CommitteeOpinions/Committee-on-Obstetric-Practice/Screening-forPerinatal-Depression?IsMobileSet=true • Replaces the Feb 2010 report 43 PMD Screening Tools ■ Edinburgh Postnatal Questionnaire (EPDS) by Cox ■ Postpartum Depression Screening Tool (PDSS) by Cheryl Beck Western Psychological Services 310-478-2061 www.wpspublish.com ■ Patient Health Questionnaire (PHQ-9) by Spitzer Linked to DSM- www.pfizer.com/phq-9 ■ Postpartum Depression Checklist (PDC) by C. Beck – Identifies 11 symptoms ■ Beck Depression Inventory (BDI) by A. Beck - 21 items, self report, 3 versions ■ Others for clinical depression: CES-D Center for Epidemiologic Studies/Depression MHI-5 Mental Health Inventory 44 Edinburgh Postnatal Depression Scale EPDS • Brief - 10 questions • Easily read and understandable - 6th grade reading level • Self administered : 2-4 minutes to complete • Published in 20 languages and used internationally • No cost - unless for electronic documentation • Can be used both prenatal or postpartum • Validated by research –Reliable Sensitivity: 78% Specificity 99% • In use since 1987 • Explores mood symptoms in PP period and less physical and somatic symptoms 45 Edinburgh Postnatal Depression Scale 46 Interpretation of the EPDS score ■ A score of 12 or more suggests further assessment for intervention to take place ■ Confirmation requires 2 consecutive scores of 12 or more separated by 2 weeks plus a professional interview/assessment. ■ Always intervene with #10 question if marked positive ■ Other Languages at: http://bit.ly/1xb0N4o 47 Research on EPDS Last Question • • • • 11% marked a score of 12 or more, of which 40% of these endorsed last question. 14% were on meds. 20% had prior suicide attempt. 8 % under care of a psychiatrist More frequently endorsed by non Caucasian with Asian /Hispanic highest 6 themes: 0.8% had an actual suicide plan 57% reporting fleeting thought of suicide but would never act on it 16% reported in past (not last 7 days) 10% denied marking last question when asked 2 % said it was marked by mistake 12% misunderstood the question (language barrier, a dream, etc) Kim, Jo. University of Chicago Pritzker School of Medicine, 2015 48 Diagnostics: DSM-V Criteria Uses same criteria as for non-pregnant. PPD is not listed as a separate diagnosis, however the DSM-V has a postpartum onset specifier within 4 weeks of delivery. (Although studies show onset can occur much later in the PP period) Five (or more) symptoms present in the same 2 week period: 1. Depressed mood most of the day 2. Diminished interest or pleasure in activities 3. Significant weight loss or weight gain 4. Insomnia or hypersomnia 5. Psychomotor agitation or retardation 6. Fatigue or loss of energy 7. Feelings of worthlessness or excessive guilt 8. Diminished ability to think or concentrate 9. Recurrent thoughts of death or suicidal ideation 49 Risk Assessment Screening Performed at many hospitals in Michigan using the Spectrum Health Postpartum Depression Risk Questionnaire. The self administered PMD Risk Questionnaire AND Edinburgh is completed by mother within first 12 hours after birth If High Risk - The staff/RN/MSW provides education, creates a PMD plan with patient and family, and initiates follow up screening and /or phone call. 35% Screen at High Risk at Spectrum Health. Other hospitals report similar findings. 