VOLUME 4 • NUMBER 3 • SEPTEMBER 2012
OF PRIMARY HEALTH CARE
‘It is not possible to
divorce the practice
of medicine from the
society in which it is
practised.’
See page 223
Original Scientific Paper
Calculating cardiovascular risk in
people with Type 2 diabetes
See page 181
Original Scientific Paper
Pre-calling babies to improve
immunisation timeliness
See page 189
Original Scientific Paper
PSA testing in asymptomatic males
See page 199
Original Scientific Paper
Acute otitis media in the under-fives
See page 205
Original Scientific Paper
Brief mental health intervention
for Maori
See page 231
Viewpoint
The platform model of pain
management
See page 254
CONTENTS
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012
ISSN 1172-6164 (Print)
ISSN 1172-6156 (Online)
OF PRIMARY HEALTH CARE
178Editorials
231
From the Editor
178
Guest Editorial
180
Fiona Mathieson, Kara Mihaere, Sunny Collings, Anthony Dowell,
James Stanley
A practical issue
Felicity Goodyear-Smith
Maori cultural adaptation of a brief mental health
intervention in primary care
Short Report
239
Commentary: risk prediction models for people with Type 2
diabetes
The anatomical placement of body organs by Australian and
New Zealand patients and health professionals in general
practice
Marjan Kljakovic, Jo Risk
Kamlesh Khunti
Improving Performance
181 Original Scientific Papers
242
Quantitative Research
181
New Zealand Diabetes Cohort Study cardiovascular risk
score for people with Type 2 diabetes: validation in the
PREDICT cohort
Tom Robinson, C Raina Elley, Sue Wells, Elizabeth Robinson,
Tim Kenealy, Romana Pylypchuk, Dale Bramley, Bruce Arroll,
Sue Crengle, Tania Riddell, Shanthi Ameratunga, Patricia Metcalf,
Paul Drury
189
Early connections: effectiveness of a pre-call intervention to
improve immunisation coverage and timeliness
Felicity Goodyear-Smith, Cameron Grant, Tracey Poole, Helen
Petousis-Harris, Nikki Turner, Rafael Perera, Anthony Harnden
199
205
The incidence of acute otitis media in New Zealand children
under five years of age in the primary care setting
Barry Gribben, Lesley Salkeld, Simon Hoare, Hannah Jones
213
Sally Abel, Bob Marshall, Donny Riki, Tania Luscombe
249 Continuing Professional Development
249
Does the order of presentation and number of online
resources affect the frequency of access by learners?
Steven Lillis, Samantha Murton
Bruce Arroll
249
String of PEARLS about musculoskeletal conditions
250
Vaikoloa: Hearing loss among Pacific peoples
Ofa Dewes
251
Addressing patient alcohol use: a view from general practice
Thomas Mules; Jennifer Taylor; Rachel Price; Logan Walker; Baneet
Singh; Patrick Newsam; Thenmoli Palaniyappan; Toby Snook;
Mahfuzah Ruselan; John Ryan; Jaishree Santhirasegaran; Phoebe
Shearman; Petronella Watson; Richard Zino; Louise Signal; Geoff
Fougere; Helen Moriarty; Gabrielle Jenkin
Mixed Method Research
223
Factors influencing diagnostic decision-making
Kathleen Callaghan
Potion or Poison? Colloidal silver David Woods
253
Nuggets of Knowledge: Statins and memory loss
Linda Bryant
254Viewpoint
254
From ladder to platform: a new concept for pain management
Lawrence Leung
259
Frequently asked questions on measurement of bone mineral
densitometry
Joseph Lee, Nelson Loh
Qualitative Research
217
Cochrane Corner: Topical antibiotics are probably better than
placebo for acute conjunctivitis but most get better anyway
PSA testing in general practice
Fraser Hodgson, Zuzana Obertová, Charis Brown, Ross Lawrenson
Evaluation of Tu Meke PHO’s Wairua Tangata Programme:
a primary mental health initiative for underserved
communities
262 Letters to the Editor
263 Film Review
263
A good death: a film about end-of-life care and advance care
planning—produced by Prof. D Robin Taylor and Paul
Trotman
Reviewed by Prof. Rod MacLeod
264 About the Journal of Primary Health Care
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE177
EDITORIALS
FROM THE EDITOR
A practical issue
Felicity GoodyearSmith MBChB, MD,
FRNZCGP, Editor
J PRIM HEALTH CARE
2012;4(3):178–179.
CORRESPONDENCE TO:
Felicity Goodyear-Smith
Professor and Goodfellow
Postgraduate Chair,
Department of General
Practice and Primary
Health Care, The
University of Auckland,
PB 92019 Auckland,
New Zealand
f.goodyear-smith@
auckland.ac.nz
178
T
his issue has a wide range of research on a
variety of topics, but the common thread is
that these studies address practical issues
relevant to New Zealand primary health care.
The lead paper by Robinson et al. reports on the
locally developed PREDICT-based risk model
which is more accurate in predicting cardiovascular risk than the adjusted Framingham equation.1
In his accompanying commentary, Dr Kamlesh
Khunti, Professor of Primary Care Diabetes and
Vascular Medicine at the University of Leicester,
points to the need for studies on the impact of
use of risk prediction models with outcomes such
as patient adherence to medication or increased
understanding before the use of these models
becomes routine practice.2
A study of routine pre-call of infants at four
weeks to alert parents to the need to present
their babies to general practice at six weeks to
start their immunisation schedule has found
that this increases the coverage and timeliness
of the immunisation series.3 However, the most
significant finding of this study is the importance
of enrolment of newborn babies with a general
practice. Making an early connection with a
practice means that an infant is much more likely
to be immunised fully and on time, as well as
the other likely health care gains that may result
from engagement with their general practitioner
(GP) or practice nurse.
Controversy around prostate-specific antigen
(PSA) screening continues. A study of GPs in the
Waikato found a high likelihood of them PSA
testing asymptomatic men including those aged
70 years or older, despite there being no evidence
of benefit in this activity.4 A qualitative study
suggests that, in Wellington at least, GPs may
not be screening and intervening sufficiently
with patients around alcohol misuse.5 While
some GPs may be ignoring Ministry of Health
recommendations regarding prostate and alcohol
screening, it appears that best practice guidance
on management of acute otitis media in children is being followed. A cohort study of nearly
20 000 New Zealand children shows a significant
decline in the use of antibiotics in treatment, in
concordance with accepted best practice.6
There are two studies on primary mental health
initiatives for Maori and other underserved
populations. Mathieson and colleagues report on
a Maori adaptation of a brief intervention involving cognitive behavioural therapy and guided
self-management,7 and a research team in Hawkes
Bay describe an integrated, holistic tikanga
Maori–based programme targeting Maori, Pacific
and quintile 5 populations aimed at reducing
mental health inequalities.8
Callaghan explores factors that might influence
GPs’ decision making and finds that clinical information and the probability of disease are rated
as highly important and desirable by ‘standard
setters’ in general practice academic departments
and The Royal New Zealand College of General
Practitioners.9 Lillis and Murton explore the
provision of online resources to GP registrars in
training and conclude that they are only likely
to access the top four in the list, underlining the
importance of prioritising and possibly limiting
provided resources.10 A study by Kljakovic finds
that patients from both Australian and New
Zealand general practices performed poorly in
correctly locating body organs in line drawings,
and health professionals achieved this only moderately better than their patients.11
On an even more practical bent, two viewpoint
papers offer specific clinical tips. Leung extends
the concept of the World Health Organization
analgesic ladder to that of a platform, providing
a broad range of pain relief interventions in a
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
EDITORIALS
FROM THE EDITOR
stepped-up manner,12 and Lee and Loh review the
facts around bone mineral densitometry.13
Our regular columns provide practical tips on the
use of topical antibiotics in acute conjunctivitis
(Cochrane Corner), best practice evidence for managing a number of musculoskeletal conditions
(String of PEARLS), the potential harm and lack
of evidence of benefit for use of colloidal silver
(Potion or Poison?), strategies to identify cognitive
impairment from statin use (Nuggets of Knowledge) and possible actions to address hearing loss
among Pacific peoples (Vaikoloa).14
Callaghan writes, ‘it is not possible to divorce the
practice of medicine from the society in which it
is practised’.9 The papers in this issue are about
primary health care practice in our New Zealand
communities with our own patient populations.
No longer do we need to rely on international
research conducted in secondary care settings to
inform our practice—the breadth and depth of
New Zealand primary care research means our
discipline has come of age.
intervention to improve immunisation coverage and timeliness. J Prim Health Care. 2012;4(3):189–198.
4. Hodgson F, Obertová Z, Brown C, Lawrenson R. PSA testing in
general practice. J Prim Health Care. 2012;4(3):199–205.
5. Mules T, Taylor J, Price R, Walker L, Singh B, Newsam P, et al.
Addressing patient alcohol use: a view from general practice.
J Prim Health Care. 2012;4(3):217–222.
6. Gribben B, Salkeld L, Hoare S, Jones H. The incidence
of acute otitis media in New Zealand children under five
years of age in the primary care setting. J Prim Health Care.
2012;4(3):205–212.
7. Mathieson F, Mihaere K, Collings S, Dowell A, Stanley J. Maori
cultural adaptation of a brief mental health intervention in
primary care. J Prim Health Care. 2012;4(3):231–238.
8. Abel S, Marshall B, Rikki D, Luscombe T. Evaluation of Tu
Meke PHO’s Wairua Tangata Programme: a primary mental
health initiative for underserved communities. J Prim Health
Care. 2012;4(3):242–248.
9. Callaghan K. Factors influencing diagnostic decision-making.
J Prim Health Care. 2012;4(3):223–230.
10. Lillis S, Murton S. Does the order of presentation and number
of online resources affect the frequency of access by learners?
J Prim Health Care. 2012;4(3):213–216.
11. Kljakovic M. The anatomical placement of body organs by
Australian and New Zealand patients and health professionals
in general practice. J Prim Health Care. 2012;4(3):239–241.
12. Leung L. From ladder to platform: a new concept for pain
management. J Prim Health Care. 2012;4(3):254–258.
13. Lee J, Loh N. Frequently asked questions on measurement of bone mineral densitometry. J Prim Health Care.
2012;4(3):259–261.
14. Dewes O. Hearing loss among Pacific peoples. J Prim Health
Care. 2012;4(3):250–251.
References
1. Robinson T, Elley R, Wells S, Robinson E, Kenealy T, Pylypchuk
R, et al. New Zealand Diabetes Cohort Study cardiovascular
risk score for people with type 2 diabetes: validation In the
PREDICT COHORT. J Prim Health Care. 2012;4(3):181–188.
2. Khunti K. Commentary: risk prediction models for people with
Type 2 diabetes. J Prim Health Care. 2012;4(3):180.
3. Goodyear-Smith F, Grant C, Poole T, Petousis-Harris H, Turner
N, Perera R, et al. Early connections: effectiveness of a pre-call
A tribute to Professor Marjan Kljakovic
Just as this issue is going to press we have received the very sad news that Marjan, the author
of one of the papers in this issue (Kljakovic M. The anatomical placement of body organs
by Australian and New Zealand patients and health professionals in general practice. J Prim
Health Care. 2012;4(3):239–241), died today, having suffered a major myocardial infarction
on 29 July.
A New Zealand academic general practitioner, Marjan relocated across the ditch seven years
ago as Professor at the Academic Unit of General Practice and Community Health, Australian
National University Medical School, Canberra. However, he remained a Kiwi at heart. Marjan
was highly regarded as an inspirational thinker and an innovative teacher who contributed
extensively to philosophical debate in the general practice arena. He will be sadly missed.
Editor, 14 August 2012
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE179
EDITORIALS
GUEST EDITORIAL
Commentary: risk prediction models for
people with Type 2 diabetes
Kamlesh Khunti PhD, MD, FRCGP, FRCP
Department of Health
Sciences, University of
Leicester, United Kingdom
J PRIM HEALTH CARE
2012;4(3):180.
CORRESPONDENCE TO:
Kamlesh Khunti
Professor of Primary Care
Diabetes and Vascular
Medicine, Department
of Health Sciences,
University of Leicester,
Gwendolen Road,
Leicester LE5 4PW, UK
kk22@le.ac.uk
180
P
eople with Type 2 diabetes are at increased
risk of cardiovascular disease, the determinants of which are multifactorial.1 A
number of international guidelines recommend
calculating future cardiovascular disease risk
for management of patients with Type 2 diabetes. There has been a plethora of cardiovascular
disease risk prediction models for Type 2 diabetes
and a recent systematic review identified 45
prediction models, of which 12 were developed
for patients with Type 2 diabetes.2 Less than onethird of these were externally validated in a diabetes population and overall the discriminative
value for most prediction models was moderate.2
Another systematic review confirmed limited
evidence of impact on patient management and
outcomes with the use of prediction models.3
References
1. Sarwar N, Gao P, Seshasai SR, Gobin R, Kaptoge S. Diabetes
mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective
studies. Lancet. 2010;375:2215–22.
2. van Dieren S, Beulens JWJ, Kengne AP, Peelen LM. Prediction
models for the risk of cardiovascular disease in patients with
Type 2 diabetes: a systematic review. Heart. 2012;98:360–9.
3. Willis A, Davies MJ, Yates T, Khunti K. Primary prevention of
cardiovascular disease using validated risk scores: a systematic
review. Journal of the Royal Society of Medicine. 2012.
4. Robinson T, Elley C, Wells S, et al. New Zealand Diabetes
Cohort Study cardiovascular risk score for people with Type 2
diabetes: validation in the PREDICT cohort. J Prim Health
Care. 2012;4(3): 181–189.
In this issue of the journal, Robinson and colleagues have conducted a validation study of
the Diabetes Cohort Study (DCS) CVD Risk
Predictive model in people with Type 2 diabetes
in New Zealand.4 The strengths of this study
are the large numbers of people included, the
long follow-up with 12.8% of people having a
cardiovascular outcome, and the validation being
conducted in a population in which the score was
derived. The study found that the DCS model
had marginally better discrimination than the
currently used New Zealand Framingham risk
equation. Overall the discriminative value was
moderate. Many of the previous new scores have
been compared with the well-established United
Kingdom Prospective Diabetes Study risk score
and, therefore, this is one limitation of this
study. In addition, robust evidence on the impact
of use of risk prediction models on patient outcomes in terms such as adherence to medications,
patient understanding or improvements in harder
outcomes is lacking. Until such evidence is available, the use of risk prediction models in routine
clinical practice will not be adopted.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
New Zealand Diabetes Cohort Study
cardiovascular risk score for people with
Type 2 diabetes: validation in the PREDICT cohort
Tom Robinson MBChB, MPH, FNZCPHM, FRNZCGP;1,3 C Raina Elley MBChB, FRNZCGP, PhD;1 Sue
Wells MBChB, FRNZCGP, FNZCPHM, PhD;2 Elizabeth Robinson MSc;2 Tim Kenealy MBChB, FRNZCGP,
PhD;1 Romana Pylypchuk MPH, MSc;2 Dale Bramley MBChB, MPH, FNZCPHM;3 Bruce Arroll MBChB,
FRNZCGP, PhD;1 Sue Crengle MBChB, FNZCPHM, FRNZCGP, PhD;4 Tania Riddell MBChB, MPH, FNZCPHM;2
Shanthi Ameratunga MBChB, FRACP, FNZCPHM, PhD;2 Patricia Metcalf PhD;5 Paul L Drury MA, MB
BChir, FRCP, FRACP6
Department of General
Practice and Primary Health
Care, The University of
Auckland, Auckland,
New Zealand
1
Section of Epidemiology and
Biostatistics, The University of
Auckland
2
Waitemata District Health
Board, Auckland
3
ABSTRACT
INTRODUCTION: New Zealand (NZ) guidelines recommend treating people for cardiovascular disease
(CVD) risk on the basis of five-year absolute risk using a NZ adaptation of the Framingham risk equation.
A diabetes-specific Diabetes Cohort Study (DCS) CVD predictive risk model has been developed and
validated using NZ Get Checked data.
AIM: To revalidate the DCS model with an independent cohort of people routinely assessed using
PREDICT, a web-based CVD risk assessment and management programme.
METHODS: People with Type 2 diabetes without pre-existing CVD were identified amongst people who
had a PREDICT risk assessment between 2002 and 2005. From this group we identified those with sufficient data to allow estimation of CVD risk with the DCS models. We compared the DCS models with the
NZ Framingham risk equation in terms of discrimination, calibration, and reclassification implications.
Te Kupenga Hauora Maori,
The University of Auckland
4
Department of Statistics,
The University of Auckland
5
Auckland Diabetes Centre,
Auckland District Health
Board
6
RESULTS: Of 3044 people in our study cohort, 1829 people had complete data and therefore had CVD
risks calculated. Of this group, 12.8% (235) had a cardiovascular event during the five-year follow-up. The
DCS models had better discrimination than the currently used equation, with C-statistics being 0.68 for
the two DCS models and 0.65 for the NZ Framingham model.
DISCUSSION: The DCS models were superior to the NZ Framingham equation at discriminating people
with diabetes who will have a cardiovascular event. The adoption of a DCS model would lead to a small
increase in the number of people with diabetes who are treated with medication, but potentially more
CVD events would be avoided.
KEYWORDS: Cardiovascular disease; diabetes; prevention; risk assessment; reliability and validity
Introduction
Globally there is an epidemic of Type 2 diabetes.1,2 It was estimated that in 2010 there were
over 195 000 people in New Zealand (NZ) with
diabetes—5.6% of the adult population.3 People
with diabetes are at increased risk of dying of
cardiovascular disease (CVD) which accounts for
almost 50% of all deaths amongst people with
diabetes.4,5
There is considerable evidence that energetic
management of risk factors such as blood pressure, dyslipidaemia, and glycaemia reduces the
risk of CVD in people with diabetes.6–11 However, it is accepted that rather than treating risk
factors separately, clinicians should use absolute
CVD risk to guide patient management.12,13
NZ guidelines for cardiovascular risk assessment use a predictive risk equation adapted from
J PRIM HEALTH CARE
2012;4(3):181–188.
CORRESPONDENCE TO:
Tom Robinson
Department of General
Practice and Primary
Health Care, The University
of Auckland, PB 92019
Auckland, New Zealand
t.robinson@auckland.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE181
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
the United States Framingham Heart Study.14,15
This equation has a number of disadvantages for
predicting risk of CVD amongst people with
diabetes in NZ. In particular, the Framingham
cohort was from the United States, did not
include ethnic groups that are important in NZ,
and only included a small number of people with
diabetes.16 In addition, the equation does not
include a number of diabetes-specific variables—
such as duration of diabetes, glycaemic control,
and albuminuria—that are predictive of cardiovascular outcomes.17–20 The NZ adaptation of the
Framingham model does include adding a single
additional five-year risk of 5% for these factors.14
In 2010, Elley et al. reported two predictive CVD
equations based on the New Zealand Diabetes
Cohort Study (DCS). This was a prospective open
cohort that used data from a national primary
care diabetes programme (Diabetes Get Checked),
which commenced in 2000.21 Full details of the
derivation and validation of the equation are
described in the original article.21 Briefly, data
from 36 127 people with Type 2 diabetes, but
without pre-existing CVD, were matched to
national hospitalisation and mortality databases.
Predictor variables for the first equation (DCS-A)
included age at diagnosis, duration of diabetes,
sex, ethnicity, smoking status, systolic blood
pressure, HbA1c, total cholesterol: HDL cholesterol ratio (TC/HDL), and the presence of microor macroalbuminuria. A second equation (DCS-B)
also included current antihypertensive treatment.
The performance of both equations was tested on
10 030 individuals from a different geographic
area in NZ with discrimination and calibration
superior to the original Framingham equation.21
Before using a prognostic model in clinical practice it is important to validate it using data from
other independent populations of patients.22 This
study aimed to validate the DCS models using
data from a cohort of people routinely assessed in
NZ general practice with PREDICT, a CVD risk
assessment and management programme.
Methods
Design
This validation study uses data from primary
care to assess the discrimination, calibration and
182
reclassification implications of the DCS equations
in predicting CVD events, compared with actual
events over five years.
Study population
PREDICT is a web-based, real-time decision support programme that has been integrated with
most practice management software in use in NZ
primary care.23 General practitioners and practice
nurses enter required clinical data to create a risk
profile. This profile is sent by a secure internet connection to a central server that returns the patient’s
NZ Framingham five-year cardiovascular risk score
with management recommendations. At the same
time, an electronic profile is stored and linked to an
encrypted National Health Index (NHI) number.
These were anonymously linked to national hospitalisation, pharmaceutical dispensing and mortality outcomes and also to regional laboratory data.
Individuals identified as having Type 2 diabetes
and no known pre-existing CVD with a PREDICT assessment between 27 August 2002 and
31 December 2005 were included. Individuals
were said to have diabetes if they were identified by their primary care physician as having
diabetes at first risk assessment, or if they had
been identified as having diabetes in the national
hospitalisation database, or had been prescribed
insulin or an oral hypoglycaemic agent prior to or
on their first PREDICT assessment date. If the
type of diabetes was unclear, we assigned them
as Type 2 if they were never on insulin, if they
had been on an oral hypoglycaemic agent, or if
their age of onset was over 30 years in Maori and
Pacific or over 50 in other ethnic groups. Preexisting CVD was identified from the primary
care physician’s risk assessment record.
Risk variables
Risk factor variables required for the DCS equations were extracted for each individual. Data
on some of the variables were missing from
early PREDICT risk assessments. Duration of
diabetes was included if it could be calculated
from any subsequent PREDICT risk assessment
record. Missing laboratory data were obtained
from laboratory records where results from up to
five years prior to the baseline assessment or two
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
weeks after the assessment were available. After
the addition of these data, only individuals with
a complete minimum dataset were included in the
final study cohort. Ethnicity was derived from
both the primary care practitioner records and
the encrypted NHI database and was prioritised
in the order: Maori, Pacific, South Asian, East
Asian, ‘Other’ and European.
Outcome measures
Primary care data were linked to national hospitalisation and mortality databases by NHI number to
identify all CVD events over the five years following baseline for each individual. CVD events included hospital admission or death from ischaemic
heart disease, cerebrovascular disease or peripheral vascular disease. These were identified from
national hospital and mortality databases coded according to ICD-9 and ICD-10 (see the appendix in
the web version of this paper).21 Five-year risk was
calculated for each individual according to both the
NZ Framingham and the DCS equations.21
Analyses
We compared predicted risk with observed
outcomes. To assess discrimination, the ability of
the models to distinguish between individuals
who do or do not have a subsequent CVD event,
we calculated the area under the receiver operating
characteristic (ROC) curve (C statistic).13,22,24 Calibration was assessed by comparing the observed
and predicted probabilities of CVD events in
the pre-specified deciles of DCS model risk, and
performing a Hosmer–Lemeshow test for equivalence. The effect of reclassification of risk from the
NZ Framingham model to the DCS models was
measured using a 15% five-year cardiovascular risk
threshold. NZ guidelines recommend drug treatment with five-year risks above 15%. A scatter plot
of risks predicted by the two models with these
pre-determined risk categories was also produced.24
All analyses were undertaken using Stata® 11.2.
Ethical approval
This validation study was approved by the Multiregion Ethics Committee (WGT/04/09/077) as
part of the Diabetes Cohort Study. The PREDICT cohort study and research process was ap-
WHAT GAP THIS FILLS
What we already know: People with Type 2 diabetes are at high risk of
a cardiovascular event. A locally derived Diabetes Cohort Study CVD risk
equation—http://www.nzssd.org.nz/cvd/—has been found to be more valid
for those with diabetes in New Zealand than the currently used Framingham
equation.
What this study adds: Before incorporating the new equation into
national recommendations for management, further validation was required
using an independent cohort. The Diabetes Cohort Study CVD risk equation
predicted risk more accurately than the currently used adjusted Framingham
equation among people with diabetes in the New Zealand PREDICT cohort.
proved by the Northern Region Ethics Committee Y in 2003 (AKY /03/12/314) with subsequent
annual approval by the National Multi-region
Ethics Committee since 2007 (MEC/07/19/EXP).
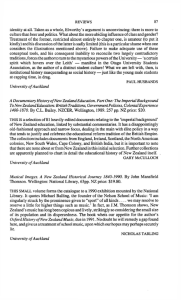
Results
Study population
The derivation of the study cohort and subsequent CVD events is shown in Figure 1. We
classified 3044 (13.3%) people on the database as
people with Type 2 diabetes without pre-existing
CVD. Of these, 1829 (60.1%) had the minimum
dataset of risk variables required and formed the
final cohort for the study. About two-thirds of
these individuals (65.9%) were included after having data added from sources other than the first
risk assessment record. These data were diabetesspecific variables (HbA1c, urinary albumin/creatinine ratio, diabetes duration, and age of onset
of diabetes). All individuals were followed for
five years from their initial CVD risk assessment.
During that time, 235 had first CVD events
(12.8%), in which 45 (2.5%) were fatal and 190
(10.4%) were non-fatal events.
Baseline characteristics of participants are
presented and compared with those of the 1215
people excluded due to missing variables in
Table 1. Compared with those included, a higher
proportion of the excluded group were European and a lower proportion Pacific. Excluded
participants had slightly higher systolic blood
pressures and TC/HDL ratios and were less likely
to be recorded as being past smokers. Although
the two groups had similar risks of CVD events
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE183
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Discrimination
Figure 1. Flow diagram of participants through study
24 446 people with first PREDICT risk assessment
between 27 August 2002 and 31 December 2005
851 people with
Type 2 diabetes and
pre-existing CVD
20 551 people with
Type 2 diabetes
3044 people with identified Type 2 diabetes
1215 people without
minimum dataset
1829 (60.1%) people with minimum* datasets
34.1% complete data from first PREDICT assessment
65.9% duration of diabetes derived from
subsequent assessments
Calibration
65.4% HbA1c from urinary ACRs variables derived from
other laboratory data
0.5% derived from subsequent PREDICT
assessments within 1 year
26 died from non-CVD
causes
235 (12.8%) people had first CVD event within
five years of date of their first PREDICT risk assessment
(45 fatal and 190 non-fatal)
Figure 3 compares the mean predicted risk with
the mean observed five-year event rate for each
decile of predicted risk for DCS-B and NZ
Framingham equations. The DCS equations
predicted higher risks than the NZ Framingham equation for people in the higher deciles of
risk. The Hosmer–Lemeshow test showed that
estimated risks based on the baseline risk profile
tended to be higher than the real event rate for
all equations (p<0.001 for DCS-A, p=0.001 for
DCS-B, and p=0.02 for NZ Framingham).
Reclassification
* Minimum dataset = age at diagnosis, gender, duration of diabetes, smoking status,
systolic blood pressure, HbA1c, fasting serum total cholesterol and HDL, urine
albumin-creatinine ratio, ethnicity, anti­hypertensive medication
according to the NZ Framingham equation and
observed events during follow-up, the excluded
group had higher fatal CVD and other-cause
mortality. Differences in duration, HbA1c, and
albuminuria between the ‘Included’ and ‘Excluded’ groups may not reflect a true underlying
difference, as information on these variables was
missing for many in the ‘Excluded’ group.
184
The ROC curves for the DCS-B equation (with
antihypertensive status included) and the modified NZ Framingham equation are shown in Figure 2. The area under the ROC curve (C statistic)
was 0.678 (95% CI 0.642–0.714) for the DCS-A
equation (without antihypertensive status included) and 0.684 (95% CI 0.648–0.720) for the DCSB equation. The C statistic for the NZ Framingham equation in this study was 0.648 (95% CI
0.612–0.684) and the unadjusted Framingham
equation was 0.649 (95% CI 0.613–0.685). Both
DCS equations had significantly higher C statistics than the NZ Framingham equation (p=0.04
DCS-A equation and p=0.01 DCS-B equation).
The DCS-B equation C statistic was also significantly higher than the DCS-A equation (p=0.04).
The C statistics for the DCS equations in this
study were similar to those found in the original
DCS validation study (0.69).21
The effect of reclassification of risk from the
NZ Framingham model to the DCS models was
measured using a 15% five-year cardiovascular
risk threshold. Figure 4 plots the predicted
five-year risk of a CVD event for each individual using the DCS-B and NZ Framingham equations. Horizontal and vertical lines
represent the 15% five-year risk cut-offs above
which drug therapy is usually recommended
in NZ. Area B in the graph represents individuals that are classified as being at low risk
under the DCS equation, but high risk under
the NZ Framingham equation. Area D on the
graph represents people who were classified as
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 1. Characteristics at baseline for study cohort compared with those excluded due to missing variables
Characteristic
Included
Excluded
Mean (SD) or Median (IQR)*
or n (%)
N
Data available,
n (%)
P value
Mean (SD) or Median (IQR)*
or n (%)
1829
1215
Age (years)
57.3 (10.7)
1215 (100)
57.0 (12.5)
Age at diagnosis (years)
51.7 (11.1)
360 (30)
53.4 (11.3)
0.01
4 (2-8)
360 (30)
1 (0-4)
<0.001
Diabetes duration (years)*
Gender
0.6
1215 (100)
Men
926 (50.6%)
668 (55.0%)
Ethnicity
1215 (100)
European
550 (30.1%)
575 (47.3%)
Maori
245 (13.4%)
155 (12.8%)
Pacific
756 (41.8%)
296 (24.4%)
South Asian
162 (8.9%)
93 (7.7%)
East Asian
82 (4.5%)
80 (6.6%)
Other
25 (1.4%)
Systolic blood pressure
Total cholesterol:HDL ratio
HbA1c (%)*
0.02
<0.001
16 (1.3%)
134.8 (15.6)
1215 (100)
137.8 (19.0)
<0.001
4.1 (1.2)
1214 (100)
4.3 (1.3)
<0.001
7.4 (6.5-8.6)
803 (66)
6.8 (6.2-7.9)
<0.001
Smoking status
1215 (100)
Current smoker
342 (18.7%)
Previous smoker
386 (21.1%)
<0.001
211 (17.4%)
95 (7.8%)
Albuminuria
458 (38)
Microalbuminuria
301 (16.5%)
Macroalbuminuria
88 (4.8%)
<0.001
100 (21.8%)
36 (7.9%)
Taking medications
1215 (100)
Antihypertensives
213 (11.7%)
186 (15.3%)
0.003
Lipid-lowering meds
185 (10.1%)
143 (11.8%)
0.1
15.0 (10.1-20.7)
0.6
5-year CVD risk *
†
14.8 (10.6-19.3)
Outcomes
1213 (100)
1215 (100)
Any CVD event
235 (12.8%)
154 (12.7%)
0.9
Fatal CVD event
45 (2.5%)
70 (5.8%)
<0.001
Non-CVD deaths
26 (1.4%)
45 (3.7%)
<0.001
* Median and inter-quartile range (IQR) given as distribution is skewed.
† NZ-adjusted Framingham equation
high risk under the DCS equation, but low risk
under the NZ Framingham equation. Areas A
and C represent people who are given the same
classification by both models. There are more
people who subsequently have CVD events in
area D than in area B, indicating that, although
there were both successes and failures in reclassification, sensitivity for the DCS equation was
superior. However, there are also more people
who did not have events who were reclassified
to high risk.
Moving from the NZ Framingham equation to
the DCS-B equation improves sensitivity from
63.8% to 77.0% (Table 2), but decreases specificity
from 54.0% to 51.4%. DCS-A behaves similarly.
The positive predictive values (PPVs) and the
negative predictive values (NPVs) are higher for
the two DCS equations than the NZ Framingham equation. These results are based upon our
study cohort five-year prevalence of CVD events
of 12.8% (95% CI, 11.3–14.4%). Sensitivity analysis around the 95% confidence intervals of CVD
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE185
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Figure 2. Receiver operating curves for the DCS-B equation and the NZ Framingham CVD
equation (five-year risk)
1.00
Strengths and limitations
Sensitivity
0.75
The use of diabetes duration, HbA1c levels, and
degrees of albuminuria are likely to contribute to
better discrimination, particularly for higher risk
groups. In addition, the DCS equation was developed in a cohort of much greater relevance to the
NZ diabetes population than the Framingham
equation, even though adjustments were made by
the NZ guidelines.14
0.50
0.25
0.00
0.00
0.25
0.50
0.75
1.00
1-Specificity
DCS with antihypertensives
NZ Framingham
Figure 3. Five-year risks observed in the study cohort compared with those predicted by
the DCS-B equation and the NZ Framingham equation for different deciles of risk
event prevalence does not change the relative
performance of the models (results not shown).
Discussion
Main finding
For this cohort of people with Type 2 diabetes,
the DCS equations were better at discriminating
risk of a first CVD event than the NZ Framingham equation currently being used in primary
186
care in NZ. The latter model in this cohort had
an area under the ROC curve of 0.65 while the
DCS equation gave an area of 0.68.
There are a number of important methodological
limitations in this validation study. One is that
these equations were developed and validated on
a cohort of people who may have being treated
for their CVD risk. Indeed, the PREDICT programme, from which this cohort is gathered, is
specifically intended to lower risk of CVD events
by encouraging appropriate treatment. Historically, these equations have been used to predict the
outcomes for patients if they were not treated. It
is therefore likely that the risk of CVD events in
this scenario would be higher than the observed
risk in this cohort.
All three equations overestimated risk when
compared to actual events in the cohort. This was
in contrast to the initial validation study, where
the DCS equations underestimated risk of first
CVD event.21 The first possibility is the effectiveness of the PREDICT programme in reducing
risk, as discussed above. A second possibility is
that the PREDICT cohort is at lower risk than
the original DCS cohort, possibly because people
with higher risk and comorbidities were enrolled
earlier into the Get Checked programme. It is
also possible that the difference is due to random
error due to the relatively small number of observed events in this study. The overall five-year
CVD incidence estimation is somewhat imprecise
(12.8%, 95% CI 11.3–14.4%).
A further limitation is that an equation should
ideally be validated on a population that is
representative of the population on which it will
eventually be used. It is a strength of this study
that the PREDICT cohort is much more repre-
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
sentative of NZ people with diabetes than the
original Framingham equation cohort. Nevertheless, the baseline characteristics table suggested
that this cohort was not completely representative
of NZ people with diabetes. For example, Pacific
people were over-represented compared to the
overall diabetes population. It is also possible that
our inability to obtain data on all patients in the
original cohort has introduced a selection bias
to our final validation cohort. As discussed, included subjects may have been at a slightly lower
risk than those excluded. However, it is important that equations discriminate across diverse as
well as representative populations.
