Including Health Care Homes
advertisement

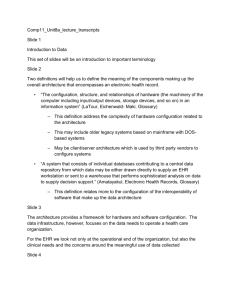
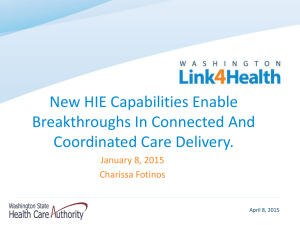
Section 1.1 Adopt – Assess Visioning and Strategic Planning— Including Health Care Homes (See accompanying Webinar and PowerPoint handouts) Health information technology (HIT) refers to the broad class of information technology that aids health care organizations in achieving efficient and effective care delivery. Electronic health record (EHR) system refers to the specific application of HIT to capture data at the point of care and use it in making clinical decisions. All HIT encompasses software applications and hardware, as well as requisite people, policies, and processes. Many clinics already have a practice management system (PMS). Some are able to connect with laboratories, imaging centers, hospitals, and other sources of clinical data. An increasing number of providers have started using standalone e-prescribing. In some cases, the sources of clinical data may be merely fax, email, or print files that can be downloaded from a provider portal. Practice guidelines and other evidence-based medical research data frequently are in paper form or images retrieved from the Web. Data from all of these sources—including data you generate about patients—needs to be available in a manner that allows computer software to process it into useful information. Minnesota Health Care Homes Providers can use the functions and capabilities of their EHR system to help deliver care as a health care home. A health care home (HCH), also known as a medical home, is an approach to health care in which primary care providers, families, and patients work in partnership to improve health outcomes and quality of life. To be certified as a health care home in Minnesota, the Minnesota Department of Health requires clinics to meet criteria related to the five following standards: Access and communication: Facilitate consistent communication among the HCH, the patient and family (“participant”), and other providers to provide the participant with continuous access to their HCH. Participant registry and tracking participant care activity: Use an electronic, searchable registry that enables the HCH to identify gaps in patient care and manage health care services. Care coordination: Include care coordination that focuses on patient and family-centered care. Care plan: Include a care plan for selected patients with a chronic or complex condition that involves the patient and the patient’s family in care planning. Performance reporting and quality improvement: Reflect continuous improvement in the quality of the patient’s experience, health outcomes, and cost-effectiveness of services. As you plan your EHR selection, consider the capabilities and functions that support the health care home standards, including: Storing and retrieving patient information, both clinical and other pertinent information (i.e., cultural background, racial heritage, primary language, values, beliefs, and preferred method of communication). Leveraging communication and interoperability capabilities to facilitate care coordination between the patient, the patient’s family, other providers involved in the patient’s care and other organizations (pharmacies, testing labs, etc.). Section 1.1 Adopt – Assess – Visioning and Strategic Planning, Including Health Care Homes - 1 Using data to develop individualized care plans that guide and educate patients and their families about the risks, benefits, and likely outcomes of available health care options. Demonstrating data reporting and analysis capabilities that enable performance reporting and tracking of key quality metrics. Computing Components that Comprise an EHR When acquiring an EHR, what you are actually getting is a special kind of database, called a clinical data repository, and software to enable you to capture, retrieve, and have the data processed with evidence-based guidance. Depending on what other information systems or sources of data you may have, you may need interfaces or other tools to help you retrieve the data and put it into the repository. Some of the data that go into the repository will be discrete, or structured, data, meaning each data variable is selected by the clinician to represent clinical findings. These data are encoded by the computer and able to be processed using clinical decision support software. Other data may come to you as digital images of documents, print files, voice files, email, fax, Web pages, and clinical pictures from picture archiving and communication systems (PACS). These images or parts of images can be retrieved for viewing (or listening) and can have electronic signatures appended to them, but individual data recorded in them generally are not able to be processed. The computer cannot create a graph of lab results directly from print files or perform drug-lab checking or other clinical decision support processing on images of documents. The goal of most EHRs is to capture as much discrete data as possible. Entering data via templates at the point of care directly supplies the reminders and alerts that create the value in using EHRs. Data Processing in an EHR Data must also be archived, so storage functionality is part of what is acquired through an EHR. As the EHR becomes a mission critical system with no backup dictation files or printed copies of documents that are filed, you not only need to have back up storage, but redundant processing as well. Some clinics invest in dual processing or mirrored servers to reduce the risk of downtime. Various input devices, network hardware and software, and other equipment are also part of an EHR. Finally, some means to generate special reports