50 Postpartum Depression Risk Questionnaire Key Questions to ask •“How are things a home?” •“Are you sleeping OK when the baby sleeps?” •“Any changes in your appetite?” •“Are you experiencing anxiety or panic?” •“Are you afraid to be alone with your baby?” •“Do you feel more irritable or angry than usual?” •“Are you afraid you might lose control?” •“Are you worried about the way you feel right now” •“Are you afraid of any thoughts you are having?” •“Does your partner know how you are feeling?” •“Do you ever have thoughts about hurting yourself or the baby?” •“Is there anything you are afraid to tell me but think I should know? 52 Red Flags: Mothers may reply… •“I have not slept at all in 48 hours or more” •“I have lost a lot of weight without trying to “ •“I do not feel loving towards my baby and can’t even go through the motions to take care of him/her” •“I feel like such a bad mother” •“I am afraid I might harm myself in order to escape this pain” •“I am afraid I might actually do something to hurt the baby” •“I hear sounds or voices when no one is around” •“I feel that my thoughts are not my own or that they are totally out of my control’ •“Maybe I should have never become a mother, I think I may have made a mistake” •Always use Clinical Judgement 53 Tips for Professional and Family ■ Do not assume that if she looks good, she is fine. ■ Do not assume this will get better on its own. ■ Do encourage her to get a comprehensive evaluation if you are concerned. ■ Do take her concerns seriously. ■ Do let her know you are available if she needs you and inform her of support resources for PPD. 54 Why don’t mothers seek treatment? “I never let others know how bad I felt. I was so afraid people would think I was crazy and take my baby away.” 55 PMD and Treatment •PMD Education •Family support •Social support / Support Groups • Self Help •Counseling / Therapy - Cognitive behavioral and Interpersonal therapy •Medications 56 Self-Care Treatment Options Education: Books, Journals, Videos, Websites, Resources Exercise “Activity or Movement” ( Yoga, Tai Chi, Stroller Exercises, etc) Sleep / Rest Nutrition (High protein, Limit sugar and caffeine) Vitamins (Prenatals, Vit. B Complex, Vit. D3, Omega 3 Fatty Acids) Social and Family Support Journaling Keep expectations realistic Postpone major life changes Prayer and Spiritual Healing 57 Other Treatment Options Hormonal replacement – Controversial - Estrogen/Progesterone creams, injections, etc Complementary Alternative Medicine (CAM) Treatment: Light Therapy, Massage Therapy, Infant massage, Hypnosis, Acupuncture, etc Mindfulness, Meditation, Relaxation, Stress Reduction Herbal -St Johns Wort ,SamE, etc Homeopathy, Naturopathy Placenta Ingestion TMS – Transcranial Magnetic Stimulation ECT – Electro Convulsive Therapy Barnes PM et al. Natl Health Stat Report. 2008;(12):1-23; Eisenberg DM et al.JAMA. 1998;280(18): 1569-1575; Nahin RL et al. Natl Health Stat Report. 2009;(18):1-14. 58 Psychotherapy Approaches Cognitive Behavioral Therapy (CBT) Thought or symptom based methods Interpersonal Psychotherapy (IPT) Grief, Role Transitions, Interpersonal Disputes, Interpersonal Deficits Couples Therapy Group Therapy EEG Biofeedback / EMDR Aaron Beck, Founder of CBT O’Hara, Interpersonal Psychotherapy Manual for PPD, 1993 59 PMD and Pharmacology • During Pregnancy • During Lactation • During postpartum without lactation 60 “There is no perfect decision, and no decision is risk free. Patients need to know about the risk of exposure to medications and they need to know about the risk of untreated disease.” Massachusetts General –Center for Women’s Mental HealthLee Cohen MD, Nuero Psychiatry Reviews June 2001 61 Two Choices: Risk/Benefit Analysis • Expose the baby/fetus to medication during pregnancy or lactation • Expose the baby/fetus to the adverse effects of untreated depression in the mother 62 Medication ■ Use the medication that Mom has taken in past with good results (if possible) ■ Start on lowest dosage and increase gradually every 5-7 days (if possible) ■ Use the safest medications possible (review the research and categories) ■ A plan of action needs discussion between patient and provider during the pregnancy for the upcoming year. ■ Most advise to continue meds 6-12 months after patient begins to feel better, then discontinue slowly as provider monitors. 