In validating any equation, it is important to
have accurate data on the cohort being studied.
The PREDICT data are collected by primary care
physicians in routine care rather than by researchers and therefore may contain some inaccuracies.
As previously mentioned, some data were not
available from the baseline risk assessment and
had to be obtained from either laboratory data or
subsequent risk assessment records. It is possible
that other data, such as smoking status or diabetes
duration, may be inaccurately recorded. Such deficiencies would lead to poorer discrimination of the
equations. The degree to which they might also
lead to systematic under- or overestimation of the
predicted risks is more difficult to judge. However,
these limitations also reflect the ‘real-life’ clinical
situation in which these tools are used.
Implications for clinical practice
Whilst the current NZ guidelines for managing
cardiovascular risk provide guidance for management across a broad range of risks, an important
decision point is when to begin treatment of
risk with medications.14 At a population level,
changing from the current NZ Framingham
equation to one of the DCS equations would have
a substantial impact on the way diabetes is managed in NZ. If this cohort were representative of
people with diabetes in NZ, then changing to the
DCS-B equation would result in recommending
treating 53% of people with diabetes with lipidlowering and antihypertensive medication instead
of 49%. Using the Ministry of Health estimates
of the number of people with Type 2 diabetes in
NZ, and excluding the estimated 22% of people
with diabetes who have pre-existing CVD, then
6503 extra people should be offered treatment.
However, the benefit would be that an additional
2587 people, who would have had a first CVD
event over the next five years, would be correctly
identified and offered preventive therapy. As
researchers interested in the population manage-
Figure 4. Scatter plot of five-year risk of CVD events predicted by the DCS-B equation
against the NZ Framingham equation with 15% five-year risk cut-offs shown
Chart area
A
B
C
D
NZ Framingham classification
Low
High
High
Low
DCS classification with antihypertensives
Low
Low
High
High
Total
Outcome
No event
634
185
549
226
1594
40%
12%
34%
14%
100%
43
11
139
42
235
18%
5%
59%
18%
100%
Proportion
CVD event
Proportion
All patients
Proportion
677
196
688
268
1829
37%
11%
38%
15%
100%
Table 2. Sensitivity, specificity, positive predictive value, and negative predictive value for
predicted vs actual CVD events using the DCS and Framingham equations with a 15% risk
cut-off (12.9% event prevalence)
DCS-A
DCS-B
NZ Framingham
Sensitivity
79.6%
77.0%
63.8%
Specificity
45.3%
51.4%
54.0%
Positive predictive value
17.7%
18.9%
17.0%
Negative predictive value
93.8%
93.8%
91.0%
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE187
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
ment of diabetes, we believe this would be a very
worthwhile trade-off.
At an individual level, the person with diabetes
or their clinician needs to know, firstly, that on
average over a five-year period, 13 people out of
100 will have a CVD event. Secondly, of these
13 people, the DCS equation will correctly
identify 10 of these people so they can be offered
treatment, whereas the current NZ Framingham
equation will successfully predict eight. However, to achieve this, 53 of the 100 people will need
to take medication (or five more than currently
would be the case). Since it is impractical to offer individual patients the choice of model, we
believe it is important to consult both clinicians
and patient representatives as to which model is
preferable. Should the DCS equation be approved,
then it can be seamlessly added to the PREDICT
decision support engine and available at the point
of care.
ACKNOWLEDGEMENTS
We would like to
acknowledge the patients,
practices and primary
care organisations who
contributed data both
to the Diabetes Cohort
Study and the PREDICT
study, and Diagnostic
MedLab Ltd who provided
anonymous matched
laboratory data.
FUNDING
We would like to
acknowledge the NZ
Health Research Council
and Auckland Medical
Research Foundation for
supporting the collection
of data for the original
cohort studies and for
supporting this validation
study. One author (T
Riddell) is the recipient
of a National Heart
Foundation fellowship.
COMPETING INTERESTS
None declared.
188
In conclusion, we have validated the previously
developed DCS equations using a different cohort
of people with diabetes from the PREDICT
dataset and compared its performance with the
currently used NZ Framingham equation. We
have shown that it has advantages over the current equation at a technical and population health
level. From a patient perspective, it will lead to
an increased chance of treatment, but also the opportunity to prevent more first CVD events.
References
1. Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek
CJ, et al. National, regional, and global trends in fasting plasma
glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies
with 370 country-years and 2.7 million participants. Lancet.
2011;378(9785):31–40.
2. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence
of diabetes: estimates for the year 2000 and projections for
2030. Diabetes Care. 2004;27(5):1047–53.
3. Wright C. Estimated prevalence of Type 2 Diabetes in New
Zealand. In: Robinson T, editor. Wellington: Ministry of
Health; 2011.
4. Seshasai SR, Kaptoge S, Thompson A, Di Angelantonio E, Gao
P, Sarwar N, et al. Diabetes mellitus, fasting glucose, and risk
of cause-specific death. N Engl J Med. 2011;364(9):829–41.
5. Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M.
Mortality from coronary heart disease in subjects with Type 2
diabetes and in nondiabetic subjects with and without prior
myocardial infarction. N Engl J Med. 1998;339(4):229–34.
6. SIGN. Management of diabetes: a national clinical guideline:
Scottish Intercollegiate Guidelines Network. Edinburgh: Scottish Intercollegiate Guidelines Network; 2010.
7. Marso SP, Kennedy KF, House JA, McGuire DK. The effect of
intensive glucose control on all-cause and cardiovascular mortality, myocardial infarction and stroke in persons with Type 2
diabetes mellitus: a systematic review and meta-analysis. Diab
Vasc Dis Res. 2010;7(2):119–30.
8. Selvin E, Bolen S, Yeh HC, Wiley C, Wilson LM, Marinopoulos SS, et al. Cardiovascular outcomes in trials of oral
diabetes medications: a systematic review. Arch Intern Med.
2008;168(19):2070–80.
9. Brugts JJ, Yetgin T, Hoeks SE, Gotto AM, Shepherd J, Westendorp RG, et al. The benefits of statins in people without
established cardiovascular disease but with cardiovascular risk
factors: meta-analysis of randomised controlled trials. BMJ.
2009;338:b2376.
10. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10year follow-up of intensive glucose control in Type 2 diabetes.
New Eng J Med. 2008;359(15):1577–89.
11. Holman RR, Paul SK, Bethel MA, Neil HA, Matthews DR.
Long-term follow-up after tight control of blood pressure in
type 2 diabetes. New Eng J Med. 2008;359(15):1565–76.
12. Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A.
Treatment with drugs to lower blood pressure and blood
cholesterol based on an individual’s absolute cardiovascular
risk. Lancet. 2005;365(9457):434–41.
13. D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M,
Massaro JM, et al. General cardiovascular risk profile for use
in primary care: the Framingham Heart Study. Circulation.
2008;117(6):743–53.
14. New Zealand Guidelines Group. Evidence-based best-practice
guideline. The assessment and managment of cardiovascular
risk. Wellington: New Zealand Guidelines Group; 2003.
15. New Zealand Guidelines Group. New Zealand cardiovascular
guidelines handbook: a summary resource for primary care
practitioners. 2009 edition. Wellington: New Zealand Guidelines Group; 2009.
16. Anderson K, Odell P, Wilson P, Kannel W. Cardiovascular
disease risk profiles. Am Heart J. 1991;121:293–8.
17. Elley CR, Kenealy T, Robinson E, Drury PL. Glycated haemoglobin and cardiovascular outcomes in people with Type 2
diabetes: a large prospective cohort study. Diabet Med.
2008;25(11):1295–301.
18. Selvin E, Marinopoulos S, Berkenblit G, Rami T, Brancati FL,
Powe NR, et al. Meta-analysis: glycosylated hemoglobin and
cardiovascular disease in diabetes mellitus. Ann Intern Med.
2004;141(6):421–31.
19. Fox CS, Sullivan L, D’Agostino RB Sr, Wilson PW. The significant effect of diabetes duration on coronary heart disease
mortality: the Framingham Heart Study. Diabetes Care.
2004;27(3):704–8.
20.Newman DJ, Mattock MB, Dawnay AB, Kerry S, McGuire A,
Yaqoob M, et al. Systematic review on urine albumin testing
for early detection of diabetic complications. Health Technol
Assess. 2005;9(30):iii–vi, xiii–163.
21. Elley C, Robinson E, Kenealy T, Bramley D, Drury P. Derivation
and validation of a new cardiovascular risk score for people
with Type 2 diabetes: The New Zealand Diabetes Cohort
Study. Diabetes Care. 2010;33(6):1347–52.
22.Altman DG, Vergouwe Y, Royston P, Moons KG. Prognosis
and prognostic research: validating a prognostic model. BMJ.
2009;338:b605.
23.Bannink L, Wells S, Broad J, Riddell T, Jackson R. Web-based
assessment of cardiovascular disease risk in routine primary
care practice in New Zealand: the first 18 000 patients (PREDICT CVD-1). N Z Med J. 2006;119(1245):U2313.
24. McGeechan K, Macaskill P, Irwig L, Liew G, Wong TY.
Assessing new biomarkers and predictive models for use
in clinical practice: a clinician’s guide. Arch Intern Med.
2008;168(21):2304–10.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Early connections: effectiveness of a pre-call
intervention to improve immunisation coverage
and timeliness
Felicity Goodyear-Smith MBChB, MD, FRNZCGP;1 Cameron Grant MBChB, FRACP, PhD;2 Tracey Poole;1
Helen Petousis-Harris BSc, PhD;1 Nikki Turner MBChB, MPH, FRNZCGP;1 Rafael Perera Sc, DPhil;3
Anthony Harnden MBChB, MSc, FRCGP, FRCPCH3
Department of General
Practice and Primary Health
Care, Faculty of Medical
and Health Science, The
University of Auckland,
Auckland, New Zealand
1
ABSTRACT
INTRODUCTION: Children who have missed or delayed immunisations are at greater risk of vaccinepreventable diseases and getting their first scheduled dose on time strongly predicts subsequent
complete immunisation. Developing a relationship with an infant’s parents and general practice staff soon
after birth followed by a systematic approach can reduce the number of delayed first immunisations.
AIM: To assess the effectiveness of a general practice–based pre-call intervention to improve immunisation timeliness.
METHODS: Clustered controlled trial of general practices in a large urban district randomised to either
delivery of pre-call intervention to all babies at aged four weeks or usual care.
Department of Paediatrics,
Faculty of Medical and Health
Science, The University of
Auckland
2
Department of Primary
Health Care, University of
Oxford, Oxford, England
3
RESULTS: Immunisation timeliness for infants receiving the primary series of immunisations among their
nominated Auckland general practices was higher than expected at 98% for the six week event. The
intervention was statistically but not clinically significant. Coverage was significantly lower among infants
with no nominated practice which reduced overall coverage rate for the district.
DISCUSSION: Pre-call letters with telephone follow-up are simple interventions to introduce into the
practice management system and can be easily implemented as usual standard of care. Early identification
of newborn infants, primary care engagement and effective systems including tracking of infants not enrolled in general practices has the greatest potential to improve immunisation coverage rates even further.
KEYWORDS: Randomized controlled trial; immunization; vaccination; general practice; intervention
studies
Introduction
New Zealand (NZ) historically has mediocre
immunisation coverage of children1 and relatively
high rates of vaccine-preventable disease.2 The
risk of vaccine-preventable diseases is greater if
childhood immunisations are incomplete, which
includes both missed and delayed immunisations.
Delays in immunisation puts infants at significant risk of contracting and being hospitalised for
diseases such as Haemophilus influenzae type b3–6
and pertussis4,6–9 and increases the potential reservoir of disease in unvaccinated infants.5,10
Receiving the first dose on the vaccination
schedule on time is one of the strongest and most
consistent predictors of subsequent complete immunisation11–13 and delays are significantly more
likely to result in lower overall coverage.12,14–16
In our previous study of 124 practices in the
Auckland and Midland regions of NZ, median
coverage at six weeks for the diphtheria, tetanus
and acellular pertussis immunisation was 93%,
while timely receipt of this dose was only 40%.17
Factors that impact upon immunisation receipt
and timeliness are now well established. These
J PRIM HEALTH CARE
2012;4(3):189–198.
CORRESPONDENCE TO:
Felicity Goodyear-Smith
Professor, Department
of General Practice and
Primary Health Care,
Faculty of Medical and
Health Science, The
University of Auckland,
PB 92019 Auckland,
New Zealand
f.goodyear-smith@
auckland.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE189
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
include the knowledge and attitudes of caregivers, particularly antenatally,18–22 attitudes of
health professionals23,24 and aspects of health care
systems such as cost, recall and reminders and
cost to provider.25
The early establishment of a relationship between
general practices and the infant’s parents can reduce the number of infants whose first immunisation is delayed.12 Our prior study demonstrated
that early enrolment with a primary care provider
was associated with a higher level of immunisation completeness.17,26,27
The NZ immunisation schedule from June 2008
for the first six months of life consisted of two
combination vaccines: INFANRIX® hexa and
Prevenar ® given at ages six weeks, three months
and five months. INFANRIX® hexa contains
antigens from diphtheria, tetanus, and pertussis (DTaP), polio, Haemophilus influenzae type b
and hepatitis B. Prevenar ® (PCV7) is a conjugate
pneumococcal vaccine that contains antigens from
seven pneumococcal serotypes that are predominant causes of invasive pneumococcal disease.28
In addition, Bacillus Calmette-Guérin (BCG) is
given to infants living in households with people
who have, or have had, tuberculosis (TB) or are
in immigrant families from countries where TB
is common, and HBvaxPRO® (hepatitis B vaccine)
is given with hepatitis B–specific immunoglobulin to newborns of mothers who are hepatitis B
carriers.
NZ practices typically have recall systems set up
in their electronic practice management systems
(PMSs) to remind parents that their child’s immunisations are overdue. All childhood scheduled immunisations should be recorded on the
National Immunisation Register (NIR) at the time
of delivery, with data directly transmitted from
the practices. The NIR sends reminder messages
to practices if information about immunisation
events is delayed. The overdue times for NIR are
set outside those for the PMS so that the practices
have time to follow up before they start receiving
overdue messages from the NIR. The PMS will
generate a recall for a child at eight weeks if the
six week doses have not been given, whereas the
NIR will consider that immunisation event overdue when the child is aged 10 weeks. Similarly,
190
PMS and NIR timeliness ‘windows’ for the three
month vaccines are aged four and four and a half
months respectively, and again for the five month
event aged six and six and a half months.
From our previous work, we hypothesised that
the enrolment of children with a general practice
soon after birth, and parents being actively invited when their baby is four weeks old to attend the
practice for their first (six week) set of vaccines,
followed up with early phone calls if they do not
respond, would improve immunisation timeliness.
We therefore aimed to conduct a randomised controlled trial (RCT) of a general practice–based precall intervention. Our objectives were to assess
the effectiveness of this enhanced practice system
on coverage and timeliness of the six week, three
month and five month immunisations.
Methods
Study design
This was an RCT of a multicomponent intervention compared with usual care. Randomisation
was at the level of the general practice. The study
was registered with Australia New Zealand
Clinical Trials Registry (00082892) and ethical approval was obtained from the Ministry of
Health Auckland Regional X Ethics Committee
(Reference NTX/08/08/072).
Setting and study population
The setting was practices in the Auckland District
Health Board (ADHB) catchment area and the
study population was babies born in the ADHB
region and/or those whose parents nominated
practices in the ADHB region as their general
practice. The study took place between 1 November 2008 and 20 April 2010. The NIR is notified
of the nominated general practice for all newborns
and the practice then is informed by the NIR that
they are the baby’s nominated practice. Children
are tracked using the unique National Health
Index (NHI) number assigned at birth.
Intervention
Our intervention consisted of a brief letter of
welcome and invitation to attend when the baby
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
was six weeks, plus simple information on immunisation. This was sent by the practice to the
baby’s caregiver when the baby was four weeks
old (see appendix in the web version of this paper
for this pre-call material). A follow-up phone call
was made to the baby’s caregiver when the baby
was five weeks old if an appointment had not
already been made for the six week vaccinations
and, if the caregiver did not present the baby
for immunisation, a further attempt at contact
(early recall) was made to the caregiver when the
baby was seven weeks old. Phone calls were the
preferred method of pre-call/recall although a
text message, email or letter could also be used.
Practices were given a $15 shopping mall voucher
per baby to acknowledge the time and effort
required to administer the intervention, to be
claimed irrespective of whether or not it resulted
in immunisation of the baby.
Inclusion/exclusion criteria
and practice allocation
A database of all 148 general practices operating
in the ADHB region was created by combining
general practice databases held by the Immunisation Advisory Centre and the Department
of General Practice and Primary Health Care.
Telephone directories were cross-referenced to
ensure all practices in the ADHB region were
included. All practices were assigned a number
(practice code). Practices identified as not involved
in delivering infant immunisations were excluded. Following consent, block randomisations were
conducted of recruited practices using a computer
random number generator to assign each practice
to either the intervention or control group. The
research team other than the project manager were
blind to the identity of practices in the intervention and control groups. Intervention practices
were assisted to adjust their PMS to automatically send out pre-call and recall letters to their
patients in the study.
Outcome measures
Our primary outcome measure was receipt of
six week immunisations and age at which these
were delivered as recorded on the NIR for all the
babies in our study in intervention, control and
non-participating practices. Secondary measure-
WHAT GAP THIS FILLS
What we already know: Children who have delayed or missed immunisation events are at greater risk of vaccine-preventable diseases. Getting
their first scheduled dose on time strongly predicts subsequent complete
immunisation, and developing a relationship between the general practice
staff and a baby’s parents soon after birth can reduce the number of delayed
first immunisations.
What this study adds: Immunisation coverage and timeliness for infants
receiving the primary series of immunisations among their nominated Auckland general practices is extremely high, with no clinically relevant room for
improvement. A pre-call intervention made a statistically significant improvement in timeliness of immunisation, but only by one day. Coverage was significantly lower among infants with no nominated practice and this reduced the
overall coverage rate for a district. Targeting both the systems and services that
can identify and track infants who are not engaged with primary care at birth
has the greatest potential to improve immunisation coverage rates even further.
ments were receipt of three month and five
month immunisations and age at which these
were delivered. Pre- and post-trial surveys were
also conducted for participating practices to establish their practice population and their pre-call/
recall practices before, during and after the trial.
Power calculations
This was a clustered randomised trial with each
enrolled practice being a cluster. Because receipt
of all three primary series doses is important to
most effectively reduce risk of vaccine-preventable diseases, the trial was powered on receipt
of three month and five month immunisations.
Our previous study had shown that the inflation
effect could be between 20 and 40 (see Table 1).17
A significant contributor to this large inflation effect was the fact that at that time some
practices were not enrolling pre-school children
in their practices for pragmatic reasons which led
to a large inter-practice variability in immunisation timeliness and coverage rates. At the time of
this current study, this problem had largely been
addressed with the introduction of the NIR plus
the introduction of children being fully vaccinated by their second birthday as a performance
indicator as part of the Primary Health Organisation Performance Management Programme. With
most or all children being enrolled with practices
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE191
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 1. Summary of sample size calculations
Immunisation
doses
Timely immunisation coverage
Current %
Desired %
Sample size required
DE = 20
Sample size required
DE = 10
6 weeks
88
98
4000
2000
3 months
75
94
2000
1000
5 months
60
85
2000
1000
DE = Design effect
soon after birth, the design effect was expected
to be significantly smaller. We planned to
deliver 1000 interventions. This sample size was
calculated to be sufficient to have 80% power at
the 0.05 level of statistical significance to detect
an increase in the timely immunisation coverage
from 75% to 94% at the three month and from
60% to 85% at the five month immunisations.
Analysis
The variables in the NIR dataset consisted of
NHI number (converted to a unique identifier),
date of birth, dates when six week, three month
and five month immunisations given (vaccines
coded v1 for INFANRIX® hexa and v2 for Prevenar ®), nominated practice at birth, practice(s)
giving immunisation for all children born in
Figure 1. Recruitment of practices in ADHB
All general practices in ADHB
148
Eligible practices
128
Recruited
practices
63
Intervention
practices
(A) 31
192
Non-eligible practices
20
Non-recruited
practices
(C) 65
Control
practices
(B) 32
the ADHB catchment area for the study period
(1 November 2008 to 20 April 2010). At this
date all intervention babies were aged six months
or older. Immunisation events identified as BCG
vaccine were deleted.
Survival curve analysis was used to measure
delay in immunisation. For each infant participant the days from their ideal immunisation date
(i.e. 42 days for six week vaccine) to the actual
day they received vaccine were counted. For this
analysis, second and third dose assumptions
were made, i.e. if the three- and/or five month
vaccines had been given it was assumed that the
child had previously received the earlier doses.
We compared total scores (i.e. number of delayed
days) using survival analysis (Kaplan-Meier and
Cox proportional hazards) for (1) intervention
versus control group (intention to treat analysis),
(2) pre-call versus non-pre-call in the intervention group, and (3) pre-call in the intervention
group versus control group to test if there was
any significant differences. This allowed analysis
by continuous rather than dichotomous data
(i.e. defining an immunisation event as either on
time or delayed). This provided greater statistical
power and allowed for graphic representation of
results plotting number of delayed days over time
for both groups. Adjustment for clustering effect
was conducted.
Results
Practice recruitment is presented in Figure 1.
From 128 eligible practices, 63 were recruited
with 31 randomised to the intervention group
(A) and 32 to the control group (B). Groups A, B
and C (non-recruited practices) were similar with
respect to the socioeconomic status of the practice
locations and the average practice size. The num-
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Figure 2. Babies born in practice groups during the study period
ADHB
11 555 babies born
Intervention (A)
practices
2842 (24.6%) babies
Pre-call
delivered
1198 (10.4%)
babies
Control (B)
practices
2414 (20.9%) babies
No nominated
practice
472 (4.1%) babies
Non-participating (C)
practices
5827 (50.4%) babies
Pre-call not
delivered
1644 (14.2%)
babies
ber of babies born in the ADHB between 1 November 2008 and 20 April 2010 (a one year 5.75
month period) was 11 555 (see Figure 2). This is
7834 babies per calendar year, which was close
to our estimate of 8000 babies per year for the
128 eligible general practices. Half of the eligible
practices (63) were enrolled in the study, and
close to half (46%) of the babies were nominated
to these practices. There were slightly more babies born to the control (B) than the intervention
(A) practices. A small number of infants (n=472,
4%) had no nominated practice.
from the NIR in time, practice nurses stopping
the intervention for periods of time (for example during the summer period when there were
locum nurses), plus one A practice failed to deliver any interventions at all. In many instances
details were not recorded as to whether or not
the intervention included a five-week pre-call or
seven-week recall as well as the four-week precall mail-out, so sub-analyses of how often these
were required was not possible.
The overall coverage rate for the six week vaccine
‘1’ (INFANRIX® hexa) for A, B and C practices
delivered on time by eight weeks of age was
98%—see Table 2. This was also the case for
vaccine 2 (Prevenar ®). Scatter plots of the difference in timing between v1 and v2 for all cases
Only 1198 of the 2842 babies in the A practices
received pre-call interventions (42%). The reasons
for these not being delivered included practices
not receiving or being aware of the notification
Table 2. Overall vaccination rate for six week event for vaccine 1 for intervention, control, non-participating and no nominated practice
Type of
practice
Six week vaccine 1 received
by age eight weeks
Opted off /
Declined
No NIR data
Total
% completed by
practice type
A
2743
53
46
2842
97
B
2388
26
0
2414
99
C
5744
83
0
5827
99
D1
32
16
0
48
67
D2
0
0
424
424
0
10 907
177
470
11 555
% by A, B
or C only
98%
% overall
94%
Key:
A = Intervention practice
B = Control practice
C = Non-participating practice
D1 = No nominated practice, six week immunisation data available
D2 = No nominated practice, six week immunisation data not available
v1 = INFANRIX® hexa
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE193
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Figure 3. Differences in timing between vaccines 1 and 2 for six week vaccination event
and then for those in practices A and B showed
that these were rarely given separately; hence,
separate analyses for v1 and 2 were not required.
See Figure 3 for scatter plots for the six week
events which shows a straight line when time of
delivery of vaccine 1 is plotted against time of
delivery of vaccine 2.
When the 472 children with no nominated practice (D) were included in the total, the overall
vaccination rate completed by eight weeks of age
for the six week vaccination dropped from 98% to
94%. Table 3 shows the average age of receipt of
INFANRIX® hexa at six weeks, three months and
five months by practice type for children receiving immunisations. It can be seen that non-participating practices (C) consistently had a slightly
longer average delay than recruited practices (A
and B), but children without a nominated practice
who were vaccinated had a much greater average
delay. While the majority (88%) of the babies
attended the practice their parents nominated at
birth, 12% were either vaccinated or declined vaccination at a different practice for vaccine 1 at the
six week event.
We analysed data both using the second and
third dose assumptions (e.g. if the three month
dose was recorded in the NIR, we assumed the
six week event had been given) and not making
this assumption but categorising these children as
having no information on the six week vaccination
event. This made a slight difference in coverage
rates. When applied to immunisation registers, the
third-dose assumption results in an over-estimate
of immunisation coverage that is smaller than the
underestimate produced by assuming all those
with missing data have not been immunised.29
When the vaccination times of A and B practices
for receipt of the six week vaccine were compared (intention-to-treat analysis), there was no
indication of a difference between the groups
(Log Rank (Mantel-Cox): Chi-square 0.268, df=1,
p=0.605). There also was no difference in days
to vaccination for the three month vaccine event
(Log Rank (Mantel-Cox): Chi-square 0.540, df=1,
p=0.46) nor for the five month vaccine (Log Rank
(Mantel-Cox): Chi-square 0.281, df=1, p=0.60).
Table 3. Average age of receipt of INFANRIX® hexa at six weeks, three months and five months by practice type
Practice
type
Average age in weeks of
receiving six week v1
Average age in months of
receiving three month v1
Average age in months of
receiving five month v1
A
7.06
3.40
5.64
B
7.09
3.43
5.65
C
7.26
3.48
5.7
D
8.92
4.49
6.32
Key:
A = Intervention practice
B = Control practice
C = Non-participating practice
D = No nominated practice
v1 = INFANRIX® hexa
194
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
However, this analysis did not take into consideration the fact that the 58% of children in the A
practices did not receive the intervention.
We therefore conducted a second analysis looking
at vaccination in group A, stratifying by actual
delivery of the intervention. This showed that
babies receiving the intervention were statistically more likely to receive their six week vaccination event earlier (Log Rank (Mantel-Cox):
Chi-square 19.187, df=1, p<0.001) with mean
days to six week vaccination event 49.6 days
for those who received interventions compared
with 51.2 days for those who did not—see
Figure 4. An advantage of this analysis is that
it takes into account types of censored data, for
example where six week data is missing but the
third dose assumption is used. The same pattern
was repeated for vaccination coverage stratified
by delivery of intervention for A practices for
the three month vaccination event (Log Rank
(Mantel-Cox): Chi-square 16.527, df=1, p<0.001)
with mean days 100.1 compared with 103.8, and
for the five month event (Log Rank (Mantel-Cox):
Chi-square 11.621, df=1, p=0.001) with mean
days 166.2 compared with 170.1.
A third analysis comparing only those babies in
the A practices who had received the intervention with the group B babies found a similarly
significant result for the six week vaccination
event results (Log Rank (Mantel-Cox): Chi-square
5.969, df=1, p=0.015), the three month (Log
Rank (Mantel-Cox): Chi-square 10.722, df=1,
p=0.001) and the five month (Log Rank (MantelCox): Chi-square 6.753, df=1, p=0.009).
While there was no statistical difference in
timeliness between A and B groups, we expected
that recruited practices (A and B) would have less
delay in immunisation overall than C practices
which declined to participate (and may be less focused on vaccination). We therefore repeated the
timeliness analysis including group C for the six
week vaccine. We found that group C practices
had a significantly more delayed vaccine rate for
the six week vaccine (Log Rank (Mantel-Cox):
Chi-square 14.705, df=1, p=0.001).
Lastly, analysis of practice surveys found that
13 A and 12 B practices used some form of
pre-call prior to the trial. All but one A practice
(which had failed to use the pre-call intervention)
intended to continue using our pre-call intervention post-trial.
Discussion
At the commencement of our study in 2008, NZ
immunisation rates were estimated from the NIR
data to be 88% for the six week vaccine event,
75% for the three month event and 60% for the
Figure 4. Days to six week vaccination event in Group A stratifying by actual delivery of the intervention
Comparison of time to vaccination comparing intervention delivered or
not delivered
Log of comparison of time to vaccination comparing intervention
delivered or not delivered to demonstrate differences
The window for ‘timely’ six week vaccination is 6–10 weeks (42–70 days)
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE195
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
five month event. We calculated our sample size
based on these data. However, we found the coverage rate for enrolled children in all practices in
the study was much higher than expected, at 98%
for the six week vaccine and dropped off very little for the three month and five month doses.
We did find a statistically significant improvement in timeliness of vaccine receipt at the
six week, three month and five month events
comparing children who received the intervention
with those who had not, but because the coverage rates were so high, this only translated into
children receiving the vaccine on average one day
earlier (from 49.5 days to 50.5 days for the vaccine
due at 42 days), which is not clinically significant.
Given that there were much higher coverage rates
across all practices to start with, the lack of clinical significance is not surprising.
While the average coverage among all the ADHB
practices was 98%, there was a small percentage of
infants without nominated practices (n=472, 4%).
Thirty-three percent of infants with no nominated practice for whom there was an entry for the
six week vaccination event were not vaccinated.
When these infants were added to the total, the
overall coverage rate dropped to 94%. This is an
important finding. Infants with no nominated
general practices are much less likely to get immunised and, if they do, are much more likely to
be delayed. This reduces the overall coverage rate
significantly for the region (making the general
practices look as though they are performing less
well than they are). Children who are not getting
general practice services including immunisation pre-call and/or recall can be considered to be
‘falling through the cracks’: Attention needs to be
given to this group of children, both encouraging
earlier general practice enrolment for them and
targeting outreach services for those unenrolled.
We identified a number of places where errors
occur in the collection of data in the NIR: the
practitioner (usually the practice nurse) may enter
incorrect data in the PMS, there may be technical problems with the transfer of data from the
PMS to the NIR, the NIR might send back error
messages to the practitioners’ inboxes that they
do not know how to action, a practitioner may not
196
know how to manage entry of complex ‘catchup’ schedules when a child is presenting late or
has received a different immunisation regime in
another country, or the PMS might not have the
facility to record these complex immunisation
entries accurately. An unvaccinated child presenting at three months may have this immunisation
event recorded as the three month rather than the
six week vaccination event. Furthermore when
patients transfer practices it is usually not possible
for their full clinical records to be transferred
electronically between practices. This means that
the new practice needs to manually enter previous vaccines from paper records or the child well
health book, which will not always be available.
How our findings relate to
what is already known
Timeliness of children’s vaccination varies
widely between and within countries.30–39 There
are a range of factors associated with timeliness reported in these studies. Ethnicity, area of
residence21,40,41 and negative media coverage are all
associated with delay in vaccination.36
Integrated systems including outreach and recall
has been shown to be effective. For example, an
extensive programme in Chicago which combined
immunisation education at birth with ongoing
reminder–recall achieved over 90% on-time adherence for recommended immunisations among
inner-city children aged 0–35 months.42 Having
a nurse vaccine manager who is in charge of
tracking inventory, training staff, and developing
vaccination protocols can improve timeliness of
vaccine delivery.43
Our study shows that enrolment and early
engagement with a general practice is resulting in
excellent coverage and timeliness. However the
children not enrolled with a general practice fare
poorly and represent a small but significant group
for whom outreach services should be targeted,
and assistance given for the infant to join a general practice.
Strengths and limitations
We piloted the intervention set-up, received early
datasets for testing, performed dummy runs, dou-
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
ble-entered data and performed meticulous data
cleaning to ensure we had an accurate dataset to
analyse.
However, we recruited fewer practices to the
study (63/128, 50%) than the 60% we had
intended and we had delays in some practices
implementing the intervention. The intervention was only delivered to 42% of the eligible
children in the intervention practices, plus some
of the practices reported that they were already
doing some form of recall; hence, the comparison
between intervention and control group had no
significant difference. We had incomplete records
of whether or not the delivered intervention
included five-week pre-call or seven-week recall
contacts.
Recommendations
As a result of this study we recommend that NIR
notify general practices so that they are aware of
all newborns for whom the practice is the nominated provider as soon as possible after birth, and
that DHBs follow up newborns with no nominated providers to ensure registration with a provider
as early as possible. Different regions will use
different strategies to achieve this. We further
recommend that practices send a pre-call letter
with accompanying information about immunisation when infants are aged four weeks, as a fully
automated prompt system followed by telephone
contact if the family does not make contact seems
to be a cost-efficient and sensible strategy. Because
many Auckland practices are already doing some
form of pre-call, having a standardised four-week
pre-call letter prompt system that all practices
could use may have a positive effect on timeliness. It could assist those practices who are not
pre-calling and act as a reaffirmation to those
practices who are pre-calling that their current
commitment is worthy of continuing.
Conclusion
We found immunisation coverage and timeliness for infants receiving the primary series of
immunisations among their nominated Auckland
general practices to be extremely high, with no
clinically relevant room for significant improvement. The intervention trialled in this study
made a statistically significant improvement to
timeliness of vaccination; however, only by one
day. However, coverage was significantly lower
among infants with no nominated practice and
this reduced the overall coverage rate. Non-enrolment of babies at birth with a general practice is a
significant factor in delayed or missed immunisations. Targeting both the systems and services
that can identify and track these infants has the
greatest potential to improve immunisation coverage rates even further.
References
1. Ministry of Health. The National Childhood Immunisation
Coverage Survey 2005. Wellington; 2007.
2. Ministry of Health. Immunisation handbook 2006. Wellington:
Ministry of Health; 2006.
3. Grant C, Roberts M, Scragg R, Stewart J, Lennon D, Kivell
D. Delayed immunisation and risk of pertussis in infants:
unmatched case-control study. BMJ. 2003;326:852–3.
4. Kolos V, Menzies R, McIntyre P. Higher pertussis hospitalization rates in indigenous Australian infants, and delayed
vaccination. Vaccine. 2007;25(4):588–90.