is needed. Many EHRs come with report writer software, but this software is generally used to process relatively small amounts of data into a report, such as how many patients need to be called this month for follow-up visits, or which patients received a specific medication that is now being recalled. For more sophisticated analysis of large amounts of data in your EHR, you may need a different kind of database, called a clinical data warehouse. Data from the clinical data repository are extracted and placed into the warehouse for analysis. This type of database has been optimized for performing data mining and special other kinds of analysis. Because it is separate from the clinical data repository used for day-to-day clinical transactions, organizations experience no degradation of performance on the daily functioning of the EHR when a warehouse is used. Section 1.1 Adopt – Assess – Visioning and Strategic Planning, Including Health Care Homes - 2 Conceptual Model of EHR The following diagram illustrates the components of an EHR system: Software Applications The term HIT covers many types of information system applications. In general, these include: 1. Financial and administrative systems include at a minimum, patient registration-admission, discharge, transfer (R-ADT) and billing systems. R-ADT includes the ability to maintain an index to all patients you have treated; document their demographic, contact, and insurance information; and manage the census of current patients, and other associated functions. Billing systems will support charge capture, accounts receivable, collections, general ledger, accounts payable, etc. 2. Clinical information systems support health care professionals in direct care delivery. When these clinical systems work together, they are often described as an electronic health record system. Clinical information systems in clinics may be all inclusive in a single suite of functions or may be several distinct modules, which may not necessarily be implemented in a specific sequence. A suite of applications for documentation may include assessments, clinical pathways, vital signs documentation, and workflow support. More sophisticated clinical systems typically include computerized provider order entry (CPOE) Although clinical decision support (CDS) is generally included in CPOE applications as relating to medication management, more sophisticated CDS and point-of-care (POC) charting are applications that frequently are implemented after most others. Many of the more sophisticated systems depend on connectivity with administrative systems and with external sources of information. For example, scheduling and other alerts may impact CPOE; lab results and other information may need to come from a lab, hospital, another provider office, durable medical equipment supplier, etc. Section 1.1 Adopt – Assess – Visioning and Strategic Planning, Including Health Care Homes - 3 3. Clinical data repository (CDR) is the means by which data from the various applications come together for processing into clinical decision support. A CDR is essentially a database that is optimized to manage transactions for a given patient. For example, a CDR may enable developing a graph showing a patient’s vital signs in comparison to the administration of a new medication. 4. Clinical decision support is greatly enabled by a CDR. For example, when a nurse goes to administer a drug for a given patient, the ordered drug is compared with drug knowledge information and the patient’s lab results. (The patient’s lab results have been entered into the CDR by the laboratory information system.) If the drug being ordered is contraindicated for poor liver function and if the lab results for the specific patient for whom the drug is ordered indicate poor liver function, an alert will display stating a potential contraindication. The nurse would then need to take appropriate action to have the drug order changed. Some EHR vendors fully integrate their clinical components with a data repository. Some clinics acquire all their applications from a single vendor that provides a well-integrated solution. If you have to buy different applications from different vendors, you will lack such strong integration. In this case, you may find you will need to manage multiple interfaces between the applications. You can buy a separate clinical data repository into which all data from the disparate applications can be directed. Although a clinical data repository is primarily designed to integrate discrete data, repositories can also include pointers to documents and images. 5. Electronic document management system (EDMS) is often used where a bridging strategy is needed to achieve a paperless environment during the time clinical systems are being implemented. EDMS allows document scanning and indexing to archive documents until all data collection aspects of the health record are automated. Later EDMS supplements the EHR when external documents are received in paper or digital form (e.g., email, e-fax, or digital dictation). 6. Portals are another important application to connect different providers to one another, such as physicians to an area hospital or your clinic to various community resources, contractors, etc. In general, a portal is a Web interface that serves as a secure door to related sets of data and services. For example, a physician from another office location may gain access to the clinic’s EHR and obtain patient vital signs and sign orders. Patient portals allow a patient or family member to complete intake forms and perform other functions, including potentially managing a personal health record (PHR). Most recently, point-to-point portals are beginning to be replaced by health information exchange (HIE) services. 