Choose to Admit/Transfer to Assess
advertisement

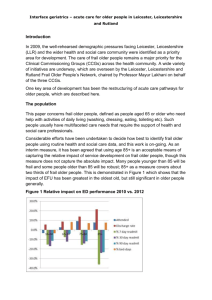
Frail Older People Programme Greater Nottingham Jeremy Griffiths Clinical Lead / Chair of SIGNS 30th October 2013 Greater Nottingham approach • Frail Older People – how we started • Learning from others - Warwick - Jan 2013 • What we have done since Who are we? • • • • • 4 CCGs 2 Local Authorities Nottingham University Hospital 2 community providers Nottinghamshire Healthcare Trust How we started August – November 2012 • Mandate from an existing health and social care senior leaders forum (Productive Notts) • Drawing on the evidence base – Comprehensive Geriatric Assessment (CGA) – Enhance intermediate care • Engagement with main clinical groups across acute and community • Event of 80 staff to determine priorities Learning from visit to South Warwickshire January 2013 • Snappy titles – Support to Thrive/Choose to Admit/ Transfer to Assess – 5 a day challenge –became 7 a day for us • Impact of ageing population on demand for services • Providers working together The Burning Platform – the impact of our ageing population To avoid opening more beds in 2013/14 and 2014/15 we need to reduce admissions by 9% per annum How we continued January – October 2013 • High level communication (H and WB), including ambition for older people • Time based standards against the bow tie • Focus on Choose to Admit/Transfer to Assess in 4 projects • Understanding our patients and where we currently cannot meet their needs in the community • Implementation of phase 1 on October 14th Our ambition for older people • I wish to retain my independence wherever possible • When I am unwell, I am assessed using Comprehensive (Geriatric) Assessment • Community services are there for me if I need support at home or overnight • Hospital is there for me if I I need specialist clinicians to manage my medical conditions until I am stabilised, or I need an operation • I leave hospital as soon as my health is stable enough for me to do so • I see a specialist in medicine for older people if this is needed • Staff on my ward organise what is needed for me to leave hospital • I will only be transferred to long term care or a nursing home if that is the best place to meet my needs • While I am recovering, my care is planned using Comprehensive (Geriatric) Assessment All standards and timings are for discussion and development Draft V2.1 Frail Elderly Pathway – Care standards (time based) Self care Support older people at home Enhanced support at home Manage Crisis Effectively Input in acute setting Manage step down from acute effectivel y Enhanced support at home Support older people at Home Self care All standards relate to patients assessed as being ‘frail’ Home/care home Std H1. All patients remotely identified as an emerging risk (by e.g. the Devon tool) will be assessed* within 7 days Std H2. Primary care will respond to a request for a GP visit and make a ‘treat/refer/admit /no action’ decision within 4 hrs Crisis Acute Std C1. For all patients identified as being at risk of admission to an acute hospital, an assessment *will be initiated within 2 hrs of the request Std C2. All patients in crisis will start to receive a package of enhanced support at home within 2 hrs of the need being identified. NB working patterns Std C3. Within XX hrs of the need being identified for a Community bed, all patients in crisis will be transferred to that bed Std A1. On arrival in ED / admissions unit, all elderly patients at risk of adverse outcomes will be ISAR scored within 4 hrs . Std A2. Patients with an ISAR score of 3 or more will be notified to the CGA case manager and assessed*within XX hrs Std A3. All patients in hospital will be assessed* before they leave hospital. HOLD pending D2A discussions Trf of care Std T1. All patients will be transferred to the most appropriate care setting following a decision of ‘medically fit for discharge’ as follows: T1a. For first time care home placement: Arrival by 17.00 within XX days of the decision T1b. For return to care home: Arrival by 21.00 if decision by 14.00. By 12.00 next day if decision after 14.00 T1c. For assessment bed / I.C. bed: Arrival within 24 hrs between 10.00 and 16.00 Home/care home Standards to be developed Self care * All assessments are carried out using a Comprehensive Geriatric Assessment (CGA) approach 6 Strategic Priorities aligned to ‘levels of care’ SCOPES Support to Thrive Support to Thrive (planned care only) Choose to Admit Transfer to Assess Comprehensive Geriatric Assessment (CGA) Pathway Standards - time based Enabling sub groups - Outcomes & Commissioning, Communications & Consultation, Workforce Planning Enabling approach - SHARING of information, risks, challenges, successes etc. will be key Transfer to Assess Our approach • Simplify the interface between NUH and community services (including social care) on transfer of care out of NUH • Transfer patients out of acute hospital as soon as their acute needs have been met. Those patients who need time for further recovery are assessed in a community setting for longer term plans about their ongoing care. • Increase the capacity of community services to meet all needs without referral criteria Who are our patients? The ‘oldest old’, physically, cognitively or socially frail (Silver Book) Patients admitted to a HCOP ward until they transfer out of HCOP ward Half of the patients are over 85 88% have dementia, delirium or other mental health problems (excluding anxiety). Half of these have moderate to severe mental health problems Capacity modelling Commissioners and providers worked together to undertake detailed analysis and modelling using 2012 activity figures to show that……. There are 38 patients in beds in NUH who could be elsewhere This equates to 7 additional discharges a day and an average reduction in delays of 5 days per patient Capacity modelling We agreed some assumptions about what would additional capacity would be needed in the community to enable those patients to go home sooner We need 21 more community beds and 22 more community places But they need to meet the needs of patients who currently have no community provision – frail, clinically unstable older people with dementia/delirium. This may be why we have empty community beds Choose to Admit and Transfer to Assess projects Patient Information exchange including Alerts 3.Community 2.Community capacity Hubs 1.Care co-ordination team (underpinned by NUH’s – flow, streaming, discharge project) 4. CGA / information sharing 4. CGA / information sharing 2.Community 3.Community Hubs capacity 4. CGA / information sharing Choose to Admit/Transfer to Assess Planned deliverables By 1st Oct 2013 Care Coordination Team Current resources working as one team to support ED, ass beds and 8 HCOP wards (14th October) Community Hubs CCG-based community hubs established with access to a clinician with streamlined interface to Care Co-Ordination Team Community capacity CGA and information sharing An additional 6 beds that are staffed to meet the needs of the most complex patients as part of an integrated community service Standardised transfer of care template used to share information on needs between NUH and community hub (fax) By 1st Dec 2013 tbc 17th Sept 2013 By March 2014 Establish single integrated Care Coordination Team to support Choose to Admit and Transfer to Assess, reconfiguring existing resources, to case manage all ‘supported transfers’ Community hubs manage all health and social care local service capacity and organise packages of care to support transfer from hospital within 24 hours Total of 21 additional beds that are staffed to meet the needs of the most complex patients as part of an integrated community service Transfer of care template operating electronically on SystmOne Strategic decision on the future provision of community based services – including balance between bed and home based services Agree and implement a method of recording and sharing CGA across primary care, social care, NUH and community services Back to time based standards….. Crisis 2 hour standard Transfer of care 2 hour and 24 hour standard Where next? • Monitor changes – do they work and what is the impact on flow through acute and community services? • Work towards March deliverables • Benefits/financial analysis to understand impact on commissioners, providers and social care • Agree strategy beyond March