5. Singleton R, Bulkow LR, Levine OS, Butler JC, Hennessy
TW, Parkinson A. Experience with the prevention of invasive
Haemophilus influenzae type b disease by vaccination in
Alaska: the impact of persistent oropharyngeal carriage. J Ped.
2000;137(3):313–20.
6. Grant C, Scragg R, Lennon D, Ford R, Stewart J, Menzies R.
Incomplete immunisation increases the risk of pertussis in
infants. BMJ. 2003;326:852–3.
7. Somerville RL, Grant CC, Grimwood K, et al. Infants hospitalised with pertussis: estimating the true disease burden. J Paed
Child Health. 2007 Sep;43(9):617–22.
8. Greenberg DP, Doemland M, Bettinger JA, et al. Epidemiology of pertussis and Haemophilus influenzae type b disease
in Canada with exclusive use of a diphtheria-tetanus-acellular
pertussis-inactivated poliovirus-Haemophilus influenzae
type b pediatric combination vaccine and an adolescent-adult
tetanus-diphtheria-acellular pertussis vaccine: implications for
disease prevention in the United States. Pediatr Infect Dis J.
2009;28(6):521–8. doi: 10.1097/INF.0b013e318199d2fc.
9. Crowcroft NS, Pebody RG. Recent developments in pertussis.
Lancet. 2006 Jun 10;367(9526):1926–36.
10. Anonymous. Pertussis epidemic in New Zealand, 1990/1991.
Commun Dis NZ. 1991;91(9):88–9.
11. Bobo JK, Gale JL, Thapa PB, Wassilak SG. Risk factors for
delayed immunization in a random sample of 1163 children
from Oregon and Washington. Pediatrics. 1993;91(2):308–14.
12. Guyer B, Hughart N, Holt E, et al. Immunization coverage and
its relationship to preventive health care visits among innercity children in Baltimore. Pediatrics. 1994;94(1):53–8.
13. Williams IT, Milton JD, Farrell JB, Graham NM. Interaction of
socioeconomic status and provider practices as predictors
of immunization coverage in Virginia children. Pediatrics.
1995;96(3 Pt 1):439–46.
14. Farizo KM, Cochi SL, Zell ER, Brink EW, Wassilak SG, Patriarca
PA. Epidemiological features of pertussis in the United States,
1980–1989. Clin Infect Dis. 1992 Mar;14(3):708–19.
15. Wood D, Donald Sherbourne C, Halfon N, et al. Factors
related to immunization status among inner-city Latino and
African-American preschoolers. Pediatrics. 1995;96(2 Pt
1):295–301.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE197
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
ACKNOWLEDGEMENTS
Thanks to the general
practices involved in the
study for their valuable
cooperation and assistance
in making this study
possible and, in particular,
the practice nurses precalling the children at the
intervention practices.
We appreciate the
valuable advice provided
to us by our Stakeholder
Advisory Board on design
and delivery of the
intervention. Thanks also
to Mr Charles Misquitta
and Ms Janine Peters at
Auckland District Health
Board (ADHB) for their
assistance with the ADHB
National Immunisation
Register (NIR), Mr Mishra
Suryaprakash at the
Ministry of Health (MoH)
for communication with
the National Immunisation
Register Governance
Group, members of the
NIR Governance Group
for approving this study,
Rachel Guthrie, Population
Event Registers Team
Lead, MoH, for assistance
with accessing NIR
data, Deirdre McMahon
and Dipan Ranchhod
(Data Quality Analyst),
National Collections Data
Management Sector
Services, MoH, for
assistance with NIR data,
and to Dr Lynn Taylor,
Operations Manager of
IMAC for information on
potential errors occurring
between practice and
NIR messaging.
FUNDING
This study was funded
by the Health Research
Council of New Zealand
and the Ministry of Health.
COMPETING INTERESTS
None declared.
198
16. Strine TW, Luman ET, Okoro CA, McCauley MM, Barker LE.
Predictors of age-appropriate receipt of DTaP Dose 4. Am J
Prev Med. 2003;25(1):45–9.
17. Grant CC, Turner NM, York DG, Goodyear-Smith F, PetousisHarris HA. Factors associated with immunisation coverage and timeliness in New Zealand. Br J Gen Pract. 2010
Mar;60(572):e113–20.
18. Samad L, Butler N, Peckham C, Bedford H. Incomplete
immunisation uptake in infancy: maternal reasons. Vaccine.
2006;24(47–48):6823–9
19. Fields V, Sumpter C, Seagraves L, Laney A, Lott A, McBride
K. Determining factors affecting parental non-compliance
with vaccination schedules of children ages 6 months to 2
years. La Grange College; 2007. Available from: http://www.
lagrange.edu/resources/pdf/citations/2007/nursing/nursing%20-%20fields.pdf
20.Tickner S, Leman PJ, Woodcock A. Factors underlying
suboptimal childhood immunisation. Vaccine. 2006;24(49–
50):7030–6.
21. Trauth JM, Zimmarman RK, Musa D, Mainzer H, Nutini JF. Do
beliefs of inner-city parents about disease and vaccine risks
affect immunization? J Nat Med Assoc. 2002;94(9):820–32.
22.Wroe A, Turner N, Salkovskis PM. Understanding and predicting decisions about early childhood immunisations. Health
Psych. 2004;23(1):33–41.
23. Pattison H, Pareek M. Health professionals’ attitudes to MMR
vaccine. Advice in primary care affects parents’ decision to take
up MMR vaccination.[comment]. BMJ. 2001;322(7294):1121.
24. Petousis-Harris H, Goodyear-Smith F, Soe B, Turner N. Family
practice nurses perspectives on barriers to childhood immunisation. Vaccine. 2005;23:2725–30.
25.Briss PA, Rodewald LE, Hinman AR, Shefer AM, Strikas RA,
Bernier RR, Carandekulis VG, Yusuf HR, Ndiaye SM, Williams
SM. Reviews of evidence regarding interventions to improve
vaccination coverage in children, adolescents, and adults. Am
J Prev Med. 2000 January 2000;18(1):97–140.
26.Goodyear-Smith F, Grant C, York D, et al. Determining immunisation coverage rates in primary health care practices:
A simple goal but a complex task. International J Med Inform.
2008;77:477–85.
27. Desmond N, Grant C, Goodyear-Smith F, Turner N, PetousisHarris H. Nurses make a difference in immunisation service
delivery. Aust J Adv Nurs. 2011;28(4):31–5.
28.Immunisation Advisory Centre. New Zealand National Immunisation Schedule from 1 September 2008. Auckland, 2008. 1 p.
29. Hull B, Lawrence G, MacIntyre C, McIntyre P. Estimating immunisation coverage: is the ‘third dose assumption’ still valid?
Commun Dis Intell. 2003;27:351–61.
30.Clark A, Sanderson C. Timing of children’s vaccinations in
45 low-income and middle-income countries: an analysis of
survey data. Lancet. 2009 May 2;373(9674):1543–9.
31. Luman ET, Barker LE, McCauley MM, Drews-Botsch C. Timeliness of childhood immunizations: a state-specific analysis. Am
J Pub Health. 2005 Aug;95(8):1367–74.
32. Luman ET, McCauley MM, Stokley S, Chu SY, Pickering LK.
Timeliness of childhood immunizations. Pediatrics. 2002
November 1, 2002;110(5):935–9.
33. Cotter JJ, Bramble JD, Bovbjerg VE, et al. Timeliness of
immunizations of children in a Medicaid primary care case
management managed care program. J Nat Med Assoc.
2002;94(9):833–40.
34.de Nuncio MLZ, Nader PR, Sawyer MH, De Guire M, Prislin R,
Elder JP. A prenatal intervention study to improve timeliness of
immunization initiation in Latino infants. J Community Health.
2003;28(2):151–65.
35. Hull BP, McIntyre PB. Timeliness of childhood immunisation in
Australia. Vaccine. 2006;24(20):4403–8.
36.Dannetun E, Tegnell A, Hermansson G, Torner A, Giesecke
J. Timeliness of MMR vaccination—influence on vaccination
coverage. Vaccine. 2004;22(31–32):4228–32.
37. Luman ET, Barker LE, Shaw KM, McCauley MM, Buehler
JW, Pickering LK. Timeliness of childhood vaccinations in the
United States: days undervaccinated and number of vaccines
delayed. JAMA. 2005 Mar 9;293(10):1204–11.
38.Bailie RS, Si D, Dowden MC, et al. A systems approach to
improving timeliness of immunisation. Vaccine. 2009 Jun
2;27(27):3669–74.
39. O’Grady K-A, Krause V, Andrews R. Immunisation coverage
in Australian indigenous children: time to move the goal posts.
Vaccine. 2009 Jan 7;27(2):307–12.
40.Dombkowski KJ, Lantz PM, Freed GL. The need for surveillance of delay in age-appropriate immunization. Am J Prev
Med. 2002;23(1):36–42.
41. Ehresmann KR, White KE, Hedberg CW, et al. A statewide
survey of immunization rates in Minnesota school age
children: Implications for targeted assessment and prevention
strategies. Ped Infect Dis J. 1998;17(8):711–6.
42. Vora S, Verber L, Potts S, Dozier T, Daum RS. Effect of a
novel birth intervention and reminder-recall on on-time immunization compliance in high-risk children. Hum Vac. 2009
Jun;5(6):395–402.
43. Joyce C. Steps to success: getting children vaccinated on time.
Ped Nursing. 2007 Nov–Dec;33(6):491–6.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
PSA testing in general practice
Fraser Hodgson MBChB, DipObst, FRNZCGP, PGCertTravMed, PGDipPHC; Zuzana Obertová PhD; Charis
Brown BCom, MIndS, PhD; Ross Lawrenson MBBS, MD, FRCGP, FAFPHM, FFPH.
Waikato Clinical School,
The University of Auckland,
Hamilton, New Zealand
ABSTRACT
INTRODUCTION: In New Zealand, prostate-specific antigen (PSA) testing has increased significantly
(275 000 tests/year). Controversy exists around PSA testing as part of an unorganised screening programme.
AIM: To look at the use of PSA testing in a sample of general practices and investigate the reasons GPs
undertake PSA testing.
METHODS: Five Waikato general practices investigated looking at PSA laboratory tests of men ≥40
years in 2010 compared against GP notes. Testing rates, reasons for testing, histology and referral/s were
examined for different age groups. A questionnaire was sent to the GPs to determine their views on PSA
testing.
RESULTS: One in four men aged 40+ years had a PSA test in 2010. Of these men, 71% were asymptomatic. More than half of men tested aged 70+ years were asymptomatic. Ten percent of all PSA tests were
elevated. Twenty-one of 23 prostate cancers were diagnosed following an elevated PSA test: more than
80% of these men had histories of prostate pathology or lower urinary tract symptoms. The questionnaire confirmed that GPs believe in the benefits of PSA screening and it also showed they had difficulty in
providing patients with information about pros and cons of PSA testing.
DISCUSSION: All GPs in this study tested asymptomatic men. GPs in this study value PSA screening and
believe that it reduces mortality rates. However, although PSA tests were most frequently done on asymptomatic patients, the majority of patients subsequently diagnosed with prostate cancer had been tested
because of symptoms or had previous prostate problems.
KEYWORDS: Prostate specific antigen (PSA); PSA testing; screening; prostate cancer; general practitioners
Introduction
Prostate cancer is a common cause of male cancer
in New Zealand with approximately 3000 new
cases diagnosed each year and 560 deaths.1 The
natural history of prostate cancer is that it usually occurs in older men. It is slowly progressive
with a long lead-time to diagnosis and symptoms.
Five-year survival rates are also high at more than
80%.2–4 The long lead-time prior to symptoms
suggests prostate cancer to be a good candidate
for screening. The PSA test is helpful as a management tool in patients with established prostate
cancer; despite its limitations it is also used as a
screening tool, being relatively cheap and simple
to use.5
General practitioners (GPs) face conflicting
messages about the need to screen. The Urological Society of Australia and New Zealand
believe GPs should offer asymptomatic men
a PSA test.6 This advice is partly based on
the results of two randomised control trials,
the European Randomized Study of Screening for Prostate Cancer (ERSPC) and Prostate,
Lung, Colorectal, and Ovarian (PLCO) Cancer
Screening Trial.7,8 The ERSPC study has
shown reduced mortality in men who were
screened between the ages of 50 and 69 years.8
However, because of the acknowledged global
issues of over diagnosis and harm caused by
screening, the NZ Ministry of Health has fol-
J PRIM HEALTH CARE
2012;4(3):199–204.
CORRESPONDENCE TO:
Fraser Hodgson
Waikato Clinical
School, The University
of Auckland, PB 3200
Hamilton, New Zealand
f.hodgson@auckland.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE199
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 1. The number and percentage of men who received a PSA test, had an elevated PSA and had been referred to a
specialist in a 12-month period in five general practices by age
Age group
Had PSA test
Years
n
%
PSA raised
%
n
%
Total
n
40–49
241
12.4
6
2.5
2
33.3
1938
50–59
481
26.7
38
7.9
16
42.1
1802
60–69
415
35.7
48
11.6
21
43.8
1161
70–79
244
35.2
32
13.1
11
34.4
694
80+
99
30.7
23
23.2
5
21.7
323
Total
1480
25
147
9.9
55
37.4
5918
lowed the trend in other OECD countries and
has avoided making recommendations supporting a national screening programme.5,9
in the Waikato region during a 12-month period
and to understand why they are being tested. We
also examined the outcomes of testing.
What are GPs to do? Patients typically have a
very straightforward understanding of the PSA
test. A negative test means they do not have
cancer, while a positive test will identify cancer
early enough to allow curative treatment. They
believe the risks of having a simple blood test are
minimal.10 However, several studies confirm that
patients’ perception of risk are not accurate.11,12
Methods
In New Zealand, it is known that PSA tests are
used widely, with 275 000 tests a year being carried out principally ordered by GPs.13 In general,
GPs would test asymptomatic men, but many
tests are also being undertaken in men with
lower urinary tract symptoms (LUTS) or previous
history of prostate problems.14–19 What has not
been recorded is why men are tested and what
happens to the men who have been tested and are
found to have a raised PSA level.
This study was designed as a pilot for a larger project looking at costs and complications of screening. This pilot was to be run within the Waikato
District Health Board. The Waikato region is a
large geographical area covering 34 890km2 or
approximately 13% of New Zealand’s land mass,
with a population of 353 000. There are a number
of main urban areas in the region, including
Hamilton. A characteristic of this region is the
number residing in rural and isolated areas (23.8%
compared with 14.3% for the total population).20
The aim of this study is to examine the age-specific rate of PSA testing in five general practices
200
Referred to specialist
n
This study was carried out in five Waikato-based
general practices with a total population of approximately 25 000 registered patients. The practices
were purposefully selected to be representative of
both rural and urban practice. Ethics approval was
obtained (reference number NTY/11/02/019). Practices were approached by the lead author, provided
information on the content of the study and then
invited to be part of the project. GP permission was
sought to access PSA test results for all enrolled
men aged 40 years and older from their practice
who had received a PSA test result during 2010.
Once permission was received, the laboratory
provided all PSA results for the given period
attached to the GP and the practice. In-house GP
patient records were reviewed to determine the
reason the PSA test was performed. These were
coded under four broad categories:
1. Opportunistic testing (e.g. done with blood
tests for acute or non-related chronic problems,
e.g. cardiovascular risk assessment (CVRA),
flu injection, non-specific check-up etc.)
2. Previous raised PSA or prostate problems
(including prostate cancer, prostatitis, benign
prostatic hyperplasia)
3. Patient request (patient with no symptoms)
4. Patient had evidence of lower urinary tract
symptoms (LUTS), including retention, reduced
flow, nocturia, urgency, frequency, haematuria,
dribbling, and erectile dysfunction.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Each practice provided baseline data of their population of enrolled men aged 40 years and over,
date of birth, ethnicity, and National Health
Index (NHI) number. The age and PSA levels of
those tested were recorded.
We analysed the data looking at testing rates
by age and reason for testing. We also analysed
referral rates to specialists for those with a raised
PSA test. A raised PSA was defined according to
Pathlab recommendations:
• 40–49 years >2.5ug/L
• 50–59 years >3.5ug/L
• 60–69 years >4.5ug/L
• 70–79 years >6.5ug/L
• 80+ years >7ug/L.
WHAT GAP THIS FILLS
What we already know: Despite ongoing debate regarding the benefits
of PSA screening in general practice, PSA testing is frequently done, and the
majority of tests can be considered screening rather than as an aid to diagnosis in men with symptoms.
What this study adds: While many studies have asked GPs for their
views regarding screening of asymptomatic patients, this study reviewed not
only GPs’ testing activity but also looked at their subsequent management.
An important finding was that a considerable proportion of PSA screening is
performed in men aged 70+ years despite the fact that international advisory
groups discourage screening in older men since it is known to cause harm
and there is no evidence of reduced mortality in men aged over 70 years.
Results
Data were entered into an Excel spreadsheet that
included date of birth and reason for testing for
all men 40 years and older. In addition to reasons
for PSA testing, details such as digital rectal
examination, referrals, biopsies, complications,
treatment, diagnosis date, stage/Gleason/extent
were all captured.
A questionnaire survey was later sent to the GPs
in the practices to ascertain their views regarding PSA testing. Each question had a choice of
five responses from ‘strongly agree’ through to
‘strongly disagree’. It included questions such as
‘I believe that PSA screening will improve mortality rates for prostate cancer’; ‘I am concerned
about the harm caused to men due to PSA screening for prostate cancer’; ‘I believe that the benefit
of screening outweighs any harm’; and ‘It is difficult to give a balanced view to patients regarding
the pros and cons of PSA testing.’ Demographic
information was also collected.
We identified 5918 resident male patients aged 40
years and older in the five practices. During the
12 months 1480/5918 (25%) had been tested with
at least one PSA test. The range varied 10–37%
over the five practices. Testing was least likely in
the 40–49 year age group and declined slightly in
the 80+ year age group (see Table 1).
Overall 147/1480 (10%) PSA tests were elevated
(Table 1). In those with an elevated PSA, 55 out
of 147 (37%) were referred to a specialist. Of the
55 referrals, 39 had a biopsy, 21 out of these had
prostate cancer, and 18 were benign (Table 2).
However, there were 10 referrals to specialists
with normal PSA test results. These had reasonable clinical grounds (LUTS and/or abnormal
DRE) to do so (Figure 1). Two men who were
biopsied had prostate cancer.
When we looked at the notes to ascertain the
reason patients had a PSA test overall, 71% of the
Table 2. Number of men with raised PSA test, referral, biopsy, and diagnosed with prostate cancer grouped by reason for
PSA test
Reasons for PSA test
Raised PSA test
Referral
Biopsy
Diagnosis of
prostate cancer
Opportunistic testing
28
6
5
4
Previous prostate problems
98
40
29
14
Patient requested test
2
1
0
0
LUTS
19
8
5
3
Total
147
55
39
21
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE201
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Figure 1. Patients with normal PSA level referred to a specialist and their outcomes
Reasons for referral
• 6 with lower urinary tract symptoms > 1 biopsy > 1 diagnosed with prostate
cancer
• 1 with abnormal digital rectal examination > 1 biopsy > 1 diagnosed with
prostate cancer
• 2 with previous prostate cancer and rising but normal PSA level > no biopsy
• 1 with elevated PSA in 2009 and upper normal range PSA in 2010 > no biopsy
Figure 2. Proportion (%) of reasons for PSA test in five general practices by patients’ age
70 years. Only 44% agreed that all men over
40 should have at least one PSA test. Seventytwo percent of GPs said they did a digital rectal
examination and PSA test when checking for
prostate cancer.
Certain questions looked at consultation restraints surrounding PSA explanations. Thirtynine percent of the GPs felt they needed more
knowledge to advise patients. Fifty-six percent
felt it was difficult to give a balanced view to
patients regarding PSA testing. The majority felt
patients had difficulty understanding the issues
despite the GP’s best efforts, and 61% said that
patients elected to get the test anyway. However,
the majority did not feel pressured by patients to
perform PSA screening. GPs were evenly divided
in their views regarding such things as medicolegal concerns, time restraints and whether
patients could in fact make up their own minds
about PSA testing.
Discussion
time GPs did this opportunistically; 14.3% when
there was a history of prostate problems; 3.9% on
patient request; 10.8 % with lower urinary tract
symptoms (Figure 2).
GP questionnaire results
Of the 26 GPs in the five practices, 18 questionnaires were returned (69%): 10 male and 8 female.
The majority worked five or more sessions in joint
practices and were aged in their 40s and 50s.
Sixty-one percent agreed or strongly agreed that
PSA screening reduced mortality rates. Fifty-five
percent were concerned regarding harm caused
by PSA testing, but the majority felt the benefits
outweighed this. All bar one GP did PSA screening: mostly selectively and/or opportunistically,
mainly focused on men aged between 50 and
202
All doctors in the five general practices involved
in the study were testing asymptomatic patients.
This was confirmed by the GP questionnaire, in
which all bar one GP said they practised screening. Testing of asymptomatic men is common
in New Zealand and this seems to be consistent
with findings in other countries.15–17 Many studies have asked GPs and primary care doctors for
their views regarding screening of an asymptomatic patient; we have gone one step further in
this study and identified why men are tested.
In our study, 25% of men 40 years and over were
tested in 2010. Testing rates increased with age
and GPs focused most of their screening on men
aged between 50 and 69 years. This may in fact
be worthwhile as the ERSPC study showed up
to 20% reduction in mortality in men in this age
group.8 What is of concern in our study is the
number of PSA tests done on patients aged 70+
years. A large number of these tests (56%) were
done opportunistically when there is no evidence
to support a mortality benefit in this age group.
The National Screening Advisory Committee
identified that nearly 50% of men 40 years and
over had had a PSA test at some time, which
compared to only 18% during 2008.21 In a 2011
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Health Committee inquiry into the early detection and treatment of prostate cancer, 50% of men
50 years and over were estimated to have a PSA
test over a two-year period.22 The New Zealand
Health Survey suggests that approximately 50%
of men aged 50 and over had a PSA test in the
previous five years, of which 80% were asymptomatic.23 This represented a 40% coverage rate in
New Zealand in any one year. Our study found
that there was a 25% chance of having a PSA test
in 2010 if 40 years and over. If we limit it to 50
years and over the chance is 31%. These figures
are consistent with the above-mentioned reports.
Our GPs generally believed that the benefits of
PSA testing outweighed harm and resulted in
reduced mortality rates.
Ten percent (147/1480) of men who had a
PSA tests in 2010 showed an elevated level of
PSA. Management of these patients reflect the
uncertainty over the value of PSA testing as a
screening tool. Fifty-five out of 147 (37%) men
were referred to a specialist (mostly urologist),
which at face value seems to be a low referral
rate. It seems that many men with raised PSA
tests are initially managed with repeated PSA
tests, rather than proceeding directly to referral.
As this study had only a limited follow-up period
we cannot comment on how many patients may
eventually require a referral and biopsy.
1000 PSA tests done for patients with previous
prostate problems (including previously elevated
PSA), approximately 66 new prostate cancers
would be identified. There would be 18 new
cancers for patients presenting with LUTS, while
only four new cancers for every 1000 tests done
opportunistically (i.e. those without symptoms
or previous prostate problems). Therefore, when
diagnosing prostate cancer it seems worthwhile if
GPs focus their PSA testing on men with previous history of prostate problems or LUTS.
GPs within our study reported that they find
explanation to patients about PSA screening
difficult. Most seem convinced that screening is beneficial although evidence supporting
improved mortality rates in the 70+ years age
groups is lacking. More education for GPs may
prove worthwhile.
One of the strengths of this study was that it
was population based and that the researchers
were able to link patient data with laboratory
data. Collection of detailed data directly from
clinical notes by the same researchers, one of
whom was a clinician, is considered a strength.
Seeking GP views via a questionnaire and
relating these findings to practice was likewise
believed to be a positive strength.
In our sample, we observed that younger patients
(40–69 years) were more likely to be referred
(42.4%) and to have a biopsy (79.5%) than older
men (29.1% referred, and 31.3% biopsied, respectively). In total, 39 out of 55 men with elevated
PSA (71%) underwent a biopsy; 21 new cases of
prostate cancer were identified. In addition, there
were 10 referrals to a specialist in the absence of
raised PSA. There seemed to be reasonable clinical grounds (LUTS and/or abnormal DRE) to do
so. Two of these 10 men were biopsied, both of
whom proved to have cancer.
Weaknesses of this study could include the selection of practices which might not reflect a true
representation of current practice. We also had
lower numbers of Maori men than we were hoping to find, precluding analysis by ethnicity. GP
questionnaire numbers were small and may not
be representative of the New Zealand population.
This study did not look at follow-up after biopsy
and any risk or benefits from the diagnosis of
prostate cancer. These aspects are being followed
up by the larger, three-year Midland Prostate
Cancer Study of which this study represents the
pilot stage.
We looked at the reasons for having the PSA
test done and checked whether this was helpful
in identifying men with prostate cancer. Having
a previously raised PSA or history of a prostate
problem together with a raised PSA proved to be
the most productive in identifying prostate cancer. From our study it is estimated that for every
In conclusion, this study looked at PSA testing
by GPs in five practices in the local Waikato setting. GPs in this study believed in the benefits of
screening and were opportunistically testing, focusing their screening on men aged 50–69 years.
They were more likely to refer and there was
a greater chance of identifying prostate cancer
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE203
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
when PSA testing was done on men with previous history of prostate problems or LUTS. Using
their clinical judgment, GPs identified further
prostate cancer cases even when PSA levels were
within normal ranges.
This study has provided useful findings that are
informing a larger study on the management of
men with prostate cancer.
References
FUNDING
The authors would like
to thank their funders,
the Waikato Medical
Research Foundation
(project number:
003626510) for their
support of the project.
COMPETING INTERESTS
None declared.
204
1. Ministry of Health. New registrations and deaths 2006.
Revised edition. Wellington; 2010.
2. Hardie C, Parker C, Norman A, Eeles R, Horwich A, Huddart
R, Dearnaley D. Early outcomes of active surveillance for localized prostate cancer. BJU Int. 2005;95:956–60.
3. Roemeling S, Roobol MJ, Postma R, Gosselar C, van der Kwast
TH, Bangma CH, Schröder FH. Management and survival of
screen-detected prostate patients who might have been suitable for active surveillance. Eur Urol. 2006;50:475–82.
4. Roemeling S, Roobol MJ, De Vries SH, Wolters T, Gosselaar
C, van Leenders GJLH, Schröder FH. Active surveillance for
prostate cancers detected in three subsequent rounds of
a screening trial: characteristics, PSA doubling times, and
outcome. Eur Urol. 2007;51:1244–50.
5. Greene KL, Albertsen PC, Babaian RJ, Carter HB, Gann PH,
Han M, Kuban DA, Sartor AO, Stanford JL, Zietman A, Carroll
P. Prostate Specific Antigen Best Practice Statement: 2009
Update. J Urol. 2009;182:2232–41.
6. Urological Society of Australia and New Zealand PSA Testing
Policy 2009. [cited 2011 Nov 9]. Available from: www.usanz.
org.au/uploads/29168/ufiles/USANZ_2009_PSA_Testing_Policy_Final1.pdf
7. Andriole GL, Crawford ED, Grubb RL, Buys SS et al. Mortality
results from a randomized prostate-cancer screening trial. N
Engl J Med. 2009;360:1310–9.
8. Schröder FH, Hugosson J, Roobol MJ, Teuvo LJ et al. Screening and prostate-cancer mortality in a randomized European
study. N Engl J Med. 2009;360:1320–8.
9. New Zealand Guidelines Group. Testing for prostate cancer. Information for men and their families. Ministry of Health; 2008.
10. Evans R, Edwards AGK, Elwyn G, Watson E, Grol R, Brett J,
Austoker J. ‘It’s a maybe test’: men’s experiences of prostate
specific antigen testing in primary care. Br J Gen Pract.
2007;57(537):303–10.
11. Arroll B, Pandit S, Buetow S. Prostate cancer screening:
knowledge, experiences and attitudes of men aged 40–79
years. N Z Med J. 2003;116(1176):U477.
12. Avery KN, Blazeby JM, Lane JA, Neal DE, Hamdy FC, Donovan JL. Decision-making about PSA testing and prostate
biopsies: a qualitative study embedded in a primary care
randomised trial. Eur Urol. 2008;53(6):1186–93.
13. Best Practice Advocacy Centre (BPAC). Annual Pharmaceutical & Laboratory Report; 2009.
14. Drummond FJ, Carsin AE, Sharp L, Comber H. Factors prompting PSA-testing of asymptomatic men in a country with no
guidelines: a national survey of general practitioners. BMC
Fam Pract. 2009;10:3.
15. Durham J, Low M, McLeod D. Screening for prostate cancer:
a survey of New Zealand general practitioners. NZ Med J.
2003;116(1176).
16. Gavin A, McCarron P, Middleton RJ, Savage G, Catney D,
O’Reilly D, Keane PF, Murray LJ. Evidence of prostate cancer
screening in a UK region. BJU Int. 2004;93:730–4.
17. Hicks RJ, Hamm RM, Bemben DA. Prostate cancer screening. What family physicians believe is best. Arch Fam Med.
1995;4(4):317–22.
18. Jonler M, Eddy B, Poulsen J. Prostate-specific antigen testing
in general practice: a survey among 325 general practitioners
in Denmark. Scand J Urol Nephrol. 2005;39:214–8.
19. Little B, Ho KJ, Gormley G, Young M. PSA testing in general
practice. Prostate Cancer Prostatic Dis. 2003;6(2):154–8.
20.Pool I, Baxendine S, Cochrane W, Lindop J. New Zealand regions, 1986–2001: population geography. Population Studies
Centre Discussion Papers 54; October 2005.
21. Sneyd DMJ. Prevalence of opportunistic prostate cancer
screening in New Zealand. A report for the National Screening
Advisory Committee; 2010.
22.Inquiry into early detection and treatment of prostate cancer.
Report of the Health Committee; 2011.
23.Ministry of Health. A portrait of health: key results of the
2006/07 New Zealand Health Survey. Wellington; 2008.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
The incidence of acute otitis media in
New Zealand children under five years
of age in the primary care setting
Barry Gribben MBChB, MMedSci, FRNZCGP;1 Lesley J Salkeld MBChB, FRACS, FRCSC, DipABO;2
Simon Hoare MBChB, DCH, MD, FRACP, FRCPCH;3 Hannah F Jones MBChB, Dip Paed4
CBG Health Research
Limited, Auckland,
New Zealand
1
ABSTRACT
INTRODUCTION: Acute otitis media (AOM) is a common childhood infection. Baseline data are required to evaluate potential changes in the epidemiology of AOM with new public health measures.
AIM: To estimate the incidence of AOM in children under five years of age in primary care in New Zealand.
METHODS: Using a cohort study design, consultation notes from 1 November 2008 to 31 October 2009
from 63 primary care facilities were analysed for new and recurrent episodes of AOM, complications,
antimicrobial use and outcome.
Paediatric Otolaryngology,
Starship Hospital, Auckland
2
Paediatrics, North Shore
Hospital, Auckland
3
Paediatrics, Starship
Hospital, Auckland
4
RESULTS: There were 19 146 children in the sample. The raw incidence of AOM was 273 per 1000
children (27.3%; 95% CI 216–330). Of the 3885 children, 2888 (74%) had one episode of AOM and 152
(4%) of these children developed recurrent AOM. Incidence declined with age. There was no difference
in incidence between Maori, Pacific and ‘Other’ ethnicities. Antibiotics were used to treat 2653 (51%)
AOM episodes and 113 (4.3%) of these children re-presented within three days of antibiotic therapy for
persistent symptoms. Tympanic membrane perforation was the only complication noted, observed in 62
(1%) episodes.
DISCUSSION: These data indicate that AOM is an important and frequent childhood infection in New
Zealand. The show a significant decline in the use of antibiotics to manage AOM in concordance with
accepted best practice. The complication rate of AOM is likely under-represented. This study enables
future research into the effectiveness of current and future immunisations and changing management
practices in New Zealand.
KEYWORDS: Otitis media; incidence; child, preschool; New Zealand, antibiotic
Introduction
Acute otitis media (AOM) remains a frequent
global infection of childhood, with up to 80%
of children having at least one episode by three
years of age.1 Ten to 30% have recurrent episodes,2,3 and 2–25% will have persistent middle
ear effusion extending beyond three months,1
many of which require tympanostomy tube insertion.4,5 Persistent tympanic membrane perforation
and otorrhoea are significant issues, particularly
in specific populations.5–7 Otitis media and
eustachian tube disorders are the third leading
diagnosis in GP consultations between 0 and 14
years,8 and myringotomy and tube insertion the
most frequent childhood surgical procedure in
the USA.9 AOM is also the commonest reason for
prescribing antibiotics to children in developed
countries,2 contributing to concerns of emerging
antibiotic resistance.6
The current incidence of AOM in New Zealand
is not known. Tilyard et al. reviewed otitis media
(OM), including AOM, treatment in general prac-
J PRIM HEALTH CARE
2012;4(3):205–212.
CORRESPONDENCE TO:
Hannah F Jones
Paediatric Registrar,
Starship Hospital,
PB 92024, Auckland
1142, New Zealand.
hannahj@adhb.govt.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE205
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 1. Geographic distribution and proportion of subjects in the study population by District Health Board
Study population
n
Population under five years of age
N
Proportion of the DHB population
included in study (%)
Auckland
1480
28680
5
Bay of Plenty
1697
14410
12
Canterbury
780
33290
2
Capital & Coast
136
19440
1
Counties Manukau
2686
41200
7
Hawkes Bay
1824
11290
16
Hutt Valley
877
10620
8
Lakes
466
8050
6
MidCentral
354
11470
3
Nelson Marlborough
461
8545
5
District Health Board
Northland
1357
11240
12
Otago
1771
10550
17
South Canterbury
267
3285
8
Southland
0
7890
0
Tairawhiti
1015
3905
26
Taranaki
294
7675
4
Waikato
1097
27070
4
Waitemata
1950
37290
5
Wairarapa
0
2680
0
West Coast
395
2125
19
239
4370
5
19146
305075
Whanganui
All
tice in New Zealand from 1993 to 1994 across
all age groups,10 and Ryan et al. surveyed the
management of AOM by GPs further in 2002.11
Historical studies show rural Maori children
have some of the highest rates of chronic suppurative otitis media (CSOM) in the world.12–14 A
more recent New Zealand study demonstrated an
incidence of 3871 hospital admissions for OM per
100 000 of the population of children under five
years of age, with higher rates of medical admissions amongst Maori and Pacific children.15
The incidence of AOM may have been affected
by the introduction of a pneumococcal conjugate
vaccine (PCV7) to New Zealand in June 2008.