63 Breastfeeding and PMD ■ Assessment of the mothers perception of the breastfeeding experience and her own expectations ■ It may be the ONLY thing that she feels good about ■ Do not tell her to automatically discontinue breastfeeding if taking meds ■ Give her permission to follow her instincts ■ Support the mother whatever her decision, to avoid guilt and shame ■ If SHE chooses to wean, do NOT let her wean abruptly (slowly over 2-3 weeks) 64 Considerations ■ Balance the benefits of breastfeeding with the risks of the drug ■ The risk/ benefit assessment is case-specific ■ Observe the infants behavior. Inform the Pediatrician. American Academy of Pediatrics Policy Statement 65 Medication Resources ■ Zachary Stowe, MD- Women's Mental Health Program, Emory University www.emorywomensprogram.org ■ Lee Cohen, MD-Center for Women’s Health, Massachusetts General Hospital www.womensmentalhealth.org ■ Thomas Hale, PhD. - “Medication and Mother’s Milk” www.iberastfeeding.com www.neonatal.ttuhsc.edu/lact ■ www.ibreastfeeding.com An online pharmacy subscription ■ www.motherrisk.org Valuable info about meds during pregnancy and lactation ■ Mother To Baby: Medications and More During Pregnancy and Breastfeeding OTIS: Organization of Teratology Information Specialists www.mothertobaby.org LactMed - www.toxnet.nim.nih.gov www.bmj.com/content/351/bmj.h3190 - SSRI safety study 66 Cultural Perspectives • • • • 67 One universal denominator: Social Support is THE most significant factor across all cultures Use of alternative words in lieu of “Depression and Anxiety” May use “stress” and “sadness”, etc instead All cultures have customs and traditions for families and women who give birth. Sometime barriers, such as distant family units, can lend to isolation difficulties for new mothers. Prognosis Excellent When…. the appropriate diagnosis and treatment occurs The sooner this occurs, the sooner mom recovers 68 PMD Resources •Referral Listings •Organizations •Websites •Books •Journals •Videos •Curriculums 69 Key PMD Organizations • Postpartum Support International (PSI) www.postpartum.net (805) 967-7636 • The Marce’ Society- International www.marcesociety.com 70 71 PSI Michigan Coordinators • West Michigan: Nancy Roberts - Spectrum Health and Pine Rest 616-391-1771 / 616-391-5000 nancy.roberts@spectrumhealth.org nancy.roberts@pinerest.org • South East Michigan: Kelly Ryan - Beaumont Hospital Parenting Program 248-898-3234 kelly.ryan@beaumont.org • Northeast Michigan: Shurkela Mason - Flint 810- 853- 9795 shurkelamason@yahoo.com • Southwest Michigan: Polly Vega – Battle Creek 269- 964-5868 vegap@trinity-health.org 72 Michigan PMD Support Groups Battle Creek (269) 964-5868 Phone support Bay City (989) 894-6980 Phone support Cadillac Mercy (231) 876-7277 Flint (810) 853-9795 Grand Rapids (616) 391-1771, (616) 391-5000 Grand Haven (616) 847-5512 Lansing (517) 363-8775 Muskegon (231) 773-6624 Traverse City (231) 947-2255 Detroit Area (586) 372-6120 Tree of Hope Foundation Sterling Heights, St. Clair Shores, Troy, Farmington Hills Zeeland (616) 741-3790 As of 2016-Subject to change 73 Pine Rest Mother and Baby Day Program • Grand Rapids • Partial Hospitalization Program- 9 am to 3 pm M-F • 68th St Pine Rest Main Campus - VanAndel Building • Pregnant and Postpartum up to 3 years postpartum • Voluntary Admission • Self Referral, Provider Referral, Agency Referral • Private Insurance and Medicaid accepted • Nursery and Nursery Attendant on site • Group and Individual PMD Therapy and Education • Psychiatrist Evaluation on Day 1 • Usual stay averages 5 