7. Data warehouse is also a database, but one that has been optimized to collect and manage data on which complex queries and analysis, such as data mining, can be performed. Such databases may also be called translational or analytical databases. While you can do some analysis and reporting from any database, including the databases in individual applications or the CDR, very complex analyses on large quantities of data will significantly slow down the system in performing its operations. Most health care organizations contribute data to external data warehouses, such those as held by the Centers for Medicare & Medicaid Services (CMS), their corporation, or various other payers, quality registries, etc. 8. Telehealth, personal health records, and health information exchange services are yet other forms of HIT which are rapidly evolving and being adopted by large and small health care delivery organizations. Clinics can use such services for remote reading of x-rays. Many small and rural communities have extensive telehealth implementations, connecting to their closest tertiary care facility or to reach out to very remote areas for patient monitoring and to supplement care delivery. Some clinics may already be using a form of telehealth to connect Section 1.1 Adopt – Assess – Visioning and Strategic Planning, Including Health Care Homes - 4 personnel in the field with a base station. Home health agencies will certainly find using a referral management system that reaches out to a variety of other organizations to be advantageous. PHRs are just starting to be recognized as important adjuncts to health care delivery. CMS is developing a PHR system for Medicare beneficiaries to keep track of their medications. Several health plans (including a number of Blue Cross Blue Shield plans) also are doing this. The US Department of Veterans Affairs has created myHealtheVet, a PHR system for veterans. Some vendors are supplying various forms of PHRs, from client-friendly summaries of care to access to lab results and even self-administered medical history systems that reduce the documentation burden for providers. Many families of chronically ill clients or elderly clients in nursing homes find that PHR is the only way they can keep track of all the medications, physician visits, etc. 9. Middleware is a final type of software that is important to include in HIT. While often not a concern to end users, various report writing applications, presentation layer utilities, interfaces, database management systems, and other software is required to make all of the end-user applications work. Hardware Information system applications require computer hardware. Hardware includes the various processing devices and servers to run the applications. If you are using a hosted application, application service provider (ASP), software as a service (SaaS), or an on-demand application, you will not need to acquire servers in house. In these cases the vendor maintains these and you pay a monthly fee for their use. Data entry requires various input devices (e.g., desktop computers, tablets, personal data assistants [PDAs], speech microphones, etc.) and output devices (monitors, display screens, printers, fax machines, speakers, etc.). They are all hardware elements you will need to purchase. Data also must be archived, so storage functionality is needed. This may be part of your remote hosting or something you need in-house. This may include various forms of storage devices, each with their associated media (such as magnetic disks, optical disks, flash drives, etc.). Various storage area networks and storage management systems are used to manage large volumes of archived data. As the HIT becomes more mission critical, backup storage and redundant processing devices are necessary, often with middleware applications to provide automatic failover. All of these devices must connect to one another in a network, so various network devices and their associated media (including various forms of cable for wired networks and wireless network capability) must be acquired and maintained. A clinic’s network capabilities are critical in order to connect with all staff working remotely. You must have sufficient speed and bandwidth, and have some form of redundancy and backup capability, in the event your primary network connection fails. Conceptual Model of HIT and EHR Technology The diagram below illustrates the many HIT components described. While this diagram may seem overwhelming, recognize that as clinical computing requirements are addressed, the complexity of applications, technology, and operational elements to support them increase in complexity, as do the capabilities for use of the resultant information and knowledge. Section 1.1 Adopt – Assess – Visioning and Strategic Planning, Including Health Care Homes - 5 More information on health care homes is available at http://www.health.state.mn.us/healthreform/homes/index.html. This tool was adapted from the Health Information Technology Toolkit for Physician Offices by Stratis Health through a contract with the Minnesota Academy of Pediatric Foundation, for the Minnesota Department of Health (MDH) Health Care Home Resources and Education Project. The full Health Information Technology Toolkit for Physician Offices is available at http://www.stratishealth.org/HIT_Toolkit_clinics. Copyright © 2010, Margret\A Consulting, LLC. Used with permission of author. For support using the toolkit Stratis Health Health Information Technology Services 952-854-3306 info@stratishealth.org www.stratishealth.org Section 1.1 Adopt – Assess – Visioning and Strategic Planning, Including Health Care Homes - 6