There has been a modest reduction in incidence
of all-cause AOM in clinical trials of this vaccine in other countries.16,17 A new pneumococcal
conjugate vaccine that targets the two predominant bacterial pathogens of AOM (Streptococ-
206
cus pneumoniae and non-typeable Haemophilus
influenzae) has been correlated with a greater
effect based on an AOM clinical efficacy study
with a precursor formulation.18 This new vaccine
was due to replace the PCV7 immunisation in the
NZ immunisation schedule in 2011.
The term ‘acute otitis media’ as used throughout
this paper can be interpreted as symptomatic,
rapidly forming purulent fluid in the middle ear
cleft which occasionally results in rupture of the
previously intact eardrum causing discernable
otorrhoea. ‘Otitis media with effusion’ (OME),
meaning inflammation associated with fluid
behind an intact eardrum without signs and
symptoms of an acute infection, is not addressed
in this study. ‘Chronic suppurative otitis media’,
where alluded to, describes dry perforations,
draining cholesteatomas or chronic discharge via
a perforation. ‘Otitis media’ is used generally to
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
describe inflammation of the middle ear without
regard to aetiology.
In this study, we have examined the current incidence of AOM in New Zealand preschool children presenting to primary care. We also assessed
clinical features (including secondary complications and recurrent disease), antimicrobial use,
and treatment failures. These data are important
for resource management and establishing the
impact of current and future vaccines.
Methods
This cohort study reviewed children less than
five years of age enrolled in a sample of general
practitioner (GP) practices in New Zealand from
1 November 2008 to 31 October 2009.
The study used the random sample of GP
practices enrolled in HealthStat, an established
primary care surveillance system in New Zealand
(See Appendix 1 in the web version of this
paper).19 The 93 GP practices participating in the
HealthStat surveillance panel at the time of the
study were invited to take part. Sixty-seven of
these practices responded, 63 practices accepted
the invitation and four declined.
These 63 practices had 261 835 patients enrolled
at the time of the study. Children were eligible
for the study if they were under five years of
age on 1 November 2008 and were continually
enrolled in a participating practice from 1 November 2008 to 31 October 2009; 19 146 eligible
children were retrospectively enrolled in the
study. The geographical distribution of the study
population by District Health Boards (DHBs) is
detailed in Table 1. Nineteen of the 21 DHBs
were represented in the study.
Anonymous data are automatically downloaded
weekly from the HealthStat practice databases,
using an encrypted messaging system. These
data include dates of all consultations, diagnostic
coding (and other classifications if recorded by
clinicians), prescriptions, laboratory results and
demographic data. Although up to three ethnicities were collected for each patient, only one
ethnicity was coded per patient with precedence
given for Maori, then Pacific, then ‘Other’.
WHAT GAP THIS FILLS
What we already know: Acute otitis media (AOM) represents significant
disease burden amongst children worldwide. Antibiotics are frequently prescribed for AOM although in most clinical scenarios this is no longer considered best practice. New immunisations targeted at common AOM pathogens
have been associated with a decreased incidence of AOM in international
studies.
What this study adds: This study presents an estimate of the incidence
of AOM in children in New Zealand, and the demographics of the affected
population and the management of AOM in primary care. It provides a baseline for future analyses of the impact of existing and new immunisations on
the incidence of AOM and of changes in the management of AOM in primary
care in New Zealand.
Data on the incidence of AOM were collected
by a review of the text of clinical notes written during the study period. All notes with
terms that either related to otological disease
(e.g. ‘AOM’, ‘OM’, ‘bulging’) or to an otological
history or examination (e.g. ‘ear’, ‘drum’, ‘tymp’)
were electronically selected for analysis: a list of
the search terms is given in Appendix 2 in the
web version of this paper. These notes were then
reviewed by a team of research nurses. Ambiguous terms were interpreted in context, e.g.
‘tymps’ was either understood to mean tympanic
membrane(s) or tympanogram. In addition to
these records, a random sample of 100 records
from each practice was reviewed for idiosyncratic
abbreviations that indicated a possible otological
problem. When a new abbreviation was found,
all notes from all the practices were re-examined
for the new term.
Episodes of AOM were coded for diagnostic
certainty according to the clinical evidence provided (Table 2). If a research nurse had difficulty
coding a consultation in terms of diagnosis or
diagnostic certainty, the consultation record was
examined by the senior research nurse and, if
necessary, a GP.
All consultation notes reviewed by the research
nurses were examined to determine whether the
case related to a new episode of AOM, recurrent AOM, ‘treatment failure’ or complicated
AOM. A new episode of AOM was defined
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE207
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 2. Ranking of criteria for the identification of acute otitis media based on terms used
in the consultation notes
Level*
Criteria
Level 1
AOM subjects defined as children (<5 yrs) with diagnosis of AOM/OM.
Level 2
AOM subjects defined as children (<5 yrs) with diagnosis of AOM/OM and
at least two clinical signs or symptoms: fever, otalgia, bulging tympanic
membranes, or otorrhoea.
Level 3
AOM subjects defined as children (<5 yrs) with diagnosis of AOM/
OM and/or clinical signs or symptoms (fever, otalgia, bulging tympanic
membrane, otorrhoea) and microbiological results (S.pneumoniae culture
positive, H. influenzae culture positive, serotype results if available).
*The higher the level, the greater the degree of clinical evidence supporting the diagnosis
Table 3. Age, gender and ethnicity demographics of patients in study sample, with
comparison to the New Zealand population
Study population
NZ population 2009
N (%)
N (%)
23 109 (8.8)*
362 858 (8.4)
Male
9730 (50.9)
156 465 (51.3)
Female
9416 (49.2)
148 610 (48.7)
Maori
6358 (33.2)
86 930 (28.5)
Pacific
1485 (7.8)
33 735 (11.1)
Other
11 303 (59.0)
18 4410 (60.4)
p
assessed no improvement in symptoms after 48
hours of antibiotic therapy.
From the collected data, the raw incidence of new
episodes of AOM was calculated using the following equation:
Incidence = Number of new AOM episodes in children
<5 years of age during the study period
Total number of children <5 years of age
in the study cohort from 2008 to 2009
Further data analyses were performed using
SAS 9.2. The confidence intervals were calculated
using SAS proc surveymeans (using the Wald
method) to estimate the average number of AOM
per child, allowing for clustering of children
within practices.
Age
0–5
Results
Gender
0.1982
Ethnicity
0.0001
* Includes children five years old at 1 November 2008 who were excluded from the final study sample.
as an episode of AOM following a 30-day
symptom-free interval. Therefore consultation
notes from 1 October 2008 to 31 October 2008
were also reviewed to ensure these patients had
not been consulted for middle ear symptoms in
the 30 days prior to diagnosis. Recurrent AOM
described three or more new episodes of AOM
within six months or four or more new episodes
of AOM within one year. ‘Complicated AOM’
was limited to complications which arose during
the study period. Perforations were only included
as a complication if there was AOM and a visible
perforation on the same day. A tympanostomy
tube was not regarded as a perforation. Otorrhoea alone or in the presence of a tympanostomy tube was not considered a complication.
The prevalence of tympanostomy tube insertions
was beyond the scope of this study. A case was
considered ‘treatment failure’ if the physician
208
Between 1 November 2008 and 31 October 2009,
19 146 children younger than five years old were
identified in participating practices representing
19 out of 21 DHBs. The demographics of the
study versus the New Zealand population are
shown in Table 3.
The number of consultations for AOM identified
was 6261. Of these, 5225 related to new episodes
of AOM. Hence, the incidence of AOM was 273
episodes per 1000 (27.3%) children under five
years of age per annum (95% CI 216–330). The
incidence definition includes multiple episodes
of new AOM for the same child. The majority
of children (74%) affected by AOM had only
one episode of AOM during the study period
(Table 4). Approximately 20% of children had two
cases of AOM and nearly 7% had three or more
cases in the 12-month analysis.
These episodes were stratified by age, gender
and ethnicity (Table 5). The incidence was
highest in children less than one year old and
significantly declined with age. There were no
significant ethnic group–related differences.
Eighty-two percent of episodes met level 2 diagnostic criteria. Less than 1% of cases fulfilled
level 3 diagnostic criteria, which required a
microbiological result obtained from otorrhoea
or tympanocentesis.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 4. Number of new episodes of acute otitis media per child from 1 November 2008 to 31 October 2009
New episodes
of AOM
Number of
children (N)
Total number of
episodes (n)
Percentage of children with
number of episodes (%)
1
2888
2888
74.3
2
731
1462
18.9
3
199
597
5.1
4
58
232
1.5
5
8
40
0.2
6
1
6
0.0
3885
5225
All
Recurrent AOM was identified in 152 children,
comprising 4% of all the children who had at
least one episode of AOM (Table 6). Recurrent
AOM was most frequently diagnosed in younger
subjects; 6.5% children under one year of age
developed recurrent AOM in comparison to less
than 1% of four-year-old children.
Fifty-one percent of the AOM episodes were
treated with antibiotics. In 4.3% of treated
episodes, the child re-presented with persistent
symptoms within three days of their initial
presentation. The only complication noted in this
study was visible perforation, present in 62 (1%)
episodes.
Discussion
This retrospective study is the first major analysis of AOM incidence in young New Zealand
children. It emphasises the major frequency,
impact and socioeconomic burden of AOM. Two
hundred and seventy-three episodes per 1000
children per annum is an incidence comparable
Table 5. Incidence of AOM by age, gender and ethnicity
Number of
children (N)
Number of new AOM
episodes (n)
Percentage incidence of
episodes (%)
95% CI (%)
Age*
<1
3485
1740
49.9
39.8-60.0
1
4091
1377
33.7
25.8-41.4
2
3951
836
21.2
16.0-26.2
3
3733
688
18.4
13.7-23.1
4
3886
584
15.0
12.1-18.0
All
19146
5225
27.3
21.6-33.3
9416
2496
26.5
21.0-31.9
Gender
Female
Male
9730
2729
28.0
22.1-32.8
All
19146
5225
27.3
21.6-33.3
11303
3187
28.2
21.1-35.3
Maori
6358
1721
27.1
20.7-33.4
Pacific
1485
317
21.3
12.9-29.8
All
19146
5225
27.3
21.6-33.3
Ethnicity
Other
* At 1 November 2008
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE209
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
to other developed countries, although differences in study methodology need to be considered.1,3,20–25 This study includes the first six
months of PCV7 immunisation in New Zealand,
but predates the introduction of vaccines with
increased serotype coverage and activity against
other pathogens such as non-typeable Haemophilus influenzae.
The gender distribution of the sample was
comparable to the New Zealand population,
but the ethnicity distribution significantly differed, with Maori being over-represented and
Pacific children under-represented. However,
calibration of the raw incidence to the New
Zealand population by gender and ethnicity
has minimal effect on the estimated incidence
(i.e. 271/1000 children per annum). Applying
Approximately half of the AOM episodes were
treated with antibiotics. This is a significant
decrease from a 96.6% prescription rate in Tilyard’s
New Zealand study from 1993 to 1994, and the 95%
rate self-reported by GPs in Ryan’s study in 2002.
this rate to the New Zealand population (July
2009 projection) suggests there are 83 000 new
episodes of AOM annually in children less
than five years of age.
The majority of diagnoses (82%) were well supported by at least two documented signs or symptoms, an accepted degree of diagnostic certainty
across studies.1,17,26 There were only three cases of
Level 3 diagnostic certainty, as tympanocentesis
(penetration of the tympanic membrane to aspirate middle ear contents for diagnostic purposes)
is not a routine procedure in primary care in
New Zealand.
The decline in incidence of new episodes of
AOM with age is consistent with international
studies.1,16,20,27 There was no significant difference
in the incidence of AOM across ethnic groups
210
in this study. This was an unexpected finding
as risk factors for otitis media (such as exposure
to second-hand smoke and lower breastfeeding
rates)28 are more prevalent in the Maori population, and a high prevalence of CSOM in Maori
has been previously reported.12–14 Maori children
have a greater ‘unmet need’ for GP services than
non-Maori,28 which may have contributed to
lower AOM rates than anticipated. For children
of Pacific ethnicity, recent research showed 1.9%
of two-year-old Pacific children investigated for
chronic otitis media were incidentally diagnosed
with AOM.29
The incidence of recurrent acute otitis media
was lower than reported in other studies, but an
inverse association between recurrent AOM and
age was still demonstrated.1,2 One explanation
for the lower incidence is that children in the
study, although enrolled in the participating GP
practices, may have presented to other general
practices throughout the year.
The occurrence of complicated acute otitis media
may be under-represented in this study. ‘Mastoiditis’ and other complications were not search
terms used to detect AOM; therefore, complications were only identified if they were simultaneously present with features of AOM during the
study period. In addition, New Zealand children
with complex disease (e.g. mastoiditis, absence of
clinical improvement, out-of-hours deterioration)
often present directly to non-GP services such as
hospital emergency departments. The only complications identified were 62 visible perforations.
In some instances these may have been chronic
perforations with acute otorrhoea.
Local data from Starship Hospital (the referral
centre for acute otorhinolaryngology services
for approximately one quarter of New Zealand’s paediatric population) indicate there
were 59 admissions consistent with mastoiditis
in children less than five years of age from
1 January 2005 to 31 December 2009.30 The
incidence was disproportionately represented
amongst Maori and Pacific populations (30.5%
(18/59) New Zealand Maori, 27.1% (16/59)
Pacific, 42.4% (25/59) ‘Other’) compared with
population statistics 28.5% Maori, 11.1% Pacific,
60.4% ‘Other’.30
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Table 6. Number of cases of recurrent AOM by age
Recurrent episodes
Number of children
with three AOM
episodes in
six months (N)
Number of children
with four AOM
episodes in
one year (N)
Number of children
with non-recurrent
AOM (N)
Proportion of children
with AOM diagnosed
with recurrent AOM (%)
<1
38
38
1085
6.5
1161
1
27
18
962
4.5
1007
2
12
6
651
2.7
669
3
7
2
546
1.6
555
Age
Total number of
children with ≥1
episode of AOM (N)
4
1
3
489
0.8
493
All
85
67
3733
3.9
3885
Approximately half of the AOM episodes were
treated with antibiotics. This is a significant decrease from a 96.6% prescription rate in Tilyard’s
New Zealand study from 1993 to 1994, and the
95% rate self-reported by GPs in Ryan’s study in
2002.10,11 This decreasing trend complies with
evidence for the management of AOM in developed countries with the exception of children
less than six months of age for whom antibiotics are still recommended.26,31 It also compares
favourably with international antibiotic prescription rates.20,23 Starship Children’s Hospital data
over five years does not reflect an increasing
rate of mastoiditis with the decrease in antibiotic therapy.30 All antibiotics prescribed were
presumed to be oral antibiotics. The use of topical
antibiotics as an adjunct or alternative to oral
antibiotics or the presence of concurrent otitis
externa was not reviewed.
Limitations of this retrospective study include
the lack of independent assessment of the
diagnoses and the bias inherent in reviewing
and interpreting medical records. Although over
90% of children nationally are able to see their
GP when needed,28 some children may have
presented to emergency departments, mobile ‘ear
clinics’, or general practices not registered as their
primary health care provider. This would lead
to an underestimation of AOM incidence and
related complications.
Only two-thirds of the invited general practices
agreed to participate in the study. This is likely
because of the short recruitment period, as study
participation rates are typically around 90%. Some
practices do not routinely accept study invitations
before they have been discussed at practice meetings, which may occur only quarterly. In spite of
this, our study sample represented over 6% of the
New Zealand population.
This study demonstrates the importance of AOM
in New Zealand children and creates baseline
data to enable future analysis of the effect of
changing management practices, including the effectiveness of current and future immunisations
on the burden of AOM disease.
References
1. Teele DW, Klein JO, Rosner B. Epidemiology of otitis
media during the first seven years of life in children in
Greater Boston: a prospective, cohort study. J Infect Dis.
1989;160(1):83–94.
2. Rovers MM, Schilder AGM, Zielhuis GA, Rosenfeld RM. Otitis
media. The Lancet. 2004;363(9407):465–73.
3. Liese J CA, Cantarutti L, Silfverdal S-A, Fuat A, Vollmar J,
Pircon J-Y, Rosenlund M. Incidence of acute otitis media
in young children seen in European medical practices. 6th
World Congress of the World Society for Pediatric Infectious
Diseases. 18–22 November, 2009.
4. American Academy of Family Physicians, OtolaryngologyHead and Neck Surgery, American Academy of Pediatrics
Subcommittee on Otitis Media With Effusion. Otitis media
with effusion. Pediatrics. 2004;113(5):1412–29.
5. Morris PS, Leach AJ. Acute and chronic otitis media. Pediatr
Clin North Am. 2009 Dec;56(6):1383–99.
6. Vergison A, Dagan R, Arguedas A, Bonhoeffer J, Cohen R,
Dhooge I, Hoberman A, Liese J, Marchisio P, Palmu AA, Ray
GT, Sanders EA, Simoes EA, Uhari M, van Eldere J, Pelton
SI. Otitis media and its consequences: beyond the earache.
Lancet Infect Dis. 2010 Mar;10(3):195–203.
7. O’Connor TE, Perry CF, Lannigan FJ. Complications of otitis
media in indigenous and non-indigenous children. Med J Aust.
2009 Nov 2;191(9 Suppl):S60–4.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE211
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
FUNDING
We wish to acknowledge
GlaxoSmithKline (GSK)
for providing the funding
for this study. GSK
manufactures the new
pneumococcal conjugate
vaccine which targets
the two predominant
bacterial pathogens of
AOM (Streptococcus
pneumoniae and nontypeable Haemophilus
influenzae).
COMPETING INTERESTS
None declared.
212
8. Top 5 diagnoses at visits to office-based physicians and hospital outpatient departments by patient age and sex: United
States, 2008. National Ambulatory Medical Care Survey
and National Hospital Ambulatory Medical Care Survey. In:
Centers for Disease Control and Prevention NCHS, editor.
Atlanta 2008.
9. Owings MF, Kozak LJ. Ambulatory and inpatient procedures in the United States, 1996. Vital Health Stat. 1998
Nov;(139):1–119.
10. Tilyard MW, Dovey SM, Walker SA. Otitis media treatment in New Zealand general practice. N Z Med J. 1997 Apr
25;110(1042):143–5.
11. Ryan J, Giles M. Management of acute otitis media by
New Zealand general practitioners. NZ Med J. 2002 Feb
22;115(1148):67–9.
12. Giles M, O’Brien P. Otitis media and hearing loss in the children of the Ruatoki valley: a continuing public health problem.
NZ Med J. 1989 Apr 12;102(865):160–1.
13. Giles M, Asher I. Prevalence and natural history of otitis media
with perforation in Maori school children. J Laryngol Otol.
1991 Apr;105(4):257–60.
14. Giles M, O’Brien P. The prevalence of hearing impairment
amongst Maori schoolchildren. Clin Otolaryngol Allied Sci.
1991 Apr;16(2):174–8.
15. Milne RJ, Van der Hoorn S. Burden and cost of hospital
admissions for vaccine-preventable paediatric pneumococcal disease and non-typable Haemophilus influenzae otitis
media in New Zealand. Appl Health Econ Health Policy.
2010;8(5):281–300.
16. Fireman B, Black SB, Shinefield HR, Lee J, Lewis E, Ray P. Impact of the pneumococcal conjugate vaccine on otitis media.
Pediatr Infect Dis J. 2003 Jan;22(1):10–6.
17. Eskola J, Kilpi T, Palmu A, Jokinen J, et al. Efficacy of a pneumococcal conjugate vaccine against acute otitis media. N Engl
J Med. 2001;344(6):403–9.
18. Prymula R, Peeters P, Chrobok V, Kriz P, Novakova E, Kaliskova
E, Kohl I, Lommel P, Poolman J, Prieels J-P, Schuerman L.
Pneumococcal capsular polysaccharides conjugated to
protein D for prevention of acute otitis media caused by both
Streptococcus pneumoniae and non-typable Haemophilus
influenzae: a randomised double-blind efficacy study. Lancet.
2006;367(9512):740–8.
19. HealthStat Primary Healthcare Intelligence. Available from:
http://www.healthstat.co.nz/.
20.Plasschaert AI, Rovers MM, Schilder AG, Verheij TJ, Hak E.
Trends in doctor consultations, antibiotic prescription, and
specialist referrals for otitis media in children: 1995–2003.
Pediatrics. 2006 Jun;117(6):1879–86.
21. Morris PS, Leach AJ, Silberberg P, Mellon G, Wilson C, Hamilton E, Beissbarth J. Otitis media in young Aboriginal children
from remote communities in Northern and Central Australia: a
cross-sectional survey. BMC Pediatr. 2005;5:27.
22.Wolleswinkel-van den Bosch JH, Stolk EA, Francois M, Gasparini R, Brosa M. The health care burden and societal impact
of acute otitis media in seven European countries: results of an
Internet survey. Vaccine. 2010 Nov 19;28 Suppl 6:G39–52.
23.Grossman Z, Silverman BG, Porter B, Miron D. Implementing the delayed antibiotic therapy approach significantly
reduced antibiotics consumption in Israeli children with first
documented acute otitis media. Pediatr Infect Dis J. 2010
Jul;29(7):595–9.
24. Thomas EM. Recent trends in upper respiratory infections,
ear infections and asthma among young Canadian children.
Health Rep. 2010 Dec;21(4):47–52.
25.Williamson I, Benge S, Mullee M, Little P. Consultations for
middle ear disease, antibiotic prescribing and risk factors for
reattendance: a case-linked cohort study. Br J Gen Pract. 2006
Mar;56(524):170–5.
26.Subcommittee on Management of Acute Otitis Media.
Diagnosis and management of acute otitis media. Pediatrics.
2004;113(5):1451–65.
27. Shaikh N, Hoberman A. Update: acute otitis media. Pediatr
Ann. 2010 Jan;39(1):28–33.
28.Ministry of Health. A focus on the health of Maori and Pacific
children: key findings of the 2006/07 New Zealand Health
Survey. In: Ministry of Health, editor. Wellington: Ministry of
Health; 2009.
29. Paterson JE, Carter S, Wallace J, Ahmad Z, Garrett N, Silva PA.
Pacific Islands families study: the prevalence of chronic middle
ear disease in two-year-old Pacific children living in New Zealand. Int J Pediatr Otorhinolaryngol 2006 Oct;70(10):1771–8.
30.Data courtesy of Decision Support CRD, Starship Children’s
Hospital, Auckland. 2010 Data obtained August, 2010.
31. Glasziou PP, Del Mar CB, Sanders SL, Hayem M. Antibiotics
for acute otitis media in children. Cochrane Database Syst Rev
2004(1):CD000219.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
Does the order of presentation and number
of online resources affect the frequency of
access by learners?
Steven Lillis MBChB, FRNZCGP, MGP, PhD;1 Samantha Murton MBChB, FRNZCGP2
Department of General
Practice & Primary Health
Care, Waikato Clinical School,
University of Auckland,
Hamilton, New Zealand
1
ABSTRACT
INTRODUCTION: Provision of web-based resources is a valuable addition to face-to-face teaching in a
blended learning environment.
AIM: To understand how both order of presentation and number of online resources impacts on the
frequency of access by learners in postgraduate vocational training in general practice.
The Royal New Zealand
College of General
Practitioners, Wellington,
New Zealand
2
METHODS: Information was collected on how many times individual online resources were accessed.
Data regarding access rates for 15 separate topics used in postgraduate general practice vocational training were aggregated. Analysis was on the basis of order of presentation where the mean of percentages
of hits by order of presentation with standard deviations was calculated.
RESULTS: The first four listed resources were accessed at a higher rate than the remainder of the resources. All resources after the first four were accessed at a relatively uniform low rate.
DISCUSSION: It would appear that providing more than four resources per topic is associated with
learner overload. The number of online resources to support face-to-face teaching should be limited to
four. Resource material needs to be carefully considered in terms of how it adds educational value. The
ability of resource material to present a different perspective on a topic and adherence to both curriculum
and assessment objectives are important considerations.
KEYWORDS: Education, medical; education, distance; internet; provision of resources; general practice
Introduction
Online learning has created diverse and innovative delivery mechanisms and an active education research stream.1 Outcomes research on
internet-based learning suggest that enhanced
learning opportunities may be generated, but
there are no time efficiencies gained.2 One
enhanced learning opportunity of e-learning is
the ease of placing education material within
reach of the learner and the self-paced nature of
subsequent learning.3
The availability of online educational material
does not, however, predict how this material will
be used.4 Issues relevant to the use of resources
within online resources include the level of
literacy necessary to incorporate the available
material, the complexity and quantity of material provided and the motivation of students
to use the material.5 Many medical education
courses now utilise both face-to-face small group
learning and internet-based learning within an
integrated and mutually supportive framework
(blended learning). The creation, sharing and
sourcing of this e-content is receiving increasing
focus.6 Guidelines regarding content of e-learning
within this blended environment are available,
but tend to provide broad rather than specific
information, such as not overloading the learner
with content.7
J PRIM HEALTH CARE
2012;4(3):213–216.
CORRESPONDENCE TO:
Steven Lillis
Director of Assessment,
Faculty of Medicine
and Health Science,
University of Auckland,
PB 92019, Auckland,
New Zealand
slillis@wave.co.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE213
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
There is little specific data on how learners access
online resource content within a blended structure. Educators therefore lack important data that
informs on the effect of volume or organisation
of online resource content. This research reports
on rates and patterns of access to online resources
by learners in a blended learning environment.
Methods
All general practice registrars in The Royal
New Zealand College of General Practitioners
(RNZCGP) training scheme enter a year of intensive training that utilises a blended learning environment. Each clinical topic (adolescent medicine,
for example) has both a set of online resources chosen by medical educators as well as several hours
of structured interactive face-to-face learning
with discussion, case studies, guest speakers etc.
The order of presentation of the online resources
within each clinical topic is unplanned.
The online resources are available through a
Moodle platform. Moodle is an open source
learning management system that facilitates
content access and communication for web-based
teaching and learning. The number of online
resources per clinical topic is variable. Data are
collected on each topic, recording the number of
times each of the online resources for that topic
is accessed.
There were 144 registrars in the programme with
approximately 70% being female in the 2011
year in which the data were collected. Data were
available for 15 topics and were aggregated and
anonymised. Each access to, or download of, a
resource by a registrar was considered as a ‘hit’.
For each scaffold, the number of hits for individual resources was calculated as a percentage of
all hits for that scaffold.
Results
There were between five and 32 resources available for each of 15 clinical topics, with a mean
of 15.5 (SD of 6.9). The overall number of hits
per clinical topic varied considerably (487 to
2136). The aggregated data on hits for the top 15
resources across all clinical topics is presented in
Figure 1. The mean of the aggregated data over
15 topics is given with one standard deviation on
Figure 1. Level of access to the 15 most accessed online resources across all clinical topics based on order of presentation
214
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
each side. The first listed resource accounts for
just under 16% of all hits, with an SD of 7%. The
first four resources accounted for 10% or more of
all hits each. Thereafter, the percentage of hits
that each resource attracted was lower.
Discussion
WHAT GAP THIS FILLS
What we already know: Provision of web-based resources is a valuable
addition to face-to-face teaching in a blended learning environment.
What this study adds: The order in which resources are listed significantly dictates the frequency of access of individual resources. Providing
more than four resources per topic is associated with decreased access rates
for subsequently listed resources.
It would be expected that learners may access
resources that are at the beginning of a list more
frequently than those at the bottom of a list and
sheer curiosity may well be the major driver of
exploring what the first-listed resources contain. What is surprising from this research is
how marked this behaviour is. After the fourth
resource, the frequency of access declines and
remains low. Even within the first four listed resources, the order of appearance would appear to
influence the frequency of accessing the material.
that all participants will read them, others may
be provided as a library of material that can be
drawn upon if there is a need, but there is no expectation that all participants will access them. In
this case, as is likely in the majority of blended
educational courses, no distinction was drawn between resources considered essential and others.
The data show that the third resource was more
frequently accessed than the second resource. A
The data also raise questions about the nature
of learning from resources in this environment.
It would be expected that learners may access resources that are at
the beginning of a list more frequently than those at the bottom of a
list and sheer curiosity may well be the major driver of exploring
what the first-listed resources contain. What is surprising from this
research is how marked this behaviour is.
more detailed analysis of the resources was undertaken to seek an explanation for this. If appropriate for the topic of a scaffold, the Best Practice
Advocacy Centre (BPAC) guidelines are included
amongst other resources and guidelines. For three
of the scaffolds, the BPAC guidelines were placed
third in the order of presentation by coincidence.
The hit rate for each of the BPAC guidelines was
high in comparison to other resources and therefore skewed the results.
These data suggest that providing more than
four resources per clinical topic is associated with
learner overload. However, there may be several
reasons for making resources available; some
resources may be provided with the intention
Social learning theory promotes the notion
that cognition is not an individual process.
Rather, learning and knowing are shaped by
both interaction with others and the context of
these interactions.8 Resources within a social
learning context become methods of exploring
different ways of knowing as well as finding
material that suits individual learning styles. As
described by Cook and McDonald, ‘Ultimately,
the rationale for using computers in education
comes not because of any inherent instructional
advantage but because computers facilitate the
use of effective instructional methods’.3 Accordingly, resources should be structured to provide
alternative ways of understanding or cater to
differing learning styles using methods either
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE215
ORIGINAL SCIENTIFIC PAPERS
QUANTITATIVE RESEARCH
not available or inappropriate for face-to-face
learning in small group meetings. As the availability of resources increases due to cooperation
and sharing between institutions and countries,
it will become even more important that careful thought is applied to what resources are
included as part of the curriculum.9
An alternative view is that resources should be
considered carefully for their ability to contribute to learning that is likely to be assessed.
This position is based on the well-researched
premise that what is assessed will drive what is
learned.10,11 A plethora of resources for a curriculum topic, some of which contain conflicting
and contradictory views or where the resource
is of marginal interest, is clearly not examinable
material irrespective of its ability to encourage
deep learning. The response of assessment-driven students will be to avoid committing time to
such learning.
It is suggested that, in planning the use of online
resources in a blended learning environment, the
following guidelines may be helpful:
References
1. Smothers V, Ellaway R, Greene P. The e-learning evolutionleveraging new technology approaches to advance healthcare
education. Med Teach. 2008;30(2):117–8.
2. Cook DA, Levinson AJ, Garside S. Time and learning efficiency
in Internet-based learning: a systematic review and meta-analysis. Adv Health Sci Educ Theory Pract. 2010;15(5):755–70.
3. Cook DA, McDonald FS. E-learning: is there anything special
about the ‘E’? Perspect Biol Med. 2008;51(1):5–21.
4. D’Alessandro DM, Kreiter CD, Peterson MW. An evaluation
of information-seeking behaviors of general pediatricians.
Pediatrics. 2004;113(1 Pt 1):64–9.
5. Hannafin MJ, Hill JR. Resource-based Learning. In: Spector M,
Merrill J, van Merrienboer, Driscoll MP, editors. Handbook of
research on educational communications and technology. 3rd
ed. London: Erlbaum; 2007. p 525–536.
6. Matyas ML. Online teaching resources: where in the WWW
are they? Physiology (Bethesda). 2007;22:68–9.
7. Choules AP. The use of elearning in medical education: a review
of the current situation. Postgrad Med J. 2007;83:212–216.
8. Hill JR, Song L, West RE. Social learning theory and webbased learning environments: a review of research and discussion of implications. Am J Distance Educ. 2009;23:2:88–103.
9. Soula G, Darmoni S, Le Beux P, Renard J Dahamna B, Fieschi
M. An open repositories network development for medical
teaching resources. Studies in health technology and informatics. Stud Health Technol Inform. 2010;160(Pt 1):610–4.
10. Newble DI, Jaeger K. The effect of assessments and examinations on the learning of medical students. Med Educ.
1983.17(3):165–71.
11. Fredericksen N. The real test bias. Influences of testing on
teaching and learning. Am Psychol. 1984;39:193–202.
• Limit the number of resources to four for each
clinical topic unless there are pressing reasons
to include more
• Carefully consider the value of each resource
for its ability to represent an alternative view
of a topic or to cater to different learning
styles
• For each resource, consider if the material is
considered essential or ‘if needed’ and clearly
indicate this difference.
Conclusions
COMPETING INTERESTS
None declared.
216
When lists of resources are provided in a blended
learning environment, the order of presentation
of the resources will substantially affect the rate
at which the resources are accessed. The first four
listed resources are likely to have much higher
access rates than the remainder of the resources.
Resources need to be considered carefully for
how they add value to learning within a social
learning theory, whether the resource is ‘essential’ or ‘if needed’ and the number of resources
should be kept to four or below.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUALITATIVE RESEARCH
Addressing patient alcohol use:
a view from general practice
Thomas Mules;1 Jennifer Taylor;1 Rachel Price;1 Logan Walker;1 Baneet Singh;1 Patrick Newsam;1
Thenmoli Palaniyappan;1 Toby Snook;1 Mahfuzah Ruselan;1 John Ryan;1 Jaishree Santhirasegaran;1
Phoebe Shearman;1 Petronella Watson;1 Richard Zino;1 Louise Signal;1 Geoff Fougere;1 Helen
Moriarty;2 Gabrielle Jenkin1
Department of Public
Health, University of Otago
Wellington, New Zealand
1
ABSTRACT
INTRODUCTION: General practitioners (GPs) have the potential to promote alcohol harm minimisation
via discussion of alcohol use with patients, but knowledge of GPs’ current practice and attitudes on this
matter is limited. Our aim was to assess GPs’ current practice and attitudes towards discussing alcohol
use with their patients.
Department of Primary
Health Care and General
Practice, University of Otago
Wellington
2
METHODS: This qualitative study involved semi-structured, face-to-face interviews with 19 GPs by a
group of medical students in primary care practices in Wellington, New Zealand.