days • Aftercare Discharge Plan and Phone follow up support Contact: 1-844-MOM-HOPE or 1-844-666-4673 www.pinerest.org/mother-baby-postpartum-depression-treatment 74 Pine Rest levels of care (*needs a trained clinician and can be difficult to assess) Outpatient Partial Inpatient Increased depressive or anxiety symptoms Loss of function in daily tasks, thoughts of not wanting to care for infant or be with infant Suicidal thoughts, can’t be safe without being with someone 24/7 Can function in work/daily living tasks Waiting for 1x a week therapy is not enough Psychosis (hearing voices, seeing things, feels everything is connected or has special mission) Meeting 1-2x a week with a therapist helps alleviate the stress Suicidal thoughts but no intent and has support system Loss of function, worsened anxiety or depression that affects ability to eat/sleep or function Michigan Statewide PMD Coalition • • • • • • • • 77 Founded 2013 www.mipmdcoalition.org PMD Providers listing in 10 regions Recruiting members- Currently 100 members Quarterly meetings Funding PMD projects Trainings/Education Goals Contact Information for Michigan Statewide PMD Coalition Nancy Roberts nancy.roberts@spectrum-health.org nancy.roberts@pinerest.org 616-391-2561 616-391-1771 Spectrum Health Healthier Communities 665 Seward Ave NW Grand Rapids, MI 49504 78 Other Michigan PMD Coalitions • Kent County - Healthy Kent 2020 Contact Barb Hawkins-Palmer barb.hawkins-palmer@kentcountymi.gov 616-632-7281 • Lakeshore PMD Coalition – Ottawa and Muskegon Co. Contact Laura Bronold lbronod@noch.org 616-847-5512 79 Program Development Toolkit for Perinatal Mood Disorders Step by Step process for organizations who wish to create a PMD program 55 distributed throughout US Contact nancy.roberts@spectrumhealth.org 616-391-1771 www.spectrumhealth.org/ppd-toolkit 80 Tree of Hope Foundation www.treeofhopefoundation.org Contact Pam Moffitt pmoffitt@treeofhopefoundation.org (586) 879-9374 Books- A few good choices • • • Postpartum Depression for Dummies – by Shoshanna Bennett. (2006) Pregnant on Prozac – Shoshanna Bennett. (2009) Beyond the Blues – A Guide to Understanding and Treating Prenatal and Postpartum Depression – by Shoshana Bennett, PhD., Pec Indman. (2005). Also in Spanish Therapy and the Postpartum Woman - Karen Kleinan. (2008) This Isn’t What I Expected – by Karen Kleinan, Valerie Raskin. (1994) Postpartum Survival Guide – by Ann Dunnewold, PhD , Diane G. Sanford, PhD. (1994) The Mother-to- Mother Postpartum Depression Support Book – by Sandra Poulin (2006) Postpartum Husband: Practical Solutions for Living with Postpartum Depression by Karen Kleinman, (2003) Women’s Moods – What Every Woman Must Know about Hormones, the Brain and Emotional Health – by Deb Sichel, MD , Jeanne Driscoll, MS, RN. (1999). What am I thinking? Having a Baby After Postpartum Depression – by Karen Kleiman. (2005) • • • • • • • 82 DVDs -A few good choices • Postpartum Depression: Speak up When You're Down – New Jersey 5 min 1-609-2924043 Recognizing and Treating Postpartum Depression: A Practitioner’s Guide – (2005) 44 min. www.Injoyvideos.com 1-800-326-2082 Healthy Mom, Happy Family – Postpartum Support International (2010) 13 min Also Spanish Postpartum Couples-Postpartum Mood Disorders: The Couple’s Experience – by Christina Hibbert (2002) 33 min www.postpartumcouples.com • • • 83 Professional books-A few good choices • Medications and Mothers Milk – by Dr. Thomas W. Hale. 12th edition (2010) • Perinatal Mental Health- A Guide to the Edinburgh Postnatal Depression Scale – by John Cox and Jeni Holden. (2003) Includes the scale in 20 languages • Postpartum Depression: A Comprehensive Approach for Nurses – by Kathleen A. Kendall-Tackett. (1993) • Postpartum Psychiatric