FINDINGS: Despite agreement amongst GPs about the importance of their role in alcohol harm minimisation, alcohol was not often raised in patient consultations. GPs’ usual practice included referral to
drug and alcohol services and advice. GPs were also aware of national drinking guidelines and alcohol
screening tools, but in practice these were rarely utilised. Key barriers to discussing alcohol use included
its societal ‘taboo’ nature, time constraints, and perceptions of patient dishonesty.
CONCLUSION: In this study there is a fundamental mismatch between the health community’s expectations of GPs to discuss alcohol with patients and the reality. Potential solutions to the most commonly
identified barriers include screening outside the GP consultation, incorporating screening tools into
existing software used by GPs, exploring with GPs the social stigma associated with alcohol misuse, and
framing alcohol misuse as a health issue. As it is unclear if these approaches will change GP practice,
there remains scope for the development and pilot testing of potential solutions identified in this research,
together with an assessment of their efficacy in reducing hazardous alcohol consumption.
KEYWORDS: Primary health care; general practice; alcohol drinking; alcohol-related disorders, attitude
of health personnel.
Introduction
Alcohol-related harm is a global problem. In
developed countries, alcohol is responsible for
6.7% of disability-adjusted life years lost and
1.6% of deaths and is increasing.1 In New Zealand
(NZ) more than 1000 deaths every year can be
attributed to alcohol, resulting in 17 000 years
of life lost annually.2 In a recent NZ study, the
proportion of people drinking more alcohol over
the past year had increased from 2% in 1998 to
16% in 2006.3 The worsening of alcohol-related
health problems internationally was realised as
early as 1980, when a World Health Organization
(WHO) expert committee on alcohol stressed the
need for increased efforts to prevent alcohol-related health harms.4 The committee called for the
development of strategies that could be applied in
primary health care settings with a minimum of
time and resources. Primary care was identified as
a key setting for the reduction of alcohol-related
harm, with general practitioners (GPs) considered
J PRIM HEALTH CARE
2012;4(3):217–222.
CORRESPONDENCE TO:
Louise Signal
Associate Professor,
Department of Public
Health, University of Otago
PO Box 7343, Mein St,
Newtown, Wellington,
New Zealand.
louise.signal@otago.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE217
ORIGINAL SCIENTIFIC PAPERS
QUALITATIVE RESEARCH
to be in an ideal position to detect, prevent and
manage patients’ alcohol problems.
A number of advantages of a GP-based strategy
have been identified.5 In addition to there being
good evidence that brief interventions delivered
by GPs have a positive impact on patients’ alcohol
consumption, GPs are readily accessible to the
general population and have role legitimacy in
the delivery of advice about alcohol consumption.5 In most countries people with alcohol problems will first present to their GP6 rather than
to specialist treatment services.7 It is perhaps because of this that there is a growing expectation
that GPs will provide advice concerning lifestyle
issues, including alcohol.8 Evidence in support of
the efficacy of brief GP interventions in this area
has also been accumulating, with longer duration
of counselling having little additional effect.9
alcohol might be somewhat optimistic. Therefore,
this study assessed GPs’ current practice in NZ
(where GP consultation is based on a user-pays
model with discounts for high needs and low
income groups) and attitudes towards addressing
alcohol use with their patients, together with
barriers and supports to such initiatives identified
by GPs.
Methods
A convenience sample of 19 GPs was interviewed
by fourth-year medical students (the primary
authors of the paper) while on a one-week general
practice placement in Wellington, NZ. From 33
invited GPs, 14 declined (58% response rate), 11
because they were too busy, two were not interested and one was ill. GPs came from a variety of
practices including privately owned and not-for-
In addition to there being good evidence that brief interventions
delivered by GPs have a positive impact on patients’ alcohol
consumption, GPs are readily accessible to the general population and
have role legitimacy in the delivery of advice about alcohol consumption.
Despite the weight of evidence in favour of brief
GP-based interventions to address hazardous
alcohol consumption, uptake by GPs is limited.5
A number of challenges to introducing a discussion on alcohol in the GP consultation have been
identified, including time pressure and sensitivity to the issue.5 Consequently, GPs do not
always identify patients with hazardous levels
of alcohol consumption.5,10 An Australian study5
reported that GPs were able to identify only 28%
of patients classified by the Australian Medical
Association criteria as ‘high risk’ drinkers, while
another study found that between 65% and 82%
of patients with alcohol-related problems (identified by consumption levels or screening tests)
were not identified by GPs.11
Taken together, this evidence suggests that the
expectation that GP-led brief interventions could
facilitate significant reductions in harm from
218
profit, central city and suburban, and a range of
socioeconomic areas. This sample was similar to
GPs nationally. The average age of the sample was
47 (compared to 48 nationally), the proportion of
males in the sample was 56% (compared to 59%
nationally), almost half (n=9) had been practising
for over 15 years and the same number worked in
private practice compared to not-for-profit practice
(no national data available for comparison).
A semi-structured interview schedule included
15 open-ended questions covering GPs’ current
practice and attitudes towards discussing alcohol
use with their patients and barriers to, and
support needed to facilitate, such discussions.
Face-to-face interviews were approximately 20
minutes long, tape-recorded with consent, and
transcribed. A thematic analysis12 was undertaken, with initial coding and analysis cross-checked
by other research team members.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUALITATIVE RESEARCH
Ethics approval was received from the Department of Public Health Ethics Committee, University of Otago Wellington.
Findings
Current practice
Discussions with patients
The GPs in this study reported rarely discussing
alcohol in their consultations. Reasons for initiating discussions with patients around alcohol
included:
• suspicious clinical signs (raised by 15 GPs)
• social issues, such as domestic violence,
depression or frequent work absence (mentioned by six GPs), and
• consultations with new patients
(mentioned by six GPs).
Other circumstances mentioned less frequently
were:
• as part of routine questioning
• in the presence of other addictions
• when the presenting complaint
was related to mental health
• when alcohol was a presenting complaint, or
• when alcohol had been raised by
a concerned family member.
Screening
Routine screening for alcohol misuse was not
common practice in consultations conducted
by these GPs. While six GPs screened all new
patients for alcohol misuse, seven GPs reported
rarely screening (all were from private practices
and six had practised for over 15 years). Sixteen
of the GPs who screened relied on a list of verbal
questions (e.g. the CAGE tool—a mnemonic for
attempts to reduce drinking, being annoyed when
criticised about drinking, feeling guilty about
drinking and using alcohol on waking),13 three
used written screening tools (the Alcohol Use
Disorders Identification Test—AUDIT)14 and, two
used liver function blood tests. Of the six GPs
who screened all new patients, four had practised
less than 15 years and five were salaried and from
not-for-profit practices (serving low income popu-
WHAT GAP THIS FILLS
What we already know: General practitioners (GPs) are thought to be
well positioned to reduce alcohol-related harm via discussion of alcohol misuse with patients. GPs identified a number of barriers to discussing alcohol
misuse as well as some potential solutions to these barriers.
What this paper adds: Although GPs in this study thought it was important to discucss alcohol use with their patients, they rarely did so unless the
patient’s drinking had signifant impacts on their health.
lations). All the younger GPs who screened used
a routine set of questions. Fifteen of the 19 GPs
were aware of NZ guidelines for alcohol screening
but 13 did not use them to guide their practice.
The difficulty of raising the issue of alcohol with
patients was noted by a number of GPs and some
had developed tactical ways of approaching the
topic, such as using the screening window (on the
computer) as an excuse for asking: ‘So I’ll say what
we’re supposed to be doing is… asking everybody
how much alcohol they [consume] in a week’ or
‘[we just] need to update our details, are you allergic to anything, do you smoke or drink?’ Doctors
said that patients expect smoking questions so
some bundle alcohol into the same question.
Interventions
GPs identified interventions including GPdelivered advice, referral to drug and alcohol
services, referral to Alcoholics Anonymous,
medication, and family support. Only five GPs
delivered alcohol intervention to patients such
as, ‘counselling [during] the consultation and
talking to the patient about what is a safe level of
alcohol intake’. Many of these GPs found that it
was sometimes very difficult to arrange followup visits as patients would not attend. Almost
all of these GPs reiterated the importance of the
patient’s willingness to talk for discussion to be
successful.
GP attitudes
The role of the GP
GPs in the study agreed that primary care has an
important role to play in delivering primary prevention, including preventing harm from alcohol.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE219
ORIGINAL SCIENTIFIC PAPERS
QUALITATIVE RESEARCH
Eleven GPs felt their own advice about alcohol
was useful to patients, six were undecided, and
two thought it made no difference to patients’
drinking. GPs expressed concern about the number of primary prevention strategies they were
expected to address. Perspectives on what their
role should entail varied and included: raising patient (n=7) and public awareness (n=2), referral to
specialist services (n=7), providing advice (n=5),
and some were unsure (n=5).
Use of screening and guidelines
Overall, GPs in the study thought that opportunistic screening was more effective than routine
screening. Those who used screening questions
found them ‘too rigid’ for the flow of consultation and therefore modified them. Reasons
given for not using guidelines included constant
changes being made to the recommendations,
guidelines not being widely applicable, and a
lack of consistency between different guidelines.
One of the two GPs who used guidelines talked
about the difficulty in staying up to date with
the changes.
Barriers to addressing alcohol
GPs identified a number of barriers to addressing
alcohol use with patients. The most common was
the ‘taboo’ nature of the subject (n=11). As one
GP explained, ‘there are stigmas around [alcohol],
so people don’t necessarily like talking about it’.
This contributes to doctor and patient discomfort.
One GP noted that, ‘if there is clinician discomfort about asking these [alcohol-related] questions,
then they might not ask [the patient]’. Three GPs
stated that they felt asking about alcohol use was
‘intruding into other people’s lives unnecessarily’
and they feared that raising the topic could damage the doctor–patient relationship, making future encounters difficult. Another GP noted that
raising the subject often made patients ‘wince…
and some became defensive’.
Ten GPs identified lack of time as a significant
barrier. One noted that ‘quality alcohol consultation should take… 15 minutes’. Perception
of patient dishonesty was another commonly
identified barrier. Four GPs believed that many
patients were not honest about their alcohol use
220
and therefore doubted the value of questioning patients. One stated that ‘most people halve
their alcohol [consumption]. We were always
taught that you double what people say’. Three
GPs identified that the presence of third parties,
commonly family members, made it inappropriate to raise the issue. Other barriers included the
patient not accepting that their drinking was a
health issue, the GP feeling they did not have
the expertise needed, and the GP being unable to
define a safe level of alcohol consumption to the
patient.
When prompted on specific patient demographics that may act as barriers, a third of GPs in
the study found it difficult to raise the topic of
alcohol with people of differing ethnicity and
gender, and a quarter found it hard to raise with
people of a different age. As one GP stated:
…it is always easier if you’re from a [patient’s]
cultural group because they identify with you and
it is difficult to tell someone from a very different
cultural background about [alcohol]… they are less
likely to listen to what you have to say.
The age barrier was a particular issue with teenage patients who see themselves as ‘bulletproof’,
often ‘don’t discuss [alcohol] with older people’,
and often come with a parent or support person.
The barriers of ethnicity, age and gender were
more commonly identified by less experienced
and younger GPs.
Supports identified by GPs
The majority of GPs (n=13) said that more
support was needed to facilitate discussions of
alcohol use with patients. Four said they did not
need further support and two made no comment.
Four GPs suggested this support should come
from raising public awareness of the adverse
health effects of alcohol. As one GP noted, ‘if it’s
just doctors struggling with this problem it’s not
enough’.
Four GPs, all practising for less than 15 years,
said longer consultations were needed. Four GPs
suggested using standardised questionnaires, ideally administered by nurses prior to the consultation, would save time. One GP suggested that it
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
QUALITATIVE RESEARCH
would be easier if a questionnaire was incorporated into a medical records computer programme.
Discussion
Routine screening of patients by GPs in this
study was uncommon and alcohol use was rarely
discussed with patients in their consultations.
However, nearly a third of GPs screened all new
patients. Slightly over a quarter of GPs delivered
alcohol interventions to their patients, including
GP-delivered interventions, referral and medication. This is despite evidence of the considerable
potential for success.4,5,7,9,15–17 This finding supports earlier work.10
While some GPs in this study were confident in
this arena, most did not address the issue unless
the level of drinking had led to a disease state
that could not be overlooked—a finding consistent with research in this area.18,19 Of the GPs
who screened all new patients, the majority were
younger and nearly all were salaried. This suggests that more recent GP training may encourage, or better equip, GPs to address alcohol issues.
It may also suggest that the work context of salaried GPs is more supportive of alcohol screening
than that of those who work for fee-for-service. It
is possible that GPs in fee-for-service practices are
under more pressure not to offend their patients
in case they go elsewhere.
While GPs agreed there is an important role for
primary care in primary prevention, they were
less clear on what this role was in relation to alcohol. GPs were generally of the view that screening for alcohol misuse should be opportunistic
rather than routine. When raising alcohol use
with patients, some GPs did so following use of
screening tools and alcohol guidelines, and others
relied on clinical or social indicators. The study
suggests that GPs find evidence-based guidelines
and structured questionnaires cumbersome and if
they use them they alter the validated questions.
Barriers to addressing alcohol use with patients
include:
• the taboo nature of the subject
• concern about intruding into people’s lives
• time shortages in consultations
• GP perception of patient dishonesty
• the presence of a third party, and
• the challenge of raising alcohol with people of different ethnicity, gender and age.
Age was a particular issue with teenagers. The
majority of GPs thought more support was
needed, including raising public awareness of the
health effects of alcohol, longer consultations,
screening prior to the consultation, and incorporation of screening tools into medical records
programmes.
These findings suggest the advantages GPs have
in addressing alcohol use with patients that
Paton-Simpson et al.5 identify are not widely
experienced, at least by this study population.
First, GPs may be accessible, but short con-
While GPs agreed there is an important role for
primary care in primary prevention, they were
less clear on what this role was in relation to
alcohol. GPs were generally of the view that
screening for alcohol misuse should be
opportunistic rather than routine.
sultations appear to be a barrier to addressing
alcohol use, although evidence suggests that five
minutes may be all that is required for successful intervention.7 Further, at least in NZ,
access to a GP is still limited for many. Second,
many GPs in this study were not clear about the
legitimacy of their role in alcohol health promotion. This may be in part because alcohol is seen
as a social problem and its discussion therefore
invokes social stigma rather than health issues.
Third, while there is good evidence of effectiveness for GP intervention, many of the GPs in
this study were unaware of, or did not believe,
the evidence. The brief time required and the
fact that brief interventions may be even more
efficacious than specialist treatment9 are messages that GPs need to hear. This research also
confirms and extends earlier research on barriers
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE221
ORIGINAL SCIENTIFIC PAPERS
QUALITATIVE RESEARCH
to progress in this area.10 GPs in the study
provided advice about the support that would
assist them.
This is a small qualitative study; hence, the findings are not generalisable. However, the sample is
similar to the NZ GP population and findings are
consistent with previous NZ research10 and other
research internationally.18,19 The response rate
of 58% may have introduced some bias, as most
of those who declined cited time constraints. It
is possible that these are the GPs most likely to
spend time with patients discussing issues such
as alcohol use, and that this study therefore
underestimates the extent that alcohol issues are
addressed in general practice. Regardless, this research suggests that a substantial number of GPs
in NZ may not routinely address alcohol issues
with their patients.
Conclusions
ACKNOWLEDGEMENTS
The authors would like
to thank the GPs who
participated in the study
for generously giving of
their time and experience.
AUTHOR
CONTRIBUTIONS
The students (TM, JT,
RP, LW, BS, PN, TP, PN,
TS, MR, JR, JS, PS, PW
RZ) participated in the
research design, collected
and analysed the data and
wrote the initial report. LS,
HM and GF initiated the
research and supervised
the researchers at all
stages of the research. GJ
wrote the first draft of this
paper and GJ, LS, HM,
GF and TM contributed
to subsequent drafts and
shared responsibility
for editing the final
version. All authors
have contributed to, and
approved, the final version.
COMPETING INTERESTS
None declared.
222
GPs in the current study rarely discussed alcohol
use with their patients and most did not do so
unless the level of drinking was significantly
impacting on health. GPs thought that discussing alcohol use was important although they
were less clear as to their role in this. These
findings challenge the concept that GPs are well
positioned to deliver community-based alcohol
screening and brief intervention. There are unresolved societal, organisational and interpersonal
barriers which deserve further exploration if GPs
are to provide primary intervention to reduce
alcohol-related harm.
First is the need to legitimate the role of GPs in
this arena, both in the minds of the public and
with GPs. A social marketing campaign that
promotes the health effects of alcohol misuse
and the assistance GPs can provide may encourage patients to approach their doctor, and give
GPs more confidence in raising the issue without
concern that they were intruding in patients’
lives. Second, consideration could be given to
how primary care is organised to promote alcohol
health promotion, for example in terms of accessibility, funding models, time with patients, the
place of screening, and screening prompts. Third,
GP training should build the skills of individual
clinicians including stressing the efficacy of brief
intervention and building their confidence to
undertake it. Addressing these issues will better
equip GPs to help their patients reduce harm
from alcohol misuse. Urgent action is needed if
we are to stem the increasing harm from alcohol.
References
1. World Health Organization. Global health risks: Mortality and
burden of disease attributable to selected major risks. Geneva:
World Health Organization; 2009.
2. Connor J, Broad J, Jackson R, Vander Hoorn S, Rehm J. The
burden of death disease and disability due to alcohol in New
Zealand. ALAC Occasional Publication 23. Wellington; 2005.
3. Wilkins C, Sweetsur P. Trends in population drug use in
New Zealand: Findings from national household surveying of drug use in 1998, 2001, 2003, and 2006. N Z Med J.
2008;121(1274):61–71.
4. World Health Organization. Problems related to alcohol
consumption: report of a WHO expert committee. Geneva,
Switzerland: World Health Organization; 1980.
5. Paton-Simpson G, McCormick R, Powell A, Adams P, Bunbury
D. Problem drinking profiles of patients presenting to general
practitioners: Analysis of alcohol use disorders identification test (AUDIT) scores for the Auckland area. N Z Med J.
2000;113:74-77.
6. Rush B. The use of family medical practices by patients with
drinking problems. Can Med Assoc J. 1989;140:35–39.
7. Anderson P. Alcohol and primary health care. WHO regional
publications. In: WHO regional publications, editor. European
series No. 64: World Health Organization; 1996.
8. Wallace P, Brennan P, Haines A. Are general practitioners doing
enough to promote healthy lifestyle? BMJ. 1987;297:663–68.
9. Kaner EF, Dickinson HO, Beyer FR, Campbell F, Schlesinger
C, Heather N, et al. Effectiveness of brief alcohol interventions in primary care populations (Review). Cochrane
Database Syst Rev 2007(Issue 2):Art. No.: CD004148. DOI:
10.1002/14651858.CD004148.pub3.
10. Moriaty H, Stubbe M, Chen L, Tester R, Macdonald L, Dowell
A, et al. Challenges to alcohol and other drug discussions
in the general practice consultation Fam Pract. 2011. doi:
10.1093/fampra/cmr082.
11. Rydon P, Redman S, Sanson-Fisher R, Reid L. Detection of
alcohol related problems in general practice. J Stud Alcohol.
1992;53:197–202.
12. Green J, Thorogood N. Qualitiative methods for health
research. London: Sage; 2004.
13. Bush B. Screening for alcohol abuse using the CAGE questionnaire. Am J Med. 1987;82(2):231–35.
14. Senft R, Polen M, Freeborn D, Hollis J. Brief intervention in a
primary care setting for hazardous drinkers. Am J Prev Med.
1997;13(6):464–70.
15. Bien T, Miller W, Tonigan J. Brief interventions for alcohol
problems: A review. Addiction. 1993;88(3):315–36.
16. Chick J, Ritson B, Connaughton J, Stewart A. Advice versus extended treatment for alcoholism. Br J Addict. 1988;83:159–70.
17. Drummond D, Thom B, Brown C, Edwards G, Mullan M.
Specialist versus general practitioner treatment of problem
drinkers. Lancet. 1990;336:915–18.
18. Anderson P. Managing alcohol problems in general practice.
BMJ. 1985;290:1873–5.
19. Powell A, Adams P, McCormick R. Preventive medicine in
general practice with particular emphasis on early intervention
for alcohol. N Z Fam Physician. 1996;23:44–7.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Factors influencing diagnostic decision-making
Kathleen SN Callaghan PhD
ABSTRACT
INTRODUCTION: Identifying influences on diagnostic decisions is important because diagnostic errors
often have far-reaching consequences for an individual’s future within the workforce and their eligibility
for Accident Compensation Corporation–funded treatment. Most investigations of factors biasing decision making have used quantitative techniques rather than qualitative methods.
Human Factors Group,
Department of Surgery,
Faculty of Medical and Health
Sciences, The University of
Auckland, New Zealand
AIM: To identify factors influencing GPs’ diagnostic decision-making and to develop a valid questionnaire to determine the desirability and importance of each factor’s influence.
METHODS: Focus groups and the Delphi method were combined with Rasch analysis to identify factors
influencing GPs’ diagnostic decision-making and then examine the strength and stability of ratings of the
factors’ desirability and importance.
RESULTS: Thirty-nine factors were identified. Factors demonstrating high stability but no consensus
included the importance of evidence-based medicine, the potential ramifications of a diagnosis, and the
desirability of medicolegal issues. Factors for which there was disagreement in the first Delphi round but
consensus in the second round included the importance of patient advocacy/support groups and the desirability of examination findings. Rasch analysis indicated that the questionnaire was close to the model
(88.6% and 86.2% of variance in the ratings of importance and desirability explained).
DISCUSSION: Participants readily identified factors influencing GPs’ diagnostic decision-making. Their
ratings did not appear to support a prescriptive model of medicine, yet two cornerstones of prescriptive
medicine, clinical information and probability of disease, were rated as highly desirable and important.
KEYWORDS: Decision-making; diagnosis; bias; Rasch analysis; general practitioners
Introduction
Making an accurate diagnosis and selecting an
appropriate treatment can have profound consequences for an Accident Compensation Corporation (ACC) claimant, determining when or if
they are able to return to work. Most investigations of factors influencing diagnostic or clinical
decision-making employ quantitative methods
rather than qualitative methods. Qualitative techniques can capture a range of factors which may
be overlooked by quantitative methods.1 In one
such qualitative study dermatologists were asked
to identify non-clinical or diagnostic factors and
to indicate how influential the factors were.1
Three types of factors were identified: patientcentred (e.g. patient choice, place of residence,
ethnicity and age), clinician-related factors (e.g.
time constraints, relationship with colleagues
and staff, and pressure from the pharmaceutical
industry), and practice-related factors (e.g. public
or private treatment, cost of treatment to NHS).
United States studies have found regional and
practice variations in diagnostic practices (e.g.
overuse of diagnostic tests) which were related to
the intensity of hospital and physician services.2
Diagnostic practices were less likely to be related
to patient characteristics.
Hajjaj et al.3 argued that understanding how
non-clinical factors affect evidence-based practice
is important in clinical consultation, but usually
overlooked. They argued that a combination of
clinical and non-clinical factors may contribute to
J PRIM HEALTH CARE
2012;4(3):223–230.
CORRESPONDENCE TO:
Kathleen Callaghan
Human Factors Group,
Department of Surgery,
Faculty of Medical and
Health Sciences, The
University of Auckland,
PB 92019 Auckland,
New Zealand
k.callaghan@
auckland.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE223
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
a clinician’s decision without their awareness (e.g.
patient adherence to advice and taking medication may influence the choice of treatment). They
also suggested that a major challenge to practising
medicine is integrating evidenced-based medicine
(EBM) with important non-clinical factors while
maintaining good standards of care. For example,
a United Kingdom report on fitness for work advocated adopting the biopsychosocial approach to
judging an employee’s capacity or fitness for work
rather than focusing on their physical symptoms.4
Others have argued that while the biopsychosocial
model is an inadequate scientific tool, it is nevertheless useful for clinical and teaching purposes5
or the foundation of a philosophy of medicine.6
The current study employed qualitative and
quantitative techniques to examine factors influencing diagnostic decisions. Three methods were
used to identify and evaluate factors affecting diagnostic decisions (especially within an ACC-related context): focus groups, the Delphi method,
and Rasch analysis. Using mixed quantitative and
qualitative methods combines the strengths of
the two while reducing their weaknesses.7 The
general practitioner’s (GP’s) evaluation of a patient’s injury or injuries is critical to the success
of an ACC claim: ‘ACC legislation is a case in
point where diagnosis routinely affects entitlement and cover decisions.’8 A misdiagnosis can
result in temporary or long-term loss of employment, reduced employment opportunities, and
poorer health.9,10 Analyses of ACC claims have
revealed shortcomings in the diagnoses11–13 so a
greater understanding of decision-making is vital.
Given the predominance of the biomedical model
of medicine and the prescriptive and normative
approaches to decision-making,14,15 it was expected
that the factors identified in the current study
would reflect these models and approaches.
Method
224
believe such techniques are necessary to reveal
hidden values and beliefs.18
The Delphi method
The Delphi method was used to identify and
prioritise factors that influence GPs’ decisionmaking. ‘Delphi may be characterised as a
method for structuring a group communication
process so that the process is effective in allowing
a group of individuals, as a whole, to deal with a
complex problem.’19 ‘The Delphi survey is a group
facilitation technique, which is an iterative multistage process, designed to transform opinion into
group consensus.’20 The Delphi method reduces
the influence of more dominant participants and
group pressure.21
Rasch analysis
The Rasch model postulates that ‘…the probability of endorsing a statement is a logistic function
of the difference between two independent quantities: the strength of the respondent’s attitude
and the location of the statement on the attitude
continuum.’22 Rasch analysis yields a measure
on a unidimensional scale of the strength of a
respondent’s attitude, and another measure of
the location on the same scale of the opinion
expressed by an item under study.23 The units
of the scale are log-odds ratio or logits. In this
study, the key respondent attitude is ‘a tendency
to endorse’ the item and the key item measure
is the importance or desirability of a diagnostic
factor. The scale was calibrated such that the
average of the items’ importance or desirability
was arbitrarily set to zero.
The University of Auckland Human Subjects
Ethics Committee informed the investigator that
ethical approval was not required.
Focus groups
Participants
Focus groups are ‘a group of individuals selected
and assembled by researchers to discuss and comment on, from personal experience, the topic that
is the subject of the research.’16 Focus groups may
be biased if one individual dominates the discussion or if the participants are too readily influenced by the facilitator;17 however, some authors
Expert groups responsible for setting GP standards in NZ were identified. There are a number
of groups that influence GP standards; however,
many are biased, either legislatively or otherwise,
towards a particular viewpoint. Academic organisations were identified as being the least biased
‘standard setters’; therefore, participants were
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
selected from five academic organisations which
provide GP training. These were the three Departments of General Practice at the University
of Otago (Dunedin, Christchurch and Otago), the
Departments of General Practice at The University of Auckland, and The Royal New Zealand
College of General Practitioners (RNZCGP).
Heads of department were asked to select a minimum of four participants from senior members of
their department currently in clinical practice. A
reasonable gender balance and a mix of rural/city
practice familiarity was preferred.
The characteristics of the 14 focus group participants were as follows: 10 were male, 4 were female; 13 were in current clinical practice (one had
recently ceased practice to complete a full-time
postgraduate degree); 11 were in urban practice,
and 3 were in rural practice.
Focus group meetings
The investigator met with three of the five
expert groups (time constraints prevented a
meeting with the RNZCGP or the Christchurch
Department of General Practice). Background
information about the study was sent prior to the
meetings. The investigator explained the purpose
of these meetings, but did not participate in the
subsequent discussion. The focus group from
the Dunedin Department of General Practice
comprised six participants while the other groups
comprised four participants.
The lists of factors obtained from each meeting
was examined for overlapping concepts and repetitions, and a composite list embracing the intent
of all the expert groups consulted was compiled.
An electronic questionnaire for Round 1 of the
Delphi process was constructed from the composite list. Copies of the questionnaire together with
instructions and background information were
sent by email to 23 experts who had not participated in the focus groups. The questionnaire contained 39 factors identified by the focus groups
as influencing GP diagnostic decision-making.
The experts were asked to rate the importance
and desirability of each factor using a seven-point
scale, where 1 represented ‘not at all important’
or ‘not at all desirable’ and 7 represented ‘very
WHAT GAP THIS FILLS
What we already know: Clinical and non-clinical factors may bias clinical decision-making. Bias is related to the GP’s perception of the costs and
benefits of making one choice over another.
What this study adds: Thirty-nine factors that potentially bias diagnostic
decision-making by GPs and the subjective value placed on these factors
were identified. Despite responses diverging from the prescriptive model,
standard setters endorsed two cornerstones of the model—clinical information and probability of disease were rated as both highly important and
desirable.
important’, or ‘very desirable’. Experts were free
to comment on each factor.
Despite both email and telephone reminders,
only 12 Round 1 responses were received—a
response rate of 52%. Of the 12 respondents, 6
were male, 6 were female; 11 were in current
clinical practice, 1 had recently ceased practice to
complete a full time postgraduate degree; 5 were
in urban practice, and 3 were in rural practice.
Following standard Delphi methodology, the
experts who responded in Round 1 were asked to
re-rate each influencing factor and provide comments if they wished (Delphi Round 2). Several
areas were clarified based on comments from the
previous round, and one new factor added—a
question designed to explore the influence of
potential ramifications of the diagnosis.
Clarifications and alterations were clearly
identified by a different coloured font. Experts
were provided with their original ratings from
Round 1 together with the group mean rating
for each item. Only 11 Round 2 responses were
received. Given the effort and time required to
elicit completed Round 2 responses, it was assumed that the cost of a further Delphi round
was likely to outweigh any benefits obtained;
hence, a third round was not undertaken.
A Rasch analysis was performed using WINSTEPS® Version 3.55.24 The method adopted was
the rating-scale version of the Rasch model25
where the ratings given to each item are not assumed to be equally spaced, but all items share
the same structure.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE225
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Results
Thirty-nine factors were identified by the focus
groups as influencing GPs’ diagnostic decisionmaking (Tables 1 and 2).
Standard Delphi methodology
The summed mean ratings and stability or consensus of response for the group of GP standard
setters are listed in Tables 1 and 2. Stability of
response is an important, albeit often unreported,
consideration in the analysis of Delphi responses.
Whether or not further Delphi rounds may be
productive can be established by measuring the
stability of respondents’ opinion distribution
curves over successive rounds. The assessment of
stable non-consensual distributions should be of
equal interest in assessing opinion as the assessment of stable consensual distributions.
Group stability of opinion between the two
Delphi rounds was assessed26 and is reported in
Tables 1 and 2. The absolute differences in the
histograms of responses were calculated (subtracted column-wise) for two successive rounds
and then summed to show total units of change.
Net person changes were then calculated by dividing the total units of change by two (any one
participant’s change of opinion is reflected in the
histogram differences by two units of change).
Finally, the percentage change was calculated by
dividing the net person changes by the number of participants. In this method, up to a 15%
change level is accepted as representing a stage of
equilibrium. The higher the percentage change,
the less stable the group’s position.
Responses from the participant who withdrew
between Rounds 1 and 2 were eliminated from
the analysis of stability. Similarly, factors which
were not rated by one of the remaining participants could not be analysed accurately (no factor
had more than one non-response). Stability was
therefore represented as a range, with the lowest
number representing the respondent as having
maintained their previous rating and the highest
number representing a change of rating.
Of interest are factors demonstrating high
group stability without consensus (indicating
fixed disagreement). The importance of EBM,
226
potential ramifications of the diagnosis and the
desirability of medicolegal issues are examples
of these. In most Delphi analyses, consensus is
assumed to have been reached when a specified
percentage of responses falls within a prescribed
range. Neither the proportion nor the range has
been defined in the literature.20 For this study,
consensus was defined as having been reached
when all responses fell within a three-point
range at Round 2. If all responses fell within a
two-point range (or less) then this was defined as
strong consensus. Responses falling outside of a
three-point range constituted disagreement. This
is consistent with other interpretations of agreement and disagreement.27
Some factors showing consensus in Round 2 were
highly unstable indicating that the group had
shifted from a state of disagreement to a state
of agreement between Round 1 and Round 2.
Examples of this are the importance of patient
advocacy/support groups and the desirability of
examination findings as influencing factors.
It is often assumed that each item measured
contributes in a meaningful way to the construct
being investigated; that is, the questionnaire
measures a single dimension. The dimensionality
of the questionnaires used in this study was determined by principal components analysis. The
Rasch measure explained 88.6% of the variance
in ratings of importance (unexplained variance
measured by the next component was 2.8%) and
86.2% of the variance in the ratings of desirability (unexplained variance measured by the
next component was 4%). These results indicate
that the questionnaire was unidimensional and
close to the Rasch model’s intent of measuring
‘one attribute at a time’.23 While the investigator
labelled the constructs ‘importance’ and ‘desirability’, it can be inferred from examination
of the items that the one attribute measured is
represented by the label.
The assumption that ratings are equally spaced
was tested using Masters and Wright’s method28
in which cumulative answers give the probability
of responding greater or equal to each one of the
available categories (e.g. ≥1, ≥2 etc). The threshold value is set where the cumulative probabilities equal 0.5. For example, in Table 3 the logit
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Table 1. Summed mean ratings of importance, stability, degree of stability, consensus and strength of consensus
Mean rating
(importance)
Stability
Degree of
stability
Consensus
Strength of
consensus
History
6.8
Yes
9.1
Yes
†
Examination findings
6.2
Yes
9.1
Yes
*
GP’s personal clinical experience
5.5
Yes
9.1
Yes
*
GP’s knowledge of local conditions
5.4
18.2
Yes
†
Yes
*
Influencing factor
Results of investigations
5.3
Possibly yes
13.6–18.2
Evidence-based medicine
5.2
Yes
9.1
Characteristics of the GP
4.8
22.7
Need to achieve an outcome
4.4
31.8–36.4
Patient expectations
4.2
36.4
Patient advocacy
4.0
22.7–27.3
Medicolegal issues
4.0
36.4
Characteristics of the patient
4.0
27.3
Reasonable patient pressure
4.0
Closeness of GP/patient relationship
4.0
Time available for the consultation
4.0
External feedback from a medical source
3.9
Potential ramifications of the diagnosis
3.9
The clinical setting
3.6
27.3
Need to justify a course of action
3.6
18.2
Personal circumstances of the patient
3.5
36.4
Expectations of external medical professionals
3.5
22.7
The Health and Disability Commissioner
3.1
18.2
Potential implications for the wider community
3.1
50–54.5
Context in which the diagnosis is made
3.1
18.2
Administrative requirements
3.0
27.3
Unreasonable patient pressure
3.0
36.4
27.3
Possibly yes
13.6–18.2
18.2
18.2
Yes
0.0
GP’s desire to please the patient
3.0
27.3
Diagnostic algorithms/categories/protocols
3.0
18.2
Fear of uncertainty
2.9
36.4
Whether or not treatment is available for the
diagnosed condition
2.9
27.3
GP’s perception of what other external health
professionals may think
2.8
36.4
GP’s perception of the state of the national
health care system
2.6
27.3
Marketing/media
2.6
18.2
Legal requirements
2.6
27.3
Patient advocacy/support groups
2.5
36.4
Technological tools
2.3
27.3
Who is funding the consultation
1.7
Business considerations
1.6
External incentives
1.1
Yes
Yes
9.1
Yes
*
18.2
Yes
†
9.1
Yes
†
*Consensus
† Strong consensus
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE227
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Table 2. Summed mean ratings of desirability, stability, degree of stability, consensus and strength of consensus.
Mean rating
(desirability)
Stability
History
6.6
Yes
Examination findings
6.2
Evidence-based medicine
6.2
GP’s knowledge of local conditions
5.7
Results of investigations
5.5
Influencing factor
Degree of
stability
Consensus
Strength of
consensus
0.0
Yes
†
27.3
Yes
*
Yes
9.1
Yes
*
Yes
9.1
Yes
*
Yes
*
Yes
*
18.2
GP’s personal clinical experience
5.2
27.3
External feedback from a medical source
4.3
36.4
Technological tools
3.8
31.8–36.4
Potential implications for the wider community
3.6
Patient advocacy
3.6
Characteristics of the GP
3.5
Characteristics of the patient
3.5
45.5
Patient expectations
3.4
18.2
Need to achieve an outcome
3.3
22.7–27.3
27.3
Possibly yes
13.6–18.2
18.2
Closeness of GP/patient relationship
3.1
Medicolegal issues
2.8
Expectations of external medical professionals
2.8
Diagnostic algorithms/categories/protocols
2.8
27.3
Legal requirements
2.6
45.5
Need to justify a course of action
2.4
31.8–36.4
40.9–45.5
Yes
9.1
36.4
Reasonable patient pressure
2.4
36.4
Personal circumstances of the patient
2.3
22.7–27.3
The Health and Disability Commissioner
2.3
27.3
Potential ramifications of the diagnosis
2.3
18.2
GP’s perception of what other external health
professionals may think
2.1
18.2
Administrative requirements
1.9
18.2
The clinical setting
1.9
18.2
Time available for the consultation
1.9
18.2
Patient advocacy/support groups
1.9
Marketing/media
1.6
GP’s desire to please the patient
36.4–40.9
Yes
*
13.6–18.2
Yes
†
1.6
36.4
Yes
*
Fear of uncertainty
1.6
22.7–27.3
Yes
†
Whether or not treatment is available for the
diagnosed condition
1.6
13.6–18.2
Yes
*
Possibly yes
Possibly yes
Unreasonable patient pressure
1.4
18.2
Yes
†
Who is funding the consultation
1.3
18.2
Yes
†
Context in which the diagnosis is made
1.3
4.5–9.1
Yes
*
GP’s perception of the state of the national
health care system
1.2
27.3
Yes
†
Business considerations
1.2
Yes
9.1
Yes
†
External incentives
1.0
Yes
9.1
Yes
†
Yes
*Consensus
† Strong consensus
228
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Table 3. Fifty percent cumulative probabilities for ratings of importance and desirability
Likert category (desirability)
1
2
3
4
5
6
7
50% cumulative probability (logits)
…
-1.97
-0.96
-0.27
0.38
1.02
1.81
Likert category (importance)
1
2
3
4
5
6
7
-2.77
-1.70
-1.00
0.15
1.62
3.70
50% cumulative probability (logits)
value of -2.77 is the threshold at which a Likert
rating of 1 is equally probable as a rating of 2 or
above. The logit value of 3.70 is the threshold at
which a rating of below 6 is as equally probable
as a rating of 7. The thresholds are not spread
equidistantly and it is easier to move between categories when rating desirability than when rating
the importance of influencing factors.
When the distribution of participants and factors was plotted, the most important influencing factor was history, followed by examination
findings, and the GP’s personal clinical experience. However, the difference between history
and examination findings is 2.22 logits versus
1.43 logits between examination findings and
GP’s knowledge of local conditions; hence, history would appear to be a much more important
influencing factor than would be expected from
knowledge of its ordinal position alone. Similarly,
external incentives are regarded as being much
less important than business considerations, with
a distance of 1.89 logits separating these factors.
While history is viewed as the most desirable
influencing factor, it is not as desirable as it is
important, according to the difference in ratings
(-5.95 logits for importance versus 3.56 logits
for desirability). This indicates that the experts
preferred to de-emphasise history as an influencing factor while maintaining its ordinal position.
EBM was the sixth most important influencing
factor but the second most desirable factor, despite representing only a difference of 0.91 logits.
At the other end of the importance and desirability ordinal scale, factors such as external incentives, business considerations, and who is funding
the consultation show very little logit mismatch.
Both the importance and desirability questionnaires are marked by a very broad span of 10.3 and
7.97 logits respectively, indicating a quite marked
‘black and white’ view of the factors at either
extreme. The item reliability index was used to
test the replicability of item placements (influencing factors) assuming these same factors were to be
given to another group of comparable standard setters. For ratings of importance the item reliability
index was 0.94 (an estimated 94% of the observed
variance in the results obtained can be regarded as
true variance, with the remaining 6% attributable
to measurement error). In other words, the results
obtained could be expected to correlate 0.94 with
the results from a parallel measure of the same
underlying construct. For ratings of desirability,
the item reliability index was 0.93.
ACC-specific ramifications were considered less
important than generic ramifications (0.01 versus
0.18 logits). The ramifications of a diagnosis
(whether generic or ACC-specific) were not considered to be a desirable influence on diagnostic
decision-making (0.34 and 0.39 logits).
Discussion
The relatively low number of participants in this
study and the low response rate of 52% raises
some concerns over the reliability29,30 of the results obtained; however, the item reliability index
values ameliorate these concerns.
The current study used a qualitative approach to
identify factors influencing GPs’ decision-making
together with quantitative techniques. The stability of responses was also assessed. An advantage
of Rasch scaling is that it enables meaningful
comparisons between different groups undertaking the same questionnaire.
It is noteworthy that the standard setters readily
identified 39 factors that influence GPs’ diagnostic
decision-making. The factors identified are not unexpected because they reflect everyday influences
such as what others think of us, what we think
of others, legality, need to achieve an outcome
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE229
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
and so forth. That these factors can be identified
supports the controversial notion that it is not
possible to divorce the practice of medicine from
the society in which it is practised.31 Interestingly,
while a prescriptive view of diagnostic decisionmaking (in which decision-making is improved
through the use of clinical guidelines etc.32) appears invalidated by the responses obtained in this
study, the factors on which a prescriptive view of
medicine relies (clinical information and probability of disease) are rated as both highly important
and highly desirable. This apparent dissonance
might be explained by Elstein:33 ‘All models and
theories are simplifications of reality. Models are
not reality however, and theory is not practice.’
Further research is required to determine the
prevalence and consequences of diagnostic errors
and to obtain further insight from an in-depth
‘systems’ approach (including nature of the error
and underlying causal/contributory factors). A
diagnosis relating to an ACC claim can be critical
to whether a patient returns to work. Remaining
in or returning to work is recognised as providing
a significant contribution to health and well­
being.34–36 A better understanding of diagnostic
decision-making within an ACC-related context,
therefore, has important financial and social
consequences not only for the patient but also for
their community.
References
ACKNOWLEDGEMENTS
We thank John Irwin
and Pat Bullen for their
invaluable comments
on this manuscript.
FUNDING
The source of funding for
the study was a University
of Auckland Senior Health
Research Scholarship.
COMPETING INTERESTS
None declared.
230
1. Hajjaj F, Salek M, Basra M, Finlay A. Nonclinical influences,
beyond diagnosis and severity, on clinical decision making in
dermatology: understanding the gap between guidelines and
practice. Br J Dermatol. 2010;163(4):789–99.
2. Song Y, Skinner J, Bynum J, Sutherland J, Wennberg JE, Fisher
ES. Regional variations in diagnostic practices. N Engl J Med.
2010;363(1):45–53.
3. Hajjaj F, Salek M, Basra M, Finlay A. Non-clinical influences on
clinical decision-making: a major challenge to evidence-based
practice. J R Soc Med. 2010;103(5):178–87.
4. Bevan S, Passmore E, Mahdon M. Fit for work? Musculoskeletal disorders and labour market participation. London; 2007.
5. Kendler KS. The rise and fall of the biopsychosocial model:
reconciling art and science in psychiatry. Am J Psychiatry.
2010;167(8):999–1000.
6. Lewis B. The biopsychosocial model and philosophic pragmatism: is George Engel a pragmatist? Philos Psychiatr Psychol.
2008;14(4):299–310.
7. Johnson R, Onwuegbuzie A. Mixed methods research:
a research paradigm whose time has come. Educ Res.
2004;33(7):14–26.
8. Callaghan KSN. Factors that influence general practitioner
diagnostic decision-making and a comparison with other
stakeholders. University of Auckland; 2006.
9. The Royal Australasian College of Physicians. Compensable
injuries and health outcomes. Sydney: The Royal Australasian
College of Physicians; 2001.
10. The Royal Australasian College of Physicians AFOEM. Helping
people return to work: using evidence for better outcomes.
Sydney; 2010.
11. Gorman DF. Audit of the ACC Workwise Clinic—December
1997. Auckland: The University of Auckland; 1997.
12. Gorman DF. Audit of the ACC Workwise Clinic—September
1997. Auckland: The University of Auckland; 1997.
13. Gorman DF, Jarvie P, Robinson P. Occupational health practice
in New Zealand. NZ Med J. 1999;112:79–82.
14. Shaban RZ. Theories of clinical judgment and decisionmaking: a review of the theoretical literature. J Emerg Primary
Health Care. 2005;3(1–2).
15. Wilson HJ. The myth of objectivity: is medicine moving
towards a social constructivist medical paradigm? Fam Pract.
2000;17(2):203–09.
16. Powell RA, Single HM. Focus groups. Int J Qual Health Care.
1996;8(5):499–504.
17. Cox SJ, Cheyne AJT. Assessing safety culture in offshore
environments. Saf Sci. 2000;34(1–3):111–29.
18. DeJoy DM. Behavior change versus culture change: divergent approaches to managing workplace safety. Saf Sci.
2005;43(2):105–29.
19. Linstone H, Turoff M. Introduction. In: Linstone H, Turoff M,
editors. The Delphi method. Techniques and applications.
Massachusetts: Addison-Wesley Publishing Company; 1975.
20.Hasson F, Keeney S, McKenna H. Research guidelines for the
Delphi survey technique. J Adv Nurs. 2000;32(4):1008–15.
21. Normand S-LT, McNeil BJ, Peterson LE, Palmer RH. Eliciting
expert opinion using the Delphi technique: identifying performance indicators for cardiovascular disease. Int J Qual Health
Care. 1998;10(3):247–60.
22. Irwin RJ, Irwin KC. Attitude towards mathematics of 11-yearolds: analysis of a questionnaire and its relation to mathematical
achievement. In: Waugh RF, editor. Frontiers in educational
psychology. New York: Nova Science Publishers; 2004:107–16.
23.Bond TG, Fox CM. Applying the Rasch model: fundamental
measurement in the human sciences. Mahwah, New Jersey:
Lawrence Erlbaum Assoicates; 2007.
24. WINSTEPS: Multiple-choice, rating scale, and partial credit
Rashch analysis [program]. Chicago: MESA Press; 2000.
25.Andrich D. A rating formulation for ordered response categories. Psychometrika. 1978;43:561–74.
26.Scheibe M, Skutsch M, Schofer J. Experiments in Delphi
methodology. In: Linstone H, Turoff M, editors. The Delphi
method. Techniques and applications. Reading, Massachusetts: Addison-Wesley Publishing Company; 1975:263–83.
27. Brook RH, Chassin MR, Fink A, Solomon DH, Kosecoff J, Park
RE. A method for the detailed assessment of the appropriateness of medical technologies. Int J Tech Assessment Health
Care. 1986;2 (Part 1):53–63.
28.Masters GN, Wright BD. The partial credit model. In: van der
Linden WJ, Hambleton RK, editors. Handbook of modern
item-response theory. New York: Springer; 1997:101–21.
29. Frisbie DA. Reliability of scores from teacher-made tests. Educ
Meas: Issues and pract. 1988;7(1):25–35.
30.Traub RE, Rowley GL. Understanding reliability. Educ Meas:
Issues and pract. 1991;10(1):37–45.
31. Gorman DF, Scott J. The social distortion of medical practice.
Med Today. 2003;4(11):75–77.
32. Shaban RZ. Theories of clinical judgment and decisionmaking: a review of the theoretical literature. J Emerg Primary
Health Care. 2005;3(1–2):23–33.
33. Elstein AS. Clinical problem solving and decision psychology:
comment on ‘The epistemology of clinical reasoning’. Acad
Med. 2000;75(10):S134–S36.
34.Bevan S, Quadrello T, McGee R, Mahdon M, Vavrovsky A,
Barham L. Fit for work? Musculoskeletal disorders in the
European workforce. London; 2009.
35. Black DC. Working for a healthier tomorrow. Norwich; 2008.
36.The Royal Australasian College of Physicians AFOEM. Realising the health benefits of work. Sydney; 2010.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Maori cultural adaptation of a brief mental
health intervention in primary care
Fiona Mathieson MA (applied) Clinical and Community Psychology, Dip Tchg;1 Kara Mihaere PGdip Clinical
Psychology, PhD;2 Sunny Collings MBChB, PhD;3 Anthony Dowell MBChB;4 James Stanley PhD4
Department of Psychological
Medicine, University of Otago
Wellington, New Zealand
1
ABSTRACT
INTRODUCTION: There are no brief psychological mental health interventions designed specifically for
Maori in a primary care setting.
AIM: To adapt an existing cognitive behavioural therapy–based, guided self-management intervention
for near-threshold mental health syndromes in primary care, for Maori, and to examine its acceptability
and effectiveness.
METHODS: Semi-structured interviews with primary care clinicians and Maori patients were conducted
to inform adaptations to the intervention. Clinicians were then trained in intervention delivery. Patients
were recruited if they self-identified as Maori, were aged 18–65 years, were experiencing stress or
distress and scored ≤35 on the Kessler-10 (K10) measure of global psychological distress. Patient and
clinician satisfaction was measured through a questionnaire and semi-structured interviews. Post-intervention, patients’ mental health status was measured at two weeks, six weeks and three months.
Te Whare Marie, Specialist
Maori Mental Health Service,
Capital Coast DHB, Wellington
2
Director of Social Psychiatry
and Population Mental Health
Research Unit, University of
Otago Wellington
3
Primary Health Care and
General Practice, University
of Otago Wellington
4
RESULTS: Maori adaptations included increased emphasis on forming a relationship; spirituality;
increased use of Maori language and changes to imagery in the self-management booklets. Nine of the
16 patients recruited into the study completed the intervention. Patients and clinicians rated the intervention favourably and provided positive feedback. Improvement was seen in patients’ K10 scores using
intention-to-treat rated global psychological distress following intervention.
DISCUSSION: This study found that it was not difficult to adapt an existing approach and resources, and
they were well received by both providers and Maori patients. Further research is required with a larger
sample utilising a randomised controlled trial, to establish whether this approach is effective.
KEYWORDS: Primary health care; Maori mental health; patient satisfaction; brief intervention
Introduction
Disseminating evidence-based mental health
treatments into real-world settings poses a number
of challenges for clinicians and policy makers. The
field of cross-cultural mental health is a fledgling
one.1 This is certainly the case in New Zealand,
with little research on talking therapies for Maori,2
none of which are in primary care mental health.
There are disparities between Maori and nonMaori regarding access to mental health services
and, when contact occurs, it is often with primary care services.3 Near-threshold mental health
symptom complexes such as anxiety, depression, harmful use of recreational or prescribed
substances, or a combination of these (not at a
diagnostic level), are common (15.3%) in Maori.3
‘Near-threshold’ anxiety, depression and substance use are common presentations in primary
care and often coexist. While not meeting the
threshold for disorder in standard diagnostic systems such as DSM-IV,4 these symptom complexes
carry a significant disability burden along with
the risk of developing a diagnosable disorder.5,6
These symptom complexes often arise in the
context of social problems and cause distress and
J PRIM HEALTH CARE
2012;4(3):231–238.
CORRESPONDENCE TO:
Fiona Mathieson
Department of
Psychological Medicine,
University of Otago
Wellington, PO Box 7343,
Wellington 6242,
New Zealand
fiona.mathieson@
otago.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE231
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
significantly impaired work and role functioning.7 GPs perceive and manage them as clinically
significant.8,9 There is evidence that mental health
services are negatively perceived by Maori,10,11
and it has been recommended that mental health
services for them should be more closely aligned
with primary health care, with services geared to
their cultural expectations, if they wish. Increasing primary care clinician skills in assessment and
management of Maori mental health will maximise early intervention and minimise referral out.12
primary care setting. The sessions comprise one
hour in total and are supported by a treatment
manual and self-help booklets on the topics of
relationships, stress and breaking habits. The clinician role is that of coach and change facilitator
rather than ‘therapist’. Patients work to develop a
specific plan for change, which is printed out as
a prescription. Prescriptions are integrated with
the computerised patient management system for
ease of access. There is one follow-up phone call/
email to ask how this plan is working.
The literature on talking therapy adaptation
for Maori is scant.2 One study adapted cognitive behaviour therapy for Maori based on input
from a range of Maori advisors, with promising
outcomes.13 However, there are no studies in this
area in primary care.
Clinicians were trained in a two-hour training session. Clinician and patient satisfaction ratings were
very positive and patient outcome scores indicated
that this approach may be beneficial, although the
sample was small in the acceptability study.19
Expert opinion on cultural adaptation suggests
that the following aspects of Maori culture
need to be incorporated into therapy in order to be effective for Maori: an emphasis on
whakawhanaungatanga (the process of forming
relationships); an emphasis on the whanau (family) and iwi (tribe);14 use of te reo (Maori language); an emphasis on spirituality and fostering
of strong cultural identity.15,16
At the same time, it is important to maintain
awareness of cultural diversity among Maori and
generalisations regarding cultural or therapeutic
mores should be avoided.15,16 While it is important to be aware of common Maori worldviews
and how they can be accommodated in practice, it
is equally important to be guided by the individual tangata whaiora (person seeking wellness)
and their whanau (extended family). International
indigenous literature reflects similar concepts and
values to those that have been identified in the
New Zealand literature.2
An innovative, ultra-brief intervention (UBI) was
designed for people aged 18–65 with near-threshold mental health syndromes. The approach was
developed through a collaborative process involving patients, clinicians and researchers.19 UBI consists of three brief sessions of guided, cognitive
behaviour therapy–based18 self-management, with
a focus on problem solving and behaviour change,
delivered by the primary care clinician in the
232
This paper reports on the process and outcomes of
a feasibility study into adapting the UBI approach
to better fit the needs of Maori patients. The aim
was to develop a credible and acceptable UBI for
subthreshold mental health syndromes among
Maori, to be delivered in primary care settings by
non-specialist clinicians. The questions were:
1. To what extent and in what way does UBI
need to be adapted for Maori?
2. How acceptable is the adapted intervention to
clinicians and Maori patients?
Methods
Adaptation process
The adaptation process comprised a review of the
literature, along with both individual face-to-face
and group interviews with primary care clinicians and individual face-to-face interviews with
Maori potential users of the intervention. The
rationale for this approach was that a collaborative approach to therapy adaptation was more
likely to result in an approach that was feasible and acceptable in this context. Early in the
research process, a partnership was formed with
a Maori health researcher (KM, co-investigator),
who worked clinically in a primary care setting.
She established relationships with local providers,
conducted the interviews with patients and clinicians, and had face-to-face contact with patients
to collect intake and outcome data.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Interviews
WHAT GAP THIS FILLS
Semi-structured interviews were conducted with
nine general practitioners (GPs) and nine primary
care nurses. Of these, four identified as Maori
(one GP, three nurses), six as New Zealand European and eight as ‘other’ ethnicity. Clinicians
were based in urban group practice primary care
settings, none of which were specifically focused
on Maori health needs, but all of which had some
Maori patients attending their practices.
What we already know: Near-threshold mental health syndromes are
common among Maori. Little is known about brief interventions in primary
care for these syndromes and, similarly, the literature on adapting talking
therapies for Maori is scant.
Clinicians were shown the existing UBI booklets
and the existing clinical approach was outlined to
them. They were asked to respond to the existing
UBI approach and to suggest how it would need
to be adapted to better meet the needs of Maori
patients.
Clinicians reported that the existing approach
and structure appealed. They felt the same basic
format could be retained, but they thought it had
a ‘middle-class European flavour’. They suggested that we have more and different imagery
and more Maori language, easier language, fewer
words, more relevant scenarios in the vignettes,
a karakia (prayer) and a whakawhanaungatanga
process (forming connections). Clinicians were
keen to get continuing education credits for the
training and preferred to have the training during regular peer meetings.
Semi-structured, individual face-to-face interviews were also conducted with six potential
patient users of the intervention, who all identified as Maori. Recruitment was through an article
in the local community newspaper. Feedback
from the potential patients was similar to that
of the clinicians. There was a range of responses
to the idea of offering karakia, with some more
comfortable with the idea than others.
What this study adds: This paper describes the process and outcomes
of an adaptation of an innovative, ultra-brief intervention, creating a version
with promising clinical effectiveness and acceptability for Maori.
option of offering a karakia in English or Maori,
if they were comfortable.
A whakawhanaungatanga process was added at the
start of the first session. In this process, clinicians
were encouraged to self-disclose a little bit about
themselves, such as family background or work
history, and ask their patient about these areas.
The imagery in the self-help booklets was
changed by increasing the number of images and
using more Maori designs. A Maori graphic designer was employed to make these changes. The
covers of the booklets and treatment manual and
some of the imagery contained in the booklets
are shown in Figure 1.
The scenarios in the vignettes were changed
to be more culturally relevant, such as playing
Figure 1. The covers of the self-help booklets and treatment manual and some of the
imagery contained in the booklets
Adaptations made
In response to the feedback, the following adaptations were made to UBI: Patients were invited to
begin sessions with an optional karakia or whakatauki (proverb). Whakatauki were provided, such
as ‘He manga wai koia kia kore e whikitia; It is a
big river indeed that cannot be crossed’. Alternatively, clinicians and patients were given the
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE233
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Figure 2. Recruitment of patient participants and data collection process
Consenting patients
make appointment for
first session and make
a problem list
Patient presents
to GP
Routine clinical
assessment CHAT/
clinical judgment
Distress?
Research assistant
contacts patient and
conducts baseline
assessment
Invite patient
to participate
touch rugby, rather than soccer. The sessions
were changed to include a stronger emphasis on
how whanau (extended family) could be involved
in supporting the person, and patients were also
asked about whether wairua (spirituality) was an
important part of their wellbeing and, if so, how
they nourished it.
There was a slight increase in the use of Maori
language in the booklets, largely through the use
of whakatauki, and terms such as ‘wairua’ and
‘whanau’. Both patient and clinician feedback
had suggested that full translation would not be
helpful.
Session 1
Clinician training
Session 2
Identify as Maori;
English speaking and
aged 18–65?
Session 3 +
follow-up phone call
And not suicidal
Administer K10
K10 scores of
35 or less?
Post-intervention K10
assessment of patients
at 2 weeks
YES
Patient satisfaction
questionnaire
administered 6 weeks
NO
K10 scores of more
than 35
Clinician satisfaction
questionnaire
administered
The clinician training session was two hours long
and included a presentation and role-play practice.
In addition, the adaptations made for Maori were
outlined and a video role-play of a clinician working with a Maori patient was added. This demonstrated skills such as offering the whakatauki and
whakawhanaungatanga process.
Recruitment
As shown in Figure 2, patient eligibility was
determined by clinician assessment of the presence of psychological distress. This was assessed
by clinical judgment and/or the Case-finding and
Help Assessment Tool (CHAT) for lifestyle and
mental health assessment of adult patients in primary care.20 After applying the exclusion criteria
(non-English speaking, under age 18 or over age
65, no suicidal ideation in the past two weeks),
the remaining patients were screened by the clinician for the presence of psychological distress
using the Kessler-10 (K10) measure of global
psychological distress (a standard 10-item selfreport questionnaire based on questions about the
level of anxiety and depressive symptoms in the
preceding four-week period). Higher scores on the
K10 indicate greater distress.21
Patient ineligible
Offer medication or
specialist referral
234
A score of 35 or less on the K10 determined final
eligibility. Patients with K10 scores over 35 received their GP’s usual care as appropriate—generally medication or referral to a mental health
professional. Patients meeting criteria for inclusion were invited to participate in the study. The
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
right-hand column of boxes in Figure 2 shows the
study data collection process before, during, and
after the UBI-Maori (UBI-M) sessions.
Clinician and patient satisfaction
Clinician and patient satisfaction questionnaires
were administered following completion of the
intervention (patient questionnaires at two weeks
post-intervention and clinician surveys at the end
of the study). Possible responses to each statement were based on a five-point Likert scale to
indicate levels of agreement or disagreement.
The statements were designed by the investigators and informed by feedback obtained from
clinician and patient interviews conducted during
the design phase of the intervention. Patient K10
scores were reassessed at two weeks, six weeks
and three months post-intervention. Patients and
clinicians were also asked a semi-structured series
of questions about what they liked and did not
like about the intervention and any changes they
would like to see.
Data collation and analysis
All semi-structured interviews were audio
recorded and transcribed verbatim. The transcript
data was collated thematically under the headings
of each question by the data gatherer (KM).
Questionnaire data were entered into Microsoft Access. Data analysis was performed using
R 2.11. The 95% confidence intervals reported
were based on the t-distribution. Formal comparisons between K10 scores at intake with K10
scores post-intervention used paired-sample
t-tests across participants. As only some participants who completed the intervention completed
all three follow-up outcome measures (n=7), the
descriptive statistics and hypothesis testing for
the K10 data were calculated on an intentionto-treat basis—that is, missing data points were
replaced with the most recent K10 score available for that participant. This produces a slightly
more conservative estimate of the magnitude
of improvement compared to excluding these
individuals from analysis. Descriptive statistics
(range, inter-quartile range, and median) were
calculated for the Likert-response items on the
patient satisfaction scales.
The feasibility study was approved by the Central
Regional Ethics Committee. (CEN/09/11/085).
Approval was also gained from the Ngai Tahu
Research Consultation Committee which is a partnership between Te Runanga o Ngai Tahu and the
University of Otago.
Findings
Sample
Sixteen patients were recruited into the study.
The majority of these patients were female (13/16,
81%) and the median age was 38.9 years, with a
range from 20 to 65 years. They came from a low
socioeconomic, urban group, with 56% not in paid
employment and 71% having an annual household
income of less than $20,000.
Five people did not complete the study for work or
personal reasons, and two did not complete due to
clinical reasons (including one patient referred to
secondary mental health services). This left nine
patient participants who completed the intervention. Seven of these completed all the follow-up
measures.
Of the 22 clinicians trained in the intervention,
five clinicians used the intervention, each seeing
between one and seven patients.
Levels of patient satisfaction
The results of the patient satisfaction questionnaire at two weeks post-intervention are presented
in Figure 3.
Patients who completed all three UBI-M sessions
reported high levels of satisfaction with most
aspects of the intervention. Some would have preferred more sessions and/or longer sessions. Some
did not find the self-help booklets particularly relevant. Patient comments from the semi-structured
interview are shown in Figure 4.
Levels of clinician satisfaction
The clinician satisfaction questionnaire ratings are
not shown graphically due to the small number of
clinicians who delivered the complete intervention (n=4). The interview data was thematically
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE235
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
Figure 3. Boxplots (median, interquartile range, range) showing patient satisfaction ratings (n=9)
collated under the headings of each question by
the data gatherer (KM). Interview data and ratings
indicated a high degree of clinician satisfaction
with many aspects of UBI-M. These included the
intervention, timing between sessions, the logical
structure, the manual was easy to use, the prescriptive approach was acceptable, and it seemed to
meet patients’ needs. Clinicians reported that they
largely kept to the framework and it was different from their usual practice. They were happy to
use the approach again and would recommend it
to colleagues. However, some felt that the length
of sessions was inadequate. Some suggestions
were made for improvements, such as a booster
training session soon after the initial training and
assistance with pronunciation of Maori words.
Clinician comments are shown in Figure 5.
Figure 4. Patient satisfaction comments
‘It felt as though he was helping me that step further’
‘It helped me as a person to have faith in myself again that I can actually pull
through these tough times’
Mental health status of
patients at follow-up
Changes in the mental health status of the
patient participants are illustrated in Figure 6, as
measured by mean K10 scores and 95% confidence intervals (n=16 intention-to-treat analysis)
at intake and post-intervention (at two weeks, six
weeks and three months). Results in the lefthand part of the figure are from the original UBI
study,19 which had a larger sample size (n=18).
The results in the right-hand side of the figure
are from the UBI-M study. For both studies, analysis was based on an intention-to-treat analysis.
Improvements in score from the intake period
were calculated for the UBI-M study. Mean
improvement at Week 2 was 5.2 points (95% CI
1.5–8.8; one-sample t-test t(15)=2.99, p=0.009).
Mean improvement at Week 6 was similar at
5.1 points (95% CI is 0.9–9.3; one-sample t-test
t(15)=2.60, p=0.020). By month 3 post-treatment,
the mean improvement from intake was no longer
statistically significant at 4.2 points (95% CI
-0.5–8.96; one-sample t-test t(15)=1.90, p=0.077).
‘It gave me the power back’
‘I just felt safe in that environment’
Discussion
‘He was lifting me out of my hole but not mollycoddling me. I was doing it but he
was there too’
A particular strength of this study is the demonstration that a culturally appropriate collaborative
approach to intervention adaptation can result in
236
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
a talking therapy which has both clinical promise
and high credibility and acceptability to patients
and clinicians.
Improvement was seen in patients’ rated global
psychological distress following intervention.
While the improvement was not statistically
significant, the confidence intervals indicate that
it is highly likely that the true mean improvement will be greater than zero (i.e. an actual
improvement). However, this study is limited by
the absence of a control group; hence, it remains
unclear whether this is any greater improvement
than might have occurred with no intervention.
Other limitations include the relatively short
follow-up (three months) and the small sample.
There was relatively low uptake by clinicians.
Reasons given for not using the intervention
included not finding suitable patients (some
practices had a low percentage of Maori patients),
finding change difficult and being busy with
competing demands.22
Unlike secondary care, primary care has a broad
scope and patients may not present there with
mental health issues as the main problem. The
Figure 5. Clinician satisfaction comments
‘Good to have another tool’
‘Familiar face, familiar environment were helpful’
‘It normalises it. That fear is not so much there’
‘I needed help with pronunciation’
‘Like the getting to know process’
‘Different from my usual practice. I do not usually self-disclose any personal information’
‘The karakia put people at ease; patients seemed surprised but appreciative at
being offered it’
‘Had to chase people for sessions 2 and 3 (text reminders helped)’
‘An extra training session would help, to help people get started’
‘Bang on, really’
‘It empowered clients to go away and do their own mahi (work) and then come
back’
‘I liked how the client made their own realisations’
‘I liked having a framework so you don’t fall apart in the middle of it’
‘Nobody in her life had ever paid her that kind of attention… it was quite humbling’
Figure 6. Mean K10 scores (95% confidence intervals) for UBI and UBI-Maori adaptation at intake, two weeks, six weeks and three months.
Analysis includes intention-to-treat carry-over of initial K10 scores for non-completers.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE237
ORIGINAL SCIENTIFIC PAPERS
MIXED METHOD RESEARCH
competing demands on clinicians in terms of
time and multiple presenting problems make it
challenging for clinicians to incorporate mental
health interventions into routine clinical practice,
particularly if a suitable patient is not identified
soon after UBI training occurs. This uptake issue
could be addressed by providing top-up training approximately three weeks after the initial
training occurs. Confidence with pronouncing
Maori words could be assisted by the provision
of a CD recording, practising common words and
whakatauki. The training could be incorporated
into ongoing peer review processes.
The total amount of contact time for this intervention is one hour and although this is brief in
terms of traditional therapy approaches, for many
clinicians in the primary care context this is a
long time. However, it can be argued that this is
a relatively small amount of time compared to an
area like diabetes care, which is long term and
time consuming due to the emphasis on teaching
self-management. Clinicians may nevertheless
need both protected time and resources for this
approach to be sustainable.
ACKNOWLEDGEMENTS
Thanks to Hori Mataki
from Ariki Creative for the
design work and Professor
Felicity Goodyear-Smith,
Associate Professor
Simon Hatcher and
Dr Simon Bennett for
their contribution to the
original UBI design.
FUNDING
Oakley Mental Health
Research Foundation
and University of Otago
Research Grants.
COMPETING INTERESTS
None declared.
238
Our experience suggests that there is potential
for clinical improvement to occur through brief
talking interventions in primary care with
both Maori and non-Maori versions of UBI.
It seems likely that there are similar change
processes that operate across cultural groups, at
least for this near-threshold group of patients.
The strong tradition of Maori oratory in healing aligns well with the overall principles of
the brief intervention and particularly with
the Maori adaptation.
Despite the limitations, the findings of this
study suggest that cultural adaptation of an
intervention was feasible and was well received
by both patients and clinicians. All but one of
the research team in the study were non-Maori,
and concerned about ‘getting it right’ culturally.
The experience of this adaptation was rewarding
for the research team and offers a model for other
areas of clinical practice.
Further research is required by way of a randomised controlled trial to establish whether this
approach is effective.
References
1. Hayes PA, Iwamasa GY, editors. Culturally responsive cognitive behavioral therapy: assessment, practice and supervision.
American Psychological Association, Washington DC; 2006.
2. Te Pou. He rongoa kei te korero. Talking therapies for Maori:
Wise practice guide for mental health and addiction services.