Illness: A Picture Puzzle – by Dr. James Hamilton and Patricia Neel Harberger. (1992) • Screening for Perinatal Depression – by Henshaw and Elliott 84 (2005) Professional Contact Hours •www.step-ppd.com •www.nursingcenter.com/ceconnection •www.netCE.com •www.Ce4Less.com Independent Study for the book Therapy and the Postpartum Woman As of 2016-Subject to change 85 Spanish PMD Resources • www.postpartumdepressionhelp.com Beyond the Blues Mas Alla de la Melancolia, contiene la informacion mas reciente para las mujeres que sufren de problemas temperamentales y depresivos durante y despues del embarazo. www.perinatalweb.org Wisconsin Perinatal Foundation pamphlets www.noodlesoup.com “Rompiendo el Silencio” (Breaking the Silence) pamphlets Speak Up When You’re Down DVD- 5 min - Kent Co PMD Coalition Healthy Mom, Happy Family video – Postpartum.net www.inprf.org.mx.?es dificilser Mujer? Una guia sobre depresion Ma. Asuncon Lara Cantu ISBN 968-860-545-X www.state.nj.us Search Postpartum Depression New Jersey • • • • • • 86 86 References •Aditi Mehta, MD; Sandeep Sheth, MD; Postpartum Depression: How to Recognize and Treat This Common Condition Medscape Psychiatry& Mental Health, Expert Column, Posted 04/24/2006 •Altshuler 96, Andersson L et al. Am J Obstet Gynecol 2003; 189:148-152 •Bettes, B. A. (1988). Maternal Depression and Motherese: Temporal and Intonational Features. Child Development, 59, 10891096. •Bonari et al. Can J Psychiatry 2004; 49(11): 726-35; •Breznitz, Z., & Friedman, S. L. (1988). Toddlers' Concentration: Does Maternal Depression Make A Difference? J. Child. Psychol. Psychiat., 29(3), 267-279. •Campbell, S. B., Cohn, J. F., & Meyers, T. (1995). Depression in First-Time Mothers: Mother-Infant Interaction and Depression Chronicity. Developmental Psychobiology, 31(3), 349-357. •Chrousos, G. P., & Gold, P. W. (1992). The concepts of stress and stress system disordres, overview of psysical and behavioral homeostasis. JAMA, 267(9), 1244-1252. •Chaudron, et al.; Detection of Postpartum Depressive Symptoms by Screening at Well-Child Visits, PEDIATRICS Vol. 113 No. 3 March 2004, pp. 551-558 •Cohen LS, et al. CNS Spectr 2004; 9:298-16; •Cohen et al, JAMA 2006 295(5) 499-507; •Corral, et al.; Am J Psychiatry 157:303-304, February 2000, Bright Light Therapy’s Effect on Postpartum Depression •Cox, J.L., et al. Detection of postnatal depression: development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry. 1987; 150:782-786. •Dawson, G., Frey, K., Panagiotides, H., Yamada, E., Hessl, D., & Osterling, J. (1999). Infants of depressed mothers exhibit atypical frontal electrical brain activity during interactions with mother and with a familiar nondepressed adult. Child Development, 70(5), 1058-1066. •Dawson, G., Frey, K., Self, J., Panagiotides, H., Hessl, D., Yamada, E., & Rinaldi, J. (1999). Frontal brain electical activity in infants of depressed and nondepressed mothers: Rrelation to variations in infant behavior. Development and Psychopathology, 11, 589-605. 87 References (cont.) •Einarson A., et al. J Psychiatry Neuroscience 2001; 26:44-48 •Field et al. Depression & Anxiety 2003;17(3): 140-15; •Field, T., Pickens, J., Fox, N., Nawrocki, T., & Gonzalez, J. (1995). Vagal tone in infants of depressed mothers. Development and Psychopathology, 7, 227-231. •Field, T., Healy, B., Goldstein, S., & Guthertz, M. (1990). Behavior-State Matching and Synchrony in Mother-Infant Interactions of Nondepressed Versus Depressed Dyads. Developmental Psychology, 26(1), 7-14.Francis & Meaney, 1999 •Gjerdingen, Dwenda, The Effectiveness of Various Postpartum Depression Treatments and the Impact of Antidepressant Drugs on Nursing Infants. Journal of the American Board of Family Practice, 2004 •Goldsmith, D. F., & Rogoff, B. (1997). Mothers' and Toddlers' Coordinated Joint Focus of Attention: Variations with Maternal Dysphoric Symptoms. Developmental Psychology, 33(1), 113-119. •Honikman, Jane; I'm Listening: A Guide to Supporting Postpartum Families, Postpartum Support International •Hostetter, et al. Biol Psychiatry 2000; 48:1032-34; •Jones, N. A., Field, T., Davalos, M., & Pickens, J. (1997). EEG stability in infants/children of depressed mothers. Child Psychiatry and Human Development, 28(2), 59-70. •Jones, N. A., Field, T., Fox, N. A., Lundy, B. L., & Davalos, M. (1997). EEG activation in 1-month-old infants of depressed mothers. Development and psychopathology, 9, 491-505. •Kendell RE et al. Br J Psychiatry. 1987;150:662-673 •Kim et al. Br J Clin Pharmacol. 2006; 61 (2): 155-63 •Llewellyn 97 •Logsdon DNS, Social Support to Childbearing Women: What Are the Rules?, ARNP Journal of Obstetric, Gynecologic, Neonatal Nursing Vol. 34 Issue 6 Page 754 November 2005; •Logsdon, M.C. (2000). Social Support for Pregnant and Postpartum Women. AWHONN •Marcus SM et al. J Womens Health 2003; 12:373-80; •Milberger, S., Biederman, J., Faraone, S. V., Chen, L., & Jones, J. (1996). Is maternal smoking during pregnancy a risk factor for attention deficit hyperactivity disorder in children? american Journal of Psychiatry, 153, 1138-1142. 88 References (cont.) •Monk, C. (2001). Stress and Mood Disorders During Pregnancy: Implications for Child Development. Psychiatric Quarterly, 72(4), 347-357.Moses-Kolko EL et al. JAMA 2005; 293: 2372-2383 •O’Connor et al. Br J Psychiatry 2002; 80: 502-8 •O’Connor et al. J Child Psychol Psychiatry 2003; 44(7): 1025-36 •Olds,D., Robinson,J., O'Brien,R., Luckey,D., Pettit,L., Henderson,C., Ng,R., Sheff,K., Korfmacher,J., Hiatt,S. & Talmi,A. (2002) Home Visiting by Paraprofessionals and by Nurses: A Randomized, Controlled Trial •Orr ST et al. Pediatric & Perinatal Epidemiology 2000; 14:309-13 •Porges, S. W. (1992). Vagal Tone: A Physiological marker of Stress Vulnerability. Pediatrics, 90(3), 498-504. •Portales, A. L., Roosevelt, J. A., Lee, H. B., & Porges, S. W. (1992). Infant Vagal tone predicts 3 year child behavior problems. Infant Behavior & Development, 15, 636. •Stein, A., Gath, D. H., Bucher, J., Bond, A., Day, A., & Cooper, P. J. (1991). The Relationship between Post-natal Depression and Mother-Child Interaction. British Journal of Psychiatry, 158, 46-52. •Stewart DE. CMAJ 2006; 174(3):302-303; •Teixeira Fisk & Glover. BMJ 1999; 318(7177): 153-7; •Van den Bergh et al. Neuroscience & Biobehavioral Reviews 2005; 29(2): 237-58 •Van Den Bergh et al. Neurosci Biobehav Rev 2005; 29(2): 237-58. •Van Den Bergh & Marcoen. Child Dev 2004 Jul-Aug;75(4):1085-97. •Wadhwa, P. D., Sandman, C. A., & Garite, T. A. (2001). The neurobiology of stress in human pregnancy: implications for prematurity and development of the fetal central nervous system. In J. A. Russell (Ed.), Progress in Brain Research (Vol. 133, pp. 131-142): Elsevier Science. •Wisner KL, Gelenberg AJ, Leonard H, Zarin D, Frank E. Pharmacologic treatment of depression during pregnancy.JAMA. 1999 Oct 6;282(13):1264-9. Review.17. •Wisner KL, Findling RL, Perel JM. Paroxetine in breast milk. Am J Psychiatry. 2001 Jan;158(1):144-5. No abstract available.18. •Wisner KL, Zarin DA, Holmboe ES, Appelbaum PS, Gelenberg AJ, Leonard HL, Frank E. Risk-benefit decision making for treatment of depression during pregnancy. Am J Psychiatry. 2000 Dec;157(12):1933-40. 89 A Challenge to Participants Health Care Providers Office nurse Childbirth educator Labor and delivery nurse Mother-baby nurse Neonatal nurse Lactation consultants Medical social worker - Care management Home visiting nurse Help line telephone nurse All Others… 90 YOU can make a difference! 91