Auckland: Te Pou o Te whakaaro Nui; 2010.
3. Oakley Browne MA, Wells JE, Scott KM, editors. Te Rau
Hinengaro: the New Zealand Mental Health Survey. Wellington: Ministry of Health; 2006.
4. American Psychiatric Association: Diagnostic and Statistical
Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
5. Judd L, Schettler P, Akiskal H. The prevalence, clinical relevance and public health significance of subthreshold depressions. Psychiatr Clin North Am. 2002;25:685–698.
6. Kessler R, Zhao S, Blazer D, Swartz M. Prevalence, correlates,
and course of minor depression in the national comorbidity
survey. J Affect Disord. 1997;45(1–2):19–30.
7. Collings S and The MaGPIe Research Group. Disability and the
detection of mental disorder in primary care. Soc Psychiatry
Psychiatr Epidemiol. 2005;40(12),994–1002.
8. Dowell A, Garrett S, Collings S, et al. Primary Mental Health
Initiatives: Interim Report. Wellington: School of Medicine and
Health Sciences, University of Otago, Wellington; 2007:242.
9. Backenstrass M, Joest K, Rosemann T, et al. The care of
patients with subthreshold depression in primary care: is it all
that bad? A qualitative study on the views of general practitioners and patients. BMC Health Serv Res. 2007;7(1):190.
10. Durie M. Whaiora: Maori Health Development. Auckland:
Oxford University Press; 1994.
11. Jansen P, Bacal K, Crengle S. He Ritenga Whakaaro: Maori Experiences of health services. Auckland: Mauri Ora Associates;
2008.
12. Durie M. Mental health and Maori development. Aust N Z J
Psychiatry. 1999;33(1):5–12.
13. Bennett S. Te Huanga o te Ao Maori: Cognitive behavioural
therapy for Maori clients with depression—development and
evaluation of a culturally adapted treatment programme. A
dissertation presented in partial fulfilment of the requirements
for the degree of Doctor of Philosophy in Psychology, Massey
University, Wellington, New Zealand; 2009.
14. Durie MH, Hermansson G. Counselling Maori people in New
Zealand [Aotearoa]. Int J Adv Couns. 1990;13(2),107–118.
15. Bennett S, Flett R. Te Hua o te Ao Maori. He Pukenga Korero:
A Journal of Maori Studies. 2001;6(2), 29–34.
16. Hirini P. Counselling Maori clients—He Whakawhiti Nga
Whakaaro i te Tangata Whaiora Maori. NZ J Psychol.
1997;26(2):13–18.
17. Mathieson F, Collings S, Dowell A, Hatcher S, GoodyearSmith F, Stanley J. From technology transfer to collaboration:
an example of real world therapy adaptation (under review,
Cognitive and Behavioral Practice).
18. Beck A, Rush A, Shaw B, Emery G. Cognitive therapy of
depression. The Guilford Press; 1979.
19. Collings S, Mathieson F, Dowell A, Stanley J, Jenkin G, Goodyear-Smith F, Hatcher S. Acceptability of a self-help mental
health intervention in general practice. Fam Pract. 2011;0:1–7.
20.Goodyear-Smith F, Coupe N, Arroll B, Elley C, Sullivan S,
McGill A. Case finding of lifestyle and mental health disorders
in primary care: validation of the ‘CHAT’ tool. Br J Gen Pract.
2008 January; 26–31.
21. Andrews G, Slade T. Interpreting scores on the Kessler
Psychological Distress Scale (K10). Aust N Z J Public Health.
2001;25(6):494–97.
22.Davis L, Collings S. A bit set in my ways: clinicians’ willingness
to implement a primary mental health intervention. Social
Psychiatry and Population Mental Health Research Unit,
University of Otago Wellington; 2011.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
SHORT REPORT
The anatomical placement of body organs
by Australian and New Zealand patients and
health professionals in general practice
Marjan Kljakovic MBChB, FRNZCGP, PhD;1 Jo Risk BN, MPHTM2
Academic Unit of General
Practice and Community
Health, School of General
Practice, Rural and
Indigenous Health, Australian
National University Medical
School, Woden, ACT,
Australia.
1
ABSTRACT
INTRODUCTION: Understanding patients’ awareness of the anatomical placement of their body organs
is important for doctor–patient communication.
AIM: To measure the correct anatomical placement of body organs by people from Australian and New
Zealand general practices
METHOD: A questionnaire survey containing drawings of 11 organs placed in different locations within
each drawing.
After Hours Coordinator,
Southern NSW Medicare
Local, Australia
2
RESULTS: Among 1156 participants, there was no difference in the proportion of correct placement of
11 organs between Australian (51.7%) and New Zealand (49.6%) general practices. There was a positive correlation between the proportion of correctly placed organs and the age participants left school
(p=0.012) and a negative correlation with the number of GP visits in the previous year (p=0.040). Participants from rural Australia were more likely to correctly place organs than urban participants (p=0.018).
The mean proportion of organs correctly placed for doctors was 80.5%, nurses 66.5%, allied health
61.5%, health administrators 50.6% and the remaining consulting patients 51.3%.
DISCUSSION: Patients from Australian and New Zealand general practice were poorly aware of the correct placement of organs. Health professionals were moderately better than patients at correct placement.
KEYWORDS: Health knowledge; attitudes; practice; anatomy; general practice
Introduction
Methods
The general public has been poorly aware of the
anatomical placement of body organs for many
years. Three UK studies found that only 50%
of people correctly identified the placement of
organs.1–3 Understanding how patients place
their organs is important for doctor–patient
communication.1
A convenience sample of three general practices
from urban Australia, three from rural Australia, and two from urban New Zealand was
approached. All participants over 18 years of age
consented to completing the questionnaire while
sitting in waiting rooms during normal practice
hours over a three-day period. Health professionals from the practices, staff from the ACT
Division of General Practice, and staff from the
Southern General Practice Network also completed the questionnaire.
A literature search found only UK studies in this
area.1–4 The aims of this study were to test the
null hypothesis that the rate of correct placement
of organs was 50% for patients attending Australian and New Zealand general practices and to
compare the rate of correct placement of organs
by patients and health professionals.
Weinman’s cross-sectional questionnaire-based
design was replicated.1 Anatomical placement
was the dependent variable. The first part of
J PRIM HEALTH CARE
2012;4(3):239–241.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE239
ORIGINAL SCIENTIFIC PAPERS
SHORT REPORT
Table 1. Comparison of the percentage of correct anatomical placement of 11 organs for 1156 participants from Australia and New Zealand who reported
having the following chronic diseases: asthma, chronic obstructive pulmonary disease, diabetes, heart failure, or hypertension
Total
N (%)
Body organ
Asthma
N=142
COPD
N=26
Depression
N=151
Diabetes
N=75
Hypertension
N=257
94.0%
Bladder
1046
(93.5)
94.2%
96.2%
90.7%
83.8%†
93.3%
Intestine
1031
(91.3)
93.6%
88.5%
91.4%
90.7%
80.6% ‡
89.8%
Liver
636
(57.5)
61.9%
48%
57.4%
50.7%
58.6%
54.2%
Stomach
557
(49.6)
51.8%
38.5%
46.3%
45.2%
30% ‡
45.2%
Gallbladder
552
(50.5)
49.6%
65.2%
40.7%
47.9%
48.1%
54.1%
Pancreas
498
(45.6)
40.6%
48%
40.4%
46.5%
46.2%
51.0%
Heart
480
(42.9)
46.4%
38.5%
43.2%
45.2%
36.7%
36.4%§
Kidney
474
(42.2)
43.6%
46.2%
42.3%
38.4%
30.0%
44.2%
Ovaries
381
(34.1)
30.4%
52%
35.1%
38.7%
48.3%
32.4%
Lungs
351
(31.5)
28.1%
24%
31.1%
34.7%
35.5%
31.1%
Thyroid
270
(24.4)
17.9%
4.3%*
20.1%
17.8%
20.7%
25.8%
*
†
‡
§
p=0.024
p=0.001
p=0.033,
p=0.02
Table 2. Comparison of the percentage of correct anatomical placement of body organs by
1088 participants from occupations in Australia and New Zealand
Occupation
N
Mean % of correct placement
SD
Health professionals*
141
63.8%
18.9%
Teaching
56
51.8%
15.5%
Students
34
53.4%
17.3%
Employed
490
49.1%
16.1%
Not employed†
367
49.2%
16.3%
Total
1088
51.3%
17.2%
*
Includes doctors, nurses, allied health, health administrators
Includes unemployed, retired, at home, beneficiaries
†
Heart failure
N=26
ment of the practice; and number of times they
had visited a general practitioner (GP) and/or a
practice nurse over the previous 12 months.
The data were entered into PASW® Statistics 18
for appropriate statistical analysis. The Australian National University Human Ethics Committee and the New Zealand Health and Disability
Ethics Committee, University of Otago Medical School, approved the study. Questionnaire
responses were anonymous.
Results
the questionnaire consisted of drawings testing
the placement of the heart, lungs, stomach,
intestines, bladder, thyroid, liver, kidneys,
pancreas, gallbladder, and ovaries.1 Each drawing depicted four body outlines each with the
organ placed in different locations within an
outline. Participants selected one out of four
drawings they felt correctly placed the organ
within the body outline.
The independent variables were gender; age;
occupation; age on leaving full-time education;
which, if any, of the following chronic diseases
they had—asthma, chronic obstructive pulmonary disease (COPD), bronchitis/emphysema,
depression, diabetes, heart failure, and hypertension/high blood pressure; urban or rural place-
240
Out of 1184 questionnaires returned, 28 were
removed because participants were too young.
Australians compared to New Zealanders were no
different in their mean (SD) age (51.18 (16.23) years
versus 49.26 (18.04) years, t-test=1.621, p=0.105).
They left school at a slightly older age (19.20
(6.63) years versus 18.2 (6.25) years, t-test=2.115,
p=0.035). They visited their GP more often in the
previous year (4.32 (2.94) visits versus 3.59 (2.75)
visits, t-test=3.299, p<0.001). And visited the nurse
less often in the previous year (1.05 (2.14) visits
versus 1.97 (2.32) visits, t-test=-5.734, p<0.001).
The mean (SD) proportion of organs correctly
placed was 55.1% (19.2%) with no difference between Australia (51.7% (7.1%)) and New Zealand
(49.6% (17.4%)).
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
SHORT REPORT
There was no gender difference in the overall
mean proportion of correct placement of organs
(males 50.0% versus females 52.0%, p=0.061).
There was a positive correlation between
correct placement and the age participants
left school (r=0.076, p=0.012). There was a
negative correlation between correct placement
and the number of GP visits in the previous
year (r=-0.061, p=0.040). Participants from
rural Australia were more likely to correctly
place organs than from urban Australia (mean
(SD) correct placement 5.68 (1.94) versus 5.41
(1.90), t=2.36, p=0.018). There was no correlation found for age of patient, number of nurse
visits in the previous year and the number of
reported chronic diseases.
Table 1 shows no difference in the proportion of
correctly placed organs for participants reporting they had asthma or depression. Participants
reporting COPD were less likely to correctly
place the thyroid (Fisher’s exact test, p=0.034).
Participants reporting diabetes were less likely
to correctly place the bladder (χ2=11.484, df=1,
p=0.001). Participants reporting heart failure
were less likely to correctly place the intestine
(χ2=4.549, df=1, p=0.033) and the stomach
(χ2=4.528, df=1, p=0.033). Participants reporting
hypertension were less likely to correctly place
the heart (χ2=5.396, df=1, p=0.02).
Table 2 lists the occupations of 1088 participants
including 27 (2.5%) doctors, 40 (3.7%) nurses, 38
(3.5%) health administrators and 37 (3.4%) allied
health workers. The mean (SD) proportion of
organs correctly placed for doctors was 80.5%
(11.5%), nurses 66.5% (13.4%), allied health 61.5%
(18.1%), health administrators 50.6% (19.7%) and
the remaining consulting patients 51.3% (17.2%).
Health professionals (63.8%) were modestly better
than the remaining occupations (51.3%) at correctly placing organs (one-way ANOVA, p<0.001).
Discussion
This study found people from Australia and
New Zealand were poorly aware of the correct
anatomical placement of 11 organs—a finding no
different from the UK.1 The biological characteristics of age, gender (as in the UK1), and chronic
disease did not appear to influence the correct
WHAT THIS GAP FILLS
What we already know: Patients in the United Kingdom have a poor
understanding of anatomy.
What this study adds: Patients from Australian and New Zealand general practice also are poorly aware of the correct anatomical placement of
organs. Health professionals were moderately better than patients at correct
placement.
placement of organs. Social characteristics such as
education (as in the UK,1 the longer patients were
educated, the more correct they were at placing
organs), living in a rural location in Australia, or
access to general practice services did appear to
have an influence.
A limitation of this study is that it did not
distinguish between patients’ personal experience
from what they had been taught when deciding
on the correct placement of organs.
Understanding how patients place their organs is
important for doctor–patient communication. For
example, only 28% of patients with asthma could
place their lungs correctly. This poor understanding of lung anatomy might influence the poor
peak flow meter technique found among patients
with asthma.5 Furthermore, the negative correlation between the correct placement of organs and
the number of GP visits in the previous year, and
the lack of correlation with visits to the nurse,
suggests contact with health professionals did not
add to patients’ knowledge of anatomy. Perhaps
also, communication difficulties arose because
health professionals were only modestly better
than their patients at correctly placing organs.
References
1. Weinman J, Yusuf G, Berks R, Rayner S, Petrie KJ. How accurate is patients’ anatomical knowledge: a cross-sectional,
questionnaire study of six patient groups and a general public
sample. BMC Fam Pract. 2009;10:43.
2. Rashid A, Jagger C. Patients’ knowledge of anatomical location of major organs within the human body: a comparison
between Asians and non-Asians. Family Pract 1996;13(5):450.
3. Boyle C. Difference between patients’ and doctors’
interpretation of some common medical terms. BMJ.
1970;2(5704):286–89.
4. Leventhal H, Weinman J, Leventhal EA, Phillips LA. Health
psychology: the search for pathways between behavior and
health. Annu Rev Psychol. 2008;59:477–505.
5. RNZCGP Wellington Faculty General Practice Network, Kljakovic M. Utilisation of the peak flow meter for acute asthma in
general practice. NZ Fam Physician 2000;27(3):58-64.
ACKNOWLEDGEMENT
The authors would like
to thank the people who
contributed to this study.
FUNDING
This study was funded by
the PHCRED researcher
development programme.
COMPETING INTERESTS
None declared.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE241
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
Evaluation of Tu Meke PHO’s Wairua
Tangata Programme: a primary mental health
initiative for underserved communities
Sally Abel PhD;1 Bob Marshall PhD;1 Donny Riki BASS (psychotherapy);2 Tania Luscombe BAgEcon, DipTchg2
Eastern Institute of
Technology, Hawke’s Bay
1
Wairua Tangata Kaiwhakaora
Hinengaro/Lead Practitioner,
Innov8 Group Ltd
2
ABSTRACT
BACKGROUND AND CONTEXT: New Zealand’s primary mental health initiatives (PMHIs) have successfully filled a health service gap and shown good outcomes for many presenting with mild to moderate
anxiety/depression in primary health care settings. Maori have higher rates of mental health disorders
and complexity of social and mental health needs not matched by access to PMHIs.
ASSESSMENT OF PROBLEM: The Wairua Tangata Programme (WTP), a Hawkes Bay PMHI, aimed to
provide an integrated, flexible, holistic, tikanga Maori–based therapeutic service targeting underserved
Maori, Pacific and Quintile 5 populations. External evaluation of the programme provided formative and
outcome feedback.
RESULTS: The WTP reported high engagement of Maori (particularly women), low non-attendance
rates, good improvements in mental health assessment exit scores, strong stakeholder support and service user gratitude. GPs reported willingness to explore mental health issues in this high needs population. Challenges included engaging Pacific peoples and males and recruiting from scarce Maori, Pacific
and male therapist workforces.
STRATEGIES FOR IMPROVEMENT: Effectively meeting the target population’s complex social and
therapeutic needs required considerable programme flexibility, referral back into the programme and
assistance with transitioning to other therapeutic or social support services. Referral criteria required
adaptation to accommodate some sectors, especially youth. A group programme was developed specifically for males.
LESSONS: A holistic PMHI programme delivered with considerable flexibility and a skilled, culturally fluent team working closely with primary care providers can successfully engage and benefit underserved
Maori communities with complex social and mental health needs. Successful targeted programmes are
integral to reducing mental health disparities.
KEYWORDS: Primary health care; mental health; Maori; medically underserved areas; evaluation.
J PRIM HEALTH CARE
2012;4(3):242–248.
Background
CORRESPONDENCE TO:
Sally Abel
Senior Research Fellow,
Eastern Institute of
Technology, PB 1201,
Hawkes Bay Mail Centre,
Napier 4142, New Zealand
sabel@eit.ac.nz
In New Zealand, over a third of general practice patients are reported to have a diagnosable
mental disorder, most commonly conditions
relating to anxiety, depression and substance
use.1 Major time constraints can militate
against GPs counselling effectively within the
context of the general practice setting,2 yet
private therapy is costly and community-based
242
secondary care services, although free, are very
stretched and have long waiting lists.3 The
Ministry of Health (MoH) funded primary
mental health initiatives (PMHIs), which
commenced in 2004, allowed primary health
care providers around the country to establish
programmes suited to their patient population
that could address mild/moderate anxiety or
depression and prevent progression into more
complex (and costly) conditions. An evaluation
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
of the first round of PMHI programmes found
that a number of different models of care were
developed, including some Kaupapa Maori
programmes; programmes were viewed very favourably by primary health care providers and
their patients; and some important service-user
outcomes were demonstrated.3
The PMHIs (both mainstream and Kaupapa
Maori) were intended to be responsive to Maori
and an aim of their evaluation was to assess
whether they were reducing mental health disparities and improving health outcomes.3 Maori
have higher rates of mental health disorders that
are not matched by access to mental health interventions.4 In addition, NZ GPs are less likely
to diagnose depression in Maori patients than in
non-Maori patients.5 The PMHI evaluation found
that Maori comprised 17.5% of service users in
the programmes evaluated, slightly higher than
the 15% in the general population, and Kaupapa
Maori and some mainstream PMHI programmes
were considered responsive to Maori. However,
many providers experienced difficulty providing Maori-focused programmes and recruiting
a Maori workforce, and the evaluators noted
that there remained a relative underutilisation
of PMHI services by Maori, given their higher
prevalence of mental health conditions. Evaluation feedback from Maori PMHI service users
also highlighted the multiple everyday life
stresses they faced and the sheer complexity of
their mental health issues.3
This paper reports on an evaluation of a
primary mental health initiative in Hawkes
Bay that was developed a little later than the
above-mentioned programmes. The Wairua
Tangata Programme (WTP) specifically targets
Maori, Pacific and NZDep Quintile 5 communities using a holistic tikanga Maori–based
approach, and has shown some success at engaging and improving outcomes for this historically underserved population. The aims of the
evaluation were to provide formative feedback
to the implementation team and, through the
collection and analysis of process and outcome
data, to determine the success of programme
outcomes. The paper reports on results from the
programme’s first year with further follow-up
results and comments.
WHAT GAP THIS FILLS:
What we already know: Primary mental health initiatives (PMHIs) have
shown successful outcomes for many presenting with mild to moderate anxiety/depression in the primary health care setting, but appear to be under­
utilised by Maori who have higher rates of these conditions.
What this study adds: A holistic PMHI programme delivered with flexibility and a skilled, culturally fluent team who work closely with primary care
health practitioners can successfully engage and benefit underserved Maori
communities with complex social and mental health needs.
Context
The WTP was established in 2008 by Tu Meke
First Choice PHO (TMFCPHO), which at that
time serviced a high needs population of 13 712
people (including 47% Maori and 11% Pacific)
resident in Hastings and Flaxmere, Hawkes Bay.
TMFCPHO was one of the three Hawkes Bay
PHOs that have since been amalgamated into
one, Health Hawke’s Bay: Te Oranga Hawke’s
Bay. The WTP was funded through the second
round of MoH PMHI contracts. Its target population was 18–60-year-old Maori, Pacific residing
in an NZDep Quintile 5 area. Access was by GP
referral and, as was required by the MoH contract, a mental health assessment tool was used
prior to entry and on exit from the programme.
The Kessler-10 (K10) assessment tool was chosen
from a range of options, although none had
been validated for Maori. The K10 criterion for
admission was a score of 20–29 (mild–moderate
depression and/or anxiety) out of a possible 50.
Those referred to the programme received an
initial therapeutic programme of four to six (more
or less) sessions of counselling or psychotherapy
and the services of a social worker if required.
The service was free of charge.
Initiation of the programme was driven by the
PHO management and general practitioners. The
programme design was developed by a predominantly Maori team who were mindful of early
evaluation feedback about the successes and
weakness of other initiatives around the country.6
A popular modality used in other PMHIs was
cognitive behavioural therapy (CBT). Although
one early commentator argued that this cognitive
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE243
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
approach may not work well for Maori,8 recent
research on how CBT might be adapted to be responsive to Maori looks promising.7 However, the
WTP team decided on a more holistic approach
with spiritual and whanau dimensions.
The programme was embedded in a Maori framework and ethos that embraced all comers. Practice
guidelines embraced a holistic view of the person
founded on Te Whare Tapa Wha model9 and on
a parallel Pacific Fonofale model (developed by
Traci Tuamaseve, Trail Media, Flaxmere). Key
features considered important and integral to the
programme were:
• an integrated model at both structural and therapeutic levels
• considerable flexibility in a range of domains
(e.g. venue, time, style of engagement and
personnel) to enable appropriate responsiveness
• a polymodal, systemic, strengthsbased therapeutic approach
• tikanga Maori–based practice, including
whakawhanaungatanga (acknowledging
relationships), whakawatea/whakanoa (creating a sense of safety), whakapapa/pepeha
(reclaiming ancestral origins), waiata/haka
composition (expression of new beginnings) and decolonisation techniques (dealing with the sense of historical injustice)
• inclusion of whanau, when appropriate
• prompt, face-to-face engagement with
the programme and therapist.
Tikanga Maori–based practice is delivered from
a contemporary understanding of a traditional
Maori worldview that provides a context to
remember, reclaim and reaffirm the empowering
elements of Maori cultural heritage. The practice
provides spaciousness that aims to counteract the
negative effects of colonisation and proactively provide the potential to expand, transform and heal.
The programme was led by an experienced
Maori service development manager and a Maori
therapist, the lead practitioner, with a programme
advisory team and support from the PHO management and board. The therapeutic team comprised the full-time lead practitioner, a part-time
Pacific social worker and a number of therapists
or counsellors who were contracted part-time to
244
the programme. The selection of therapists, most
of whom were Pakeha women, was based on both
cultural competence and appropriate professional
scope of practice. Cultural supervision was provided by the lead practitioner. The social worker
assisted service users with a range of practical
problems, including liaison and advocacy around
access to benefits and services, assistance with
budgeting and food, and transport to therapy
and other services. The team liaised closely
with PHO clinical staff, providing programme
information and training, including cultural
competency, where necessary. Some data not
required by the contract but considered necessary
to monitor for meaningful and positive outcomes
(such as attendance rates, onward pathways and a
satisfaction survey) were collected.
Assessment
Evaluation method
The Eastern Institute of Technology Hawke’s Bay
was commissioned by the PHO to undertake an
evaluation of the WTP in early 2008. The evaluation objectives were to describe the service-user
population and their use of the service, report
on effects of the therapeutic treatment in terms
of changes to K10 scores, and assist programme
improvement by identifying implementation process issues. As no service users were interviewed
personally, the Central Regional Ethics Committee confirmed that the evaluation did not need
ethics approval or expedited review.10
The evaluation covered the first 15 months of
the programme: 1 April 2008 to 30 June 2009. A
mixed methods approach was used to provide a picture of formative issues and programme processes
and outcomes.11 Qualitative data were obtained
from in-depth interviews or focus groups with
key informants, the formative evaluator’s notes on
team meetings, and document review. Open-ended
interview questions focused on participants’ views
of programme progress, what they considered key
programme strengths and difficulties, and what
recommendations they had for improvement. In
the early phase, 13 key people were interviewed as
part of the formative evaluation. Face-to-face key
informant interviews or small focus groups were
then undertaken midway (n=15) and at the end of
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
the first 15 months (n=21), with many people interviewed on both occasions. Those interviewed
at least once included therapists (6), social worker
(1), community worker (1), general practitioners
(GPs) (10), nurse (1); admin/management staff
(6). The 10 GPs interviewed had made 72% of all
GP referrals to the programme. Quantitative data
were obtained from the programme database. This
comprised service user demographics, patterns
of service use and K10 pre- and post-treatment
scores. In addition, service-user satisfaction
surveys, which comprised both quantitative and
qualitative components, were analysed. For this
paper, some descriptive quantitative data for the
programme’s second MoH contract (July 2009 to
June 2010) have also been included and compared
to the previous period.
Outcome evaluation results
Quantitative data
The quantitative data (Table 1) indicated that the
programme successfully reached most of its target
population, with particularly high engagement of
Maori women, high appointment attendance rates
and improvement in average exit K10 scores, the
latter being slightly higher than the 80% average
shown in the national evaluation.3 The low nonattendance (DNA) rates recorded are considered
very good for therapy in the primary health
setting,12,13 and are likely to be particularly so for
this demographic group. All the above measures
were demonstrated to improve over the two-year
period. The engagement of Pacific peoples and
men, however, was low and remained so despite
efforts at improvement.
Entry K10 scores tended to be considerably
higher than the admission criteria. In the first
15-month period, the average score was 33.4,
with 73% of users having a score of 30 or more.
Although exit K10 scores averaged 25.3, a highly
significant (p<0.001) improvement, this was still
in the mid-range of scores denoting a mild/moderate depression or anxiety.
In the first 15-month period, the majority (79%) of
service users were diagnosed with some form of
depression (depression, moderate depression, reactive depression, postnatal depression). Other diag-
Table 1. WTP quantitative outcomes
2008–2009
% (n)
2009–2010
% (n)
Maori
65% (138)
71.5% (236)
European
Referrals
23% (49)
25.8% (85)
Pacific
3% (6)
1.5% (5)
Other
9% (19)
1.2% (4)
Females
75%
74%
Males
24%
26%
No. of packages of care
257
330
No. of therapeutic sessions
1228
1860
Average sessions per package of care
4.8
5.6
No. of social worker interventions
204
262
Attendance rates
86.4%
84.5%
Did not attend (DNA) rates
10.2%
5.3%
Late cancellation
3.4%
10.2%
Kessler 10 score—reduced
87%
83%
Kessler 10 score—increased
5%
8%
Kessler 10 score—no change
8%
9%
noses included anxiety, post-traumatic stress disorder, stress, grieving and relationship problems.
Anecdotal reports of high levels of distress and
comorbidities were confirmed by the K10 scores,
stakeholder interview data and the programme
data­base, with 71% of service users having physical and/or mental comorbidities recorded. Those
who required more than the standard package of
care were either referred back into the programme
(4%) or on to other services (20%).
Service user feedback
Service users completed a short satisfaction
survey approximately six weeks after exiting
the programme. Results must be viewed knowing that this was undertaken over the phone
by a therapist and thus responses may be more
positive than if collected by an independent
person. Within the first 15-month period, 113
of the 170 people who had exited the programme
at least six weeks before had provided feedback
via the survey. Table 2 details responses to the
closed response questions. Some did not answer
all questions and percentages are of those who
responded. They show that a significant majority
of those providing feedback responded positively
to all questions.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE245
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
Table 2. WTP satisfaction survey responses six weeks post-exit
Yes
n (%)
No
n (%)
More content and happier in yourself?
88 (84%)
17
Healthier from a spiritual point of view?
73 (73%)
27
Stronger in yourself as a Maori or other cultural group
you identify with?
67 (72%)
26
More able to set goals for yourself?
86 (81%)
20
More able to think and feel positive?
82 (77%)
24
More able to manage unwelcome thoughts and feelings?
72 (67%)
35
More committed to having good physical health?
73 (72%)
28
More able to communicate with your whanau?
95 (88%)
13
More confident in your relationships with other people?
87 (81%)
20
105 (98%)
2
As a result of the counselling/therapy programme do you
generally feel:
As a result of the counselling/therapy programme are you:
Were you happy with our service?
Responses to the small number of open-ended
questions gauging satisfaction with the service
were very positive, with strong appreciation
expressed for the kindness and support of the
therapists and social worker, the availability of
Maori therapists, the fact the service was no cost,
the flexibility around venue and the ability to
involve whanau members.
Stakeholder feedback
Stakeholder interviews showed strong confidence
in the WTP team and good relationships between
the team and primary care practices. General
practitioners felt many of their patients did
not seek help unless their situation was serious
and, whilst previously they might have avoided
probing a problem in the 15-minute consultation,
they reported an increased willingness to pursue
a patient’s depression or anxiety because of their
confidence in the programme now available to
them. Some changes in GP prescribing practices occurred, with several reporting they used
medication less frequently or delayed use to see
if therapy was useful. General practitioners also
reported seeing important and significant changes
in many of their referred patients, such as visible
reductions in anxiety and distress and, in some
cases, major lifestyle changes.
246
Both GPs and therapists expressed ambivalence
about the cultural and social appropriateness
of the K10 assessment tool for this high-needs
Maori community, but it was considered useful to the extent that entry and exit scores
could be compared. Participating GPs, who were
very experienced in this community, reported,
however, that they preferred their own clinical
judgment to the K10 score when assessing the
appropriateness of the referral. Therapists trusted
their judgment and liaised closely with them.
The WTP commitment to accepting those with
K10 scores higher than the referral criteria meant
there was no temptation for GPs to adjust scores
downward in order for the person to be admitted
to the programme, as anecdotal comments suggest
may have occurred elsewhere.
Strategies for quality
improvement/change
This section describes quality improvement
strategies adopted by the team to address issues
identified through formative evaluation feedback and internal review. To effectively meet
the complex needs of many referred, more than
the standard package of care was often required.
This was achieved through referral back into the
programme for another package of care or transitioning on to other therapeutic or social support
services. The latter required the programme
manager to seek alternative funding options and
liaise with a range of agencies (e.g. Work and
Income NZ, Ministry of Social Development
and Accident Compensation Corporation). The
team found the requirement of GP referral to the
programme limited entry for those who did not
use GP services, so direct access through whanau
or self-referral was initiated in the second year.
Rangatahi/youth under 18 years were initially
not eligible for admission to the programme, but
the holistic therapeutic model placed importance
on the integrity of the whanau so strategies
such as including rangatahi in whanau sessions
and liaising with existing youth services were
explored as necessary. In the second year, those
aged 12 years and over became eligible for referral to the programme and were seen by either the
programme’s therapeutic team or the team of a
contracted dedicated youth service.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
Key informants considered reasons for relatively
low Pacific referral rates were complex, but
included Pacific community sensitivity around
confidentiality, unfamiliarity with seeking help
from outsiders, low usage of GP services through
which referral occurred, GPs not recognising
need because of cultural or language barriers, and
the lack of a Pacific therapist. To optimise effective engagement with those referred, the team
involved the Pacific social worker in first sessions
if appropriate.
Reasons for low male referral rates were seen
to be a combination of men being reluctant to
access therapy and the shortage of male therapists. A male therapist was later recruited and
a men’s group programme, Tane Toa, funded
from an alternative source, was started in the
second year.
The scarcity of available Maori, Pacific and male
therapists was an ongoing issue. To increase the
pool of male and Maori therapists for the programme, a mentoring system was developed with
senior psychotherapy students from the regional
Eastern Institute of Technology. Ensuring availability of Maori and male therapists remained a
priority and, at the time of writing (September
2011), the therapeutic team comprises five therapists; three are Maori, one of whom is male.
Discussion
Programme data showed that the WTP successfully reached and maintained engagement with
many of the historically underserved target population. In addition, it showed successful outcomes
for many of those finishing the programme, with
ongoing referral if necessary.
Key features which differed from many mainstream PMHIs included the use of tikanga Maori
to build rapport, enhance feelings of safety and
strengthen cultural identity; the emphasis on culturally competent personnel; the availability of a
social worker; flexibility around venue and time;
and the inclusion of family/whanau if wanted. Issues identified through the formative evaluation,
for which quality improvement strategies were
developed, were generally specific to high needs,
underserved populations.
Many of the WTP’s reported successes (improvements in K10 scores, stakeholder support
and service-user gratitude) and difficulties (low
recruitment of Pacific peoples and men and lack
of available Maori, Pacific and male therapist
workforce) were a feature of other PMHIs around
the country.3 However, high Maori engagement,
low non-attendance rates and high percentage improvements in K10 exit scores for this population
are distinctive WTP features.
Two possible explanations might account for the
high entry K10 scores and, although significantly
reduced, relatively high exit scores. Firstly, that
those referred were the more distressed of a
population in which high levels of distress and
anxiety are perhaps the norm. Secondly, as key
informants in both this and the national PMHI
evaluation6 have suggested, that the assessment
tool might not be as meaningful or culturally
appropriate for this population. Despite ambivalence about the tool, both GPs and therapists
were happy with the referral process and service
users who required more or ongoing therapy or
support were assisted on to other services. An
evaluation recommendation, however, was that
the K10 entry criteria be reassessed.
Perhaps more relevant markers of success for this
population were the low DNA rates, GPs’ confidence in the programme and reported observed
improvements in their patients. Of note was
GPs’ greater willingness to pursue mental health
issues in this high needs population and reported
changes in their prescribing practices.
Lessons and messages
A key message to take from the WTP programme
is that a holistic, tikanga Maori–based programme
delivered with considerable flexibility and skilled,
culturally fluent programme management and
therapeutic teams who work closely with primary
care providers can successfully engage and benefit
underserved communities with complex social
and mental health needs. The complexity of need
and high prevalence of comorbidities amongst
Maori service users are consistent with national
data14 and, given Maori have higher unmet need
for general practitioner services than the general
population,15 alternative referral pathways to
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE247
ORIGINAL SCIENTIFIC PAPERS
IMPROVING PERFORMANCE
PMHIs and a dedicated specialist team, such as
the WTP, appear necessary to ensure services to
this population.
The PMHIs have clearly increased services to,
and shown benefits for, the general population,
including Maori, and new developments, such
as screening tools16,17 and brief interventions in
the primary health care setting,18 continue to be
assessed. While the general view is that Maori
probably benefit best from having both Kaupapa
Maori and mainstream PMHI models available,3
the challenge is to ensure that new developments do not disproportionately benefit some
groups over others and increase mental health
disparities. A recent NZMA position statement,
supported by mounting research evidence, has
prioritised a focus on reducing health disparities
in New Zealand.19 This signals to PMHI funders
and providers the importance of ensuring that
new and existing services are at least as effective
for Maori and others in underserved communities
as the general population and that successfully
targeted programmes, like the WTP, which are
developed around the specific needs in these communities, are sufficiently resourced.
ACKNOWLEDGEMENTS
We wish to thank the
erstwhile Tu Meke First
Choice PHO Operations
Manager and Board for
providing access to WTP
data and supporting the
writing of this paper and
the busy professionals
interviewed for the
evaluation. We would
also like to acknowledge
Dr David Tipene-Leach
and two anonymous
reviewers for their helpful
peer review comments.
FUNDING
We are grateful to Tu
Meke First Choice
PHO for funding the
evaluation and EIT
Hawke’s Bay for funding
the writing of this paper.
COMPETING INTERESTS
Donny Riki is the WTP
lead practitioner and
Tania Luscombe is the
WTP project manager.
248
8. Hirini, P. Counselling Maori clients: He whakawhiti nga
whakaaro i te tangata whaiora Maori. NZ J Psych. 1997;
26(2):13–18.
9. Durie M. Whaiora: Maori health development. Auckland:
Oxford University Press; 1994.
10. Abel S, Marshall B. Evaluation of the Wairua Tangata Project,
Tu Meke First Choice PHO’s primary mental health initiative,
Hawke’s Bay. Final report, April 2008–June 2009. Hawke’s
Bay: Eastern Institute of Technology; 2009.
11. Patton MQ. Qualitative research and evaluation methods. 3rd
ed. Thousand Oaks: Sage Publications; 2002.
12. Gilbert N, Barkham M, Richards A, Cameron I. The effectiveness of a primary care mental health service delivering brief
psychological interventions: a benchmarking study using the
CORE system. Prim Care Ment Health. 2005;3(4):241–251.
13. Hamilton R, Gordon P, Naji S. Service innovation: the first year
of a brief psychiatric screening clinic in primary care. Psychiatric Bulletin. 2002;26:218–21.
14. Baxter J. Maori mental health needs profile—summary: a
review of the evidence. Wellington: Ministry of Health; 2008.
15. Ministry of Health. A portrait of health: key results of the
2006/07 New Zealand Health Survey. Wellington: Ministry of
Health; 2008.
16. Calveley J, Verhoeven A, Hopcroft D. A patient-centred referral pathway for mild to moderate lifestyle and mental health
problems: does this model work in practice? J Prim Health
Care. 2009;1(1):50–56.
17. Goodyear-Smith F, Arroll B, Coupe N, Buetow S. Ethnic
differences in mental health and lifestyle issues: results
from multi-item general practice screening. NZ Med J. 2005;
18(1212):U1374.
18. Mathieson F, Collings S, Dowell A. Sub-threshold mental
health syndromes: finding an alternative to the medication of
unhappiness. J Prim Health Care. 2009;1(1):74–7.
19. New Zealand Medical Association. Health equity position
statement. NZ Med J. 2011;124(1330):99.
References
1. The MaGPIe Research Group. The nature and prevalence of
psychological problems in New Zealand healthcare: a report
on mental health and general practice investigation. NZ Med J.
2003;116(1171):1–15.
2. Hutton C, Gunn J. Do longer consultations improve the
management of psychological problems in general prac­tice? A
systematic literature review. BMC Health Serv Res. 2007 May
17;7:71. PMID:17506904.
3. Dowell AC, Garrett S, Collings S, McBain L, McKinlay E,
Stanley J. Evaluation of the Primary Mental Health Initiatives:
summary report 2008. Wellington: University of Otago and
Ministry of Health; 2009.
4. Oakley Browne MA, Wells JE, Scott KM, editors. Te Rau
Hinengaro—the New Zealand Mental Health Survey. Wellington: Ministry of Health; 2006.
5. Thomas DR, Arlidge B, Arroll B, Elder H. General practitioners’
views about diagnosing and treating depression in Maori and
non-Maori patients. J Prim Health Care. 2010;2(3):208–16.
6. Department of Primary Healthcare and General Practice.
Interim report: primary mental health initiatives evaluation.
Wellington: School of Medicine and Health Sciences, University of Otago; 2007.
7. Bennett ST, Flett RA, Babbage, DR. The adaptation of cognitive behavioural therapy for adult Maori clients with depression: a pilot study. In: Levy M, Nikora LW, Masters-Awatere B,
Rua M, Waitoki W, editors. Claiming spaces: proceedings of
the 2007 national Maori and Pacific psychologies symposium;
23–24 November 2007, Hamilton, New Zealand. Hamilton:
Maori and Psychology Research Unit, University of Waikato;
2008. p. 83–91.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
CONTINUING PROFESSIONAL DEVELOPMENT
COCHRANE CORNER
PEARLS
Topical antibiotics are
probably better than placebo
for acute conjunctivitis but
most get better anyway
Bruce Arroll MBChB, PhD, FRNZCGP; Professor of General Practice
and Primary Health Care, The University of Auckland, PB 92019,
Auckland, New Zealand; Email: b.arroll@auckland.ac.nz
THE PROBLEM: Acute bacterial conjunctivitis is an infec-
tive condition in which the eyes become red and inflamed.
The condition is not normally serious and usually recedes
spontaneously within about a week. People with acute conjunctivitis are often given antibiotics, usually as eye drops or
ointment, to speed recovery. If there is any loss of vision, the
problem is more serious and needs an immediate eye consult.
The benefits of antibiotics to the sufferer of conjunctivitis
have been questioned. I am always impressed by the ‘mass
hysteria’ of ‘pink eye’ in day care centres where the staff act
like it was the plague as opposed to a self-limiting viral infection. However, there are cases of bacterial infection and I
am more inclined to give antibiotics if the eye is really stuck
down in the morning.
CLINICAL BOTTOM LINE: The review of trials found that
the signs of conjunctivitis went away more quickly in people
taking antibiotics, but the benefits are marginal as in most
cases the infection is self-limiting. However, most cases resolve spontaneously with clinical remission being achieved in
65% (95% CI 59–70) by days 2–5 in those receiving placebo.
Treatments for acute bacterial conjunctivitis with topical antibiotics
Topical
antibiotics
vs placebo
Success
Evidence
Harms
Effective;
NNT = 6
(range 6–15)
Cochrane
review1
No major
harms
String of PEARLS
Practical Evidence About Real Life Situations
Musculoskeletal conditions
PEARLS are succinct summaries of Cochrane Systematic Reviews for
primary care practitioners—developed by Prof. Brian McAvoy for the
Cochrane Primary Care Field (www.cochraneprimarycare.org), New
Zealand Branch of the Australasian Cochrane Centre at the Department
of General Practice and Primary Health Care, University of Auckland
(www.auckland.ac.nz/uoa), funded by the Ministry of Health (www.
health.govt.nz), and published in NZ Doctor (www.nzdoctor.co.nz.).
Pronation may be more effective than supination in
correcting pulled elbow
Local corticosteroid injections improve symptoms of
carpal tunnel Corticosteroid injections are effective for trigger finger
Oral steroids are effective short-term treatment for
adhesive capsulitis
Topical glyceryl trinitrate may be effective in rotator
cuff disease
Surgery for rotator cuff disease is no more effective
than active non-surgical treatment
Insufficient evidence of benefit of topical rubefacients
for acute and chronic painful musculoskeletal
conditions in adults
DISCLAIMER: PEARLS are for educational use only and are not meant
to guide clinical activity, nor are they a clinical guideline.
NNT = numbers needed to treat. An NNT of 6 means that for every six people given
the treatment, one additional person will get better due to the effective treatment
Reference
1. Sheikh A, Hurwitz B. Antibiotics versus placebo for acute bacterial conjunctivitis. Cochrane Database of Systematic Reviews. 2006, Issue 2. Art. No.:
CD001211. DOI:
All people residing in New Zealand have access to the Cochrane Library
via the Ministry website www.health.govt.nz/cochrane-library
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE249
CONTINUING PROFESSIONAL DEVELOPMENT
VAIKOLOA
Hearing loss among Pacific peoples
Ofa Dewes PhD
N
VAIKOLOA
Pacific Primary
Health Care
Treasures
Vai (water)
is a symbol of
‘life-source’ and
koloa (treasures)
to share
oa’ia e mauri. Pacific peoples in Aotearoa
New Zealand represent a distinct population group. With a population of approximately 266 000, we are undergoing significant
demographic changes and growing rapidly into a
sizeable number and social significance.1,2
Low health indicators, particularly in relation
to non-communicable diseases and capacity and
capability gaps that impact service delivery, highlight for us the urgent need for more effective
and efficient services, including models of care
for Pacific peoples and the development of Pacific
capacity and capabilities.3,4,5,6 A health indicator
in the health and disability sector which falls
into the non-communicable disease category and
calls for our attention is hearing loss.
Hearing loss carries a financial burden on individuals, their families, and on governments.
The effects of hearing impairment can impact
our children’s education, social development and
quality of life.7,8,9 Among adults, hearing loss
can result in poor communication, social isolation, reduced employment opportunities and poor
quality of life.7,8,9 Untreated ear disease can have
serious clinical consequences such as middle ear
erosion and chronic infections as well as brain
abscesses and meningitis. According to the World
Health Organization, hearing loss and ear disease
is considered to be highly prevalent in developing countries with estimates of up to 21% of the
population affected.10,11
J PRIM HEALTH CARE
2012;4(3):250–251.
CORRESPONDENCE TO:
Ofa Dewes
School of Population
Health, The University
of Auckland,
PB 92019, Auckland,
New Zealand
o.dewes@auckland.ac.nz
250
There is some anecdotal evidence on population groups in the Pacific region which supports
high prevalence estimates. However, services are
fragmented and variable. Services are generally ad
hoc or focused around specific non-governmental
organisations with voluntary help provided by
nurses, hearing therapists, audiologists and ENT
surgeons. Our knowledge and understanding of
hearing loss prevalence among Pacific peoples is
also limited.
Credible information and evidence to help
leverage appropriate resources to meet the needs
of Pacific peoples and inform national policy
development and services are required. Motivations to reduce the burgeoning cost of hearing loss
through preventative efforts and decisive action
that will lead to service and clinical quality improvement and innovation in service delivery for
Pacific peoples are warranted. In New Zealand the
government is committed to leading significant
change in the health and disability sector through
its increased focus on evidence-based decisionmaking processes and by prioritising resources for
frontline services.12,13,14
Here at the School of Population Health we are
committed to overcoming this knowledge gap and
developing a strong relationship with other universities in the region, especially around research and
education initiatives. Growing interest is emerging
to utilise Pacific researchers and the expertise in
our Audiology section to look into the nature of
hearing loss and assist with the development of sustainable services for Pacific children, young people
and adults. This interest has led us to conduct an
epidemiological pilot study on hearing loss among
the Fijian (Indigenous Fijian, Indo-Fijian, Rotuman)
population in Auckland to determine the prevalence of hearing loss and ear disease in this group.
Study findings have been disseminated to the Fijian
communities in Auckland and in Fiji, highlighting the need to strengthen the global discourse on
hearing loss among Pacific peoples, to identify their
needs and regional distribution, inform service
development and explore opportunities to develop a
critical mass of Pacific frontline workers including
audiologists and hearing therapists to provide and
maintain hearing services for Pacific peoples.
We are committed to strengthening and maintaining collaborative relationships with key stakeholders and Pacific communities to develop sustainable
hearing services for Pacific peoples. We are also
committed to generating new knowledge and
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
CONTINUING PROFESSIONAL DEVELOPMENT
POTION OR POISON?
articulating the issues that Pacific peoples face, as
well as encouraging public debate to improve the
hearing health for Pacific peoples. In this connection, some of the implications for future work on
hearing loss among Pacific peoples may include
the need to:
Colloidal silver • overcome data limitations by collecting credible evidence, investigating the
hearing health of Pacific peoples by ethnicity, and describing the prevalence
of health conditions of each group
• know what’s important and works for Pacific
peoples and their lived realities in order to improve care for them and maintain relationships
• understand the issues within the institutional
framework in which they currently exist
• work across other sectors like education
• support local ownership of services that
are adaptable, innovative and responsive
to the needs of Pacific peoples, and
• develop local capacity and capability to support
hearing services for and with Pacific peoples.
Silver is a metallic element. Through the ages there has been the belief
that silverware used for water storage had disinfecting properties. People
are exposed to silver, usually in tiny amounts, through environment and
in certain work activities or hobbies. Colloidal silver is a suspension of
very small metallic silver particles in a liquid base. It has been marketed in
various forms for many years as a topical antimicrobial preparation and as a
dietary supplement to stimulate the immune system.
References
1. Statistics New Zealand. Pacific Peoples: 2006 Census of Population and Dwellings. Wellington: Statistics NZ; 2007.
2. Statistics New Zealand and Ministry of Pacific Island Affairs.
Demographics of New Zealand’s Pacific population. Wellington: Statistics NZ; 2010. ISBN 978-0-478-35344-0 (online).
3. Ministry of Health. A portrait of health: key results of the 2006/07
NZ Health Survey. Wellington: Ministry of Health; 2008.
4. Ministry of Health. Improving quality of care for Pacific peoples. Wellington: Ministry of Health; 2008.
5. Ministry of Health. The health of Pacific peoples. Wellington:
Ministry of Health; 2005.
6. Gribben B. Improving access to primary health care: an
evaluation of 35 reducing inequalities projects. Overview.
Wellington: Ministry of Health; 2007.
7. Greville A. Hearing impaired and deaf people in New Zealand:
an update on population numbers and characteristics. 2005.
[cited 2011 Nov]. Available from: http://www.grevilleconsulting.co.nz/HearingimpaireddeafpeopleNZMar05a.pdf.
8. Ministry of Health. Pacific peoples’ experience of disability: a
paper for the Pacific Health and Disability Action Plan Review.
Wellington: Ministry of Health; 2008.
9. Ministry of Health. Pacific child health: a paper for the Pacific
Health and Disability Action Plan Review. Wellington: Ministry
of Health; 2008.
10. World Health Organization. Deafness and hearing impairment. 2010. Available from: http://www.who.int/mediacentre/factsheets/fs300/en/.
11. World Health Organization, 2008. The global burden of
disease: 2004 update. Available from: http://www.who.int/
healthinfo/global_burden_disease/2004_report_update/en/.
12. Ministry of Health. Tupu Ola Moui: Pacific Health Chart Book.
Wellington: Ministry of Health; 2004.
13. Ministry of Health. Making a Pacific difference: strategic
initiatives for the health of Pacific peoples in New Zealand.
Wellington: Ministry of Health; 1997.
14. Minister of Health and Minister of Pacific Island Affairs. ‘Ala
Moui: Pathways to Pacific Health and Wellbeing 2010–2014.
Wellington: Ministry of Health; 2010.
David J Woods BSc (Hons), MPharm, MPSNZ, MRPharmS, FNZHPA
PREPARATIONS: Available products range from liquids for oral adminis-
tration to topical gels, ointments and sprays, usually supported by websites
that describe the manufacturing process and their silver content.
ACTIVE CONSTITUENTS: Elemental silver, usually its ionic form, is pro-
posed as the active ingredient as an antimicrobial and immunostimulant.
MAIN USES AND CLAIMS: Silver in various forms and salts has had
medicinal uses since ancient times. Most recently, silver nitrate has been
used to treat corns and warts and silver sulfadiazine to treat burns. These
uses should not be confused with the claims associated with colloidal
silver. Colloidal silver products are often marketed as dietary supplements
or topical products with various health-related claims, including that it
kills disease-causing agents such as bacteria, viruses, and fungi (alternative to prescription antibiotics); treats diseases such as cancer, HIV/AIDS,
diabetes, tuberculosis, syphilis, scarlet fever, shingles, herpes, pneumonia
and prostatitis; promotes bladder and lung health; and stimulates the immune system.
EVIDENCE FOR EFFICACY: Official drug compendia such as the United
States Pharmacopeia and National Formulary have not listed colloidal
silver products since 1975 due to lack of evidence of effectiveness and
growing concerns about possible toxicity. Colloidal silver products are still
advertised and available in New Zealand as an alternative therapy.
The scientific literature comprises numerous studies showing that silver in
various forms does possess in vitro antimicrobial activity, but there is no
clinical evidence of effectiveness. Whilst the intake or application of small
amounts of colloidal silver is unlikely to be harmful, chronic use or use of
Herbal medicines are a popular health care choice, but few have been
tested to contemporary standards. POTION OR POISON? summarises
the evidence for the potential benefits and possible harms of well-known
herbal medicines.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE251
CONTINUING PROFESSIONAL DEVELOPMENT
POTION OR POISON?
preparations with unstated or high silver content
may lead to significant adverse effects.1
A recent review by the National Center for
Complementary and Alternative Medicine in the
United States2 concluded that:
• silver has no recognised function in the body
and is not an essential mineral supplement
• silver should not be promoted as a cure-all or
to treat a ‘deficiency’ of silver in the body
• claims made about the effectiveness of
colloidal silver products for numerous
diseases are unsupported scientifically
• colloidal silver products can have
serious adverse effects
• the amounts of silver in supplements can vary
greatly, which can pose risks to the consumer.
Summary Message
Colloidal silver is widely marketed for a variety of
health benefits. A range of potentially useful in
vitro effects have been shown, but no scientific
evidence of actual patient benefit. Adverse effects are possible and are more likely with products with high silver content or long-term use.
References
1. Fung MC, Bowen DL. Silver products for medical indications:
risk-benefit assessment. J Clin Toxicol. 1996;34(1):119–126.
2. Colloidal silver products. A review by the National Center for
Complimentary and Alternative Medicine (NCCAM); August
2010. [cited 2012 Jan]. Available from: http://nccam.nih.gov/
health/silver.
ADVERSE EFFECTS: Adverse effects are relative-
ly unlikely if a product with a stated low amount
of colloidal silver is used for a short time. Longterm use can lead to argyria (silver salts deposit
in the skin, gums, nails, eyes, and internal organs
causes a permanent bluish-grey discolouration).1
Other possible adverse effects include neurological problems, renal damage, gastrointestinal
upset, headaches, fatigue, and skin irritation.
DRUG INTERACTIONS: Although there is no
supporting clinical evidence, it is possible that
colloidal silver taken by mouth may interfere
with the absorption of some drugs, e.g. penicillamine, quinolones, tetracyclines, and thyroxine.
J PRIM HEALTH CARE
2012;4(3):251–252.
CORRESPONDENCE TO:
David J Woods
School of Pharmacy,
University of Otago,
PO Box 56, Dunedin
9054, New Zealand
david.woods@otago.ac.nz
252
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
CONTINUING PROFESSIONAL DEVELOPMENT
NUGGETS OF KNOWLEDGE
Statins and memory loss
Linda Bryant MClinPharm, PGDipHospPharmAdmin, PhD, FNZHPA, FNZCP, FPSNZ, MCAPA
‘I read in the newspaper that statins may cause
dementia… so I want to stop my statin’
In February 2012 the FDA Consumer Information website1 warned that statins may cause subtle cognitive impairment such as mild memory
loss or forgetfulness and ‘fuzzy’ or unfocused
thinking. This uncommon adverse effect is
reversible on stopping the statin. The mild cognitive impairment is not dementia. Statins do not
prevent or treat dementia per se,2,3 but may help
reduce risk of multi-infarct or vascular dementia.
It is important for the patient to know that subtle
changes in memory or cognitive function does
not mean statin-induced dementia.
Onset of cognitive impairment may be within
weeks or after several years of statin therapy. The
median time of onset is about six months.1,2 In a
survey of 171 people with self-reported memory or
cognition impairment, improvement was reported
a median of two to three weeks after stopping the
statin. A number of patients were rechallenged,
with rapid recurrence of cognitive impairment.4
The mechanism for statin-induced memory loss
is unclear, although it is likely to relate to the
medicine rather than the extent of cholesterollowering. There is a view that impairment may be
related to demyelination of CNS nerve fibres. Although it is difficult to distinguish between any
of the statins, it may be that pravastatin, with
less tendency to cross the blood-brain barrier or
being less potent, has less impact on memory.
Practical approach to the person who claims
to have statin-induced memory impairment
Because cognitive impairment is mild there is
a need to identify subtle changes in cognition,
usually at a high functioning level. It is difficult
to find a suitable evidence-based test of cogni-
tion for statin-induced cognitive impairment. If a
person thinks that their statin is causing cognitive
impairment, a possible method to test this is:
• Do a baseline TSH, lipid profile and
cardiovascular risk assessment.
• Administer the Montreal Cognitive Assessment (MoCA, http://www.mocatest.org/ )—takes 10–15 minutes.
• Stop statin for three months.
• Repeat MoCA and lipid profile.
• If cognitive function improves, rechallenge with a statin, perhaps pravastatin. Rechallenge is important in case
the decline in cognitive function was
coincidental to stress or depression.
KEY POINTS
Statins may cause mild
cognitive impairment:
• Assess cognitive
function
• Stop statins for three
months
• If function improves,
rechallenge with
statins
And another potential adverse effect—fatigue
A recent study found that statins may cause low energy and fatigue on exertion in up to 20% of people,
particularly women.5 Benefits of statins are well
established, and they certainly have a mortality
benefit. Application of this study is to use statins
for people with a calculated risk of having a cardiac
event the next five years >15%. For people with a
lower risk, the potential impact of fatigue on quality of life and activity may outweigh the benefits.
References
1 FDA expands advice on statin risks (for Consumers) 29 Feb
2012. http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm293330.htm. [cited 2012 Jun 15].
2. McGuinness B, O’Hare J, Craig D et al. Statins for the
treatment of dementia. Cochrane Database Syst Rev. 2010
(8):CD000714.
3. McGuinness B, Carig D, Bullock R, Passmore P. Statins for the
prevention of dementia. Cochrane Database Syst Rev. 2009
(2):CD003160.
4. Evans M, Golomb B. Statin-associated adverse cognitive
effects: survey results from 171 patients. Pharmacotherapy.
2009;29:800–11.
5. Golomb B, et al. Effects of statins on energy and fatigue with
exertion: Results from a randomized controlled trial. Arch
Intern Med 2012; doi:10.1001/archinternmed.2012.2171.
NUGGETS of KNOWLEDGE provides succinct summaries of pharmaceutical evidence about
treatment of common conditions presenting in primary care and possible adverse drug reactions.
J PRIM HEALTH CARE
2012;4(3):253.
CORRESPONDENCE TO:
Linda Bryant
Clinical Manager, Clinical
Advisory Pharmacist,
East Health Trust PHO
PO Box 38248, Howick
Auckland, New Zealand
l.bryant@auckland.ac.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE253
VIEWPOINT
From ladder to platform: a new concept for
pain management
Lawrence Leung MBBChir(Cantab), MFM(Clin), CCFP, FRACGP, FRCGP
ABSTRACT
BACKGROUND: Pain remains one of the top five reasons for consultations in general practice, presenting either alone or as comorbidity. The World Health Organization (WHO) analgesic ladder proposed in
1986 has been the cornerstone of pain management, but is often inadequate in daily practice, especially
when dealing with the diverse nature and etiology of various pain conditions. There is a need for a better
concept which is universally applicable that acknowledges the value of, and need for, other domains of
treatment for pain.
OBJECTIVE: This article reviews the original ideas of the WHO analgesic ladder and proposes its extension to a platform model in the context of pain management.
DISCUSSION: Pain affects both the physical and psychological wellbeing of patients and should not be
treated with pharmacotherapy alone. The model of WHO analgesic ladder provides guidelines for choosing the analgesic agents, but has its limitations. Incorporating the latest paradigm of neuromatrix theory,
both acute and chronic pain should be best managed with a broader perspective incorporating multimodal non-pharmacological and supportive treatments, illustrated by the concept of interacting domains
on a broad platform as presented in this article. Different levels of pain severity and chronicity necessitate
different analgesic platforms of management, and the clinician should move up or down the appropriate
platform to explore the various treatment options as per the status and needs of the patient.
KEYWORDS: Analgesic ladder; pain management; analgesic platform
The original WHO analgesic ladder
J PRIM HEALTH CARE
2012;4(3):254–258.
CORRESPONDENCE TO:
Lawrence Leung
Department of Family
Medicine, Queen’s
University, PO Bag
8888, Kingston ON
K7L 5E9, Canada
leungl@queensu.ca
254
In 1986, the World Health Organization (WHO)
published a set of guidelines regarding the use of
analgesics in treating cancer pain.1 It described a
three-step approach of sequential use of pharmacological agents commensurate with the pain
level as reported by the patient. This stepwise
concept with practical recommendations eponymously became the analgesic ladder which was
later translated into 22 languages and became one
of the most adopted standards for general pain
therapy in the next three decades (see Figure 1).2
Moving up from no treatment, the original ladder model starts with non-opioids (e.g. aspirin,
paracetamol or nonsteroidal anti-inflammatory
drugs, NSAIDs) for mild pain, then increasing
to weak opioids like codeine and its derivatives
as the second step for intermediate level of pain,
and finally escalating to strong opioids like morphine, methadone and even fentanyl as the third
step for the highest level of pain (Figure 1).
Apart from the choice of pharmacological agents,
the original analgesic ladder states that:3
• assessment of the patient is necessary prior to
initiation and at regular intervals of therapy
• oral form of analgesics is preferred wherever
possible
• analgesic should be given at regular intervals
rather than on demand
• there is no standardised dosage and therapy
should be individualised according to the level
of pain as perceived
• the central aim is to relieve as much pain as
possible
• adjuvant treatment should be added where
necessary.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
VIEWPOINT
Advantages of the analgesic ladder
The original ladder was put forward to address
the prevalent obstacles of effective cancer pain
relief at that time, which included inadequate
training amongst carers in cancer pain management, overt fear of addiction, poor drug availability and lack of public awareness. It both
legitimises and rationalises the use of opioids in
a cost-effective way for cancer pain. Two years
after launching, the analgesic ladder was already
validated to be useful in 80–90% of cases.4 The
guidelines were further revised in 1997 and their
efficacies have stood the test of time. Because of
its step-by-step concept, the ladder approach is
extended to management of acute and chronic
pain, and modified in various specialties.
Controversies and limitations
of the WHO ladder
Right from the start
We may take for granted that NSAIDs are the
bedside norm for mild acute pain, the evidence
for standalone use in mild chronic and cancer
pain is still inconclusive. Studies, however, have
shown additional benefits of NSAIDs when used
in combination with opioids for moderate to
severe pain.5–7 North American physicians are less
enthusiastic in general than their European colleagues in prescribing long-term NSAIDs for fear
of gastrointestinal and renal complications.8
Thus said, in managing chronic pain, it would not
be advisable to proceed to fentanyl patches too
soon without properly titrating the actual opioid
requirement. In fact, for cancer-type pain with
breakthrough phenomena, fentanyl patches may
not be a suitable choice due to their 72-hour longacting nature and relative lack of dose gradation.
Taboo of switching agents or using more
than two agents in the same rung
The original ladder advises against using two or
more agents of the same rung simultaneously.3
Nowadays, this advice is seldom adhered to. In
managing mild acute pain, it is not unusual to
prescribe both paracetamol and NSAIDs in step 1
of the ladder. For moderate to severe chronic
and cancer pain, it is now standard practice to
give a long-acting opioid for basal control of
pain plus a short-acting opioid for breakthrough
pain.14 In managing rheumatological pain, it is
Figure 1. The original WHO analgesic ladder
The value of the second step
The role of weak opioids (e.g. codeine, dihydrocodeine, dextroproxyphene and tramadol) as the
second step is also intensely debated. Two studies
have shown better pain control with these step 2
agents as compared to morphine.9,10 One randomised controlled trial favoured using strong
(step 3) opioids as initial agents for cancer pain
and question the need of weak opioids;11 however,
the validity of this was confounded by the use
of a number of opioids at varying doses and 50%
controls do not have matching levels of pain. Two
other studies using transdermal fentanyl patches
(step 3 opioid) demonstrated that 25µg/hr patches
produce good pain relief in opioid-naive patients
with chronic pain, omitting the need for step 2 of
the WHO ladder.12,13
This shows the stepwise recommendation of pharmacotherapy
from non-opioids (e.g. acetaminophen, aspirin, NSAIDs), weak
opioids (e.g. codeine, hydrocodone, tramadol) to strong opioids
(morphine, hydromorphone, fentanyl)
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE255
VIEWPOINT
analgesics are poised in an interactive way. These
domains include:
Figure 2. The concept of the neuromatrix theory for pain
Itself visualised as an entity (like an incessant spinning sphere) comprising the somatosensory (S),
cognitive (C) and affective (A) domains, it receives inputs from areas of the brain governing sensation,
emotions and cognitions and, in return, churns out a neurosignature (output) which activates various
programmes for pain recognition, motor response, emotional and stress reactions. (Adapted from
Melzack, Evolution of the neuromatrix theory of pain. The Prithvi Raj Lecture: presented at the third
World Congress of World Institute of Pain, Barcelona 2004. Pain Pract. 2005 Jun;5(2):85–94.)
often necessary to try two or three NSAIDs and
even use them in combination, as failure of one
agent does not predict inefficacy of another.15
Similarly, switching between different types and
deliverable forms of potent opioids (step 3 of the
analgesic ladder) in cancer pain is now commonly
practised to achieve better outcomes and lesser
toxicity.16
From rungs to platforms:
time to think broad
Pain in human beings, whether acute or chronic,
has both physical and psychological components.
Theories of pain have also moved from the
original linear concept of gate-control17 to the
latest three-dimensional neuromatrix system,18
incorporating the emotional and cognitive
domains with the processing of pain signals in
the central nervous system (see Figure 2). In the
same line of thought, management of pain should
no longer be a linear direction going up or down
the narrow rungs of a ladder. Rather, it should
be conceptualised as various levels of analgesic
platforms extending horizontally from the rungs
of the analgesic ladder, on which other domains
to alleviate pain in addition to the recommended
256
• adjuvant pharmacological agents like muscle relaxants (e.g. cyclobenzaprine, baclofen
and dantrolene), anticonvulsants (e.g.
gabapentin, pregabalin and lamotrigine),
antidepressants (e.g. tricyclics, SSRI, SNRI),
injectable agents (steroids, local anaesthetics), compounds that act synergistically
with opioids like cannabinoids (nabilone)
• physiotherapy and physical therapy
• surgical and neurosurgical procedures (e.g. spinal cord stimulation, deep brain stimulation,
spinal delivery of opioids, ganglion ablation by
phenol or electrofrequency, sympathectomy)
• cognitive behavioural therapy and psychological counselling
• interpersonal reinforcement (e.g. support
group)
• mind–body integration (e.g. yoga, meditation
and religious support)
• hypnosis and relaxation therapy
• acupuncture and chiropractic
• other complementary and alternative medicine
(CAM) options.
Each of these domains can be present in every
platform and should be considered as an adjunct
where appropriate. Depending on the chronicity
and severity of the pain and physical/psycho­
social construct of the patient, the clinician
moves up or down the platforms in time enlisting
different domains (Figure 3), similar to the traditional WHO analgesic ladder which stipulates
different choice of pharmacological agents. However, unlike the traditional ladder which needs
frequent modifications, either with extra rungs2,19
for cancer or severe types of pain, or fast-tracking2 in cases of acute pain, this novel concept of
analgesic platform model is universally applicable
to all pain scenarios, capable of describing the
dynamics of pain management in a broader and
holistic manner.
Relevance in general practice
This platform modification of the original WHO
analgesic ladder extends the concept of pain
management from an up–down linear pharmacological adjustment to a broader three-dimensional
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
VIEWPOINT
Figure 3. Change of concept from the analgesic ladder to the analgesic platform
A—Physiotherapy and physical therapy | B—Mind–body integration (e.g. yoga, meditation and religious support) | C—Hypnosis and relaxation therapy |
D—Acupuncture | E—Chiropractic | F—External rub/lotions | G—Other CAM options (Tai chi, Tui Na) | H—Muscle relaxants (e.g. cyclobenzaprine, baclofen
and dantrolene) | I—Injectable agents (steroids, local anaesthetics) | J—Interpersonal reinforcement (e.g. support group) | K—Anticonvulsants (e.g. gabapentin,
pregabalin and lamotrigine) | L—Antidepressants (e.g. tricyclics, SSRI, SNRI) | M—Compounds that act synergistically with opioids like cannabinoids (nabilone) |
N—Cognitive behaviour therapy and psychological counselling | O—Surgical and neurosurgical procedures (e.g. spinal cord stimulation, deep brain stimulation, spinal
delivery of opioids, ganglion ablation by phenol or electrofrequency, sympathectomy)
perspective that encompasses other domains and
disciplines of therapies. Adopting this novel
analgesic platform concept will not only remind
practising clinicians to think and act broadly in
seeking solutions, it will also align the treatment
goals with the modern neuromatrix theory in
dealing with acute and chronic pain. In primary
care, the analgesic platform is of particular
relevance as patients with pain often present to
their primary care providers with psychosocial
overlays that are best approached and managed
with a broad and multimodal horizon.
Case study 1
A 56-year-old retired manual labourer with four
years’ history of chronic back pain as a result of
traumatic herniation of L5/S1 disc. He underwent
discectomy which gave him little improvement,
and he experienced constant sharp pain in his
lower back which would often radiate down to
both of his thighs. Patient responded initially to
non-steroidal anti-inflammatory drugs, but soon
proceeded to codeine and hydrocodone. He tried
three courses of physiotherapy and noticed very
slight benefits. He was given amitriptyline but developed dizziness. As you reviewed his file, a pain
specialist recommended that the patient should be
moved up the analgesic ladder for stronger choices
like morphine or hydro­morphone. On examination, patient seemed distressed and tired. Further
questioning revealed recent stress in the patient’s
family with on­going financial difficulties. Patient
also admitted having poor quality of sleep and
depressed mood, albeit lack of suicidal ideation.
You realised that there were coexisting psychosocial issues in the patient’s life that could perpetuate and, in fact, exacerbate the chronic pain
conditions. Hence, you decide to think broad and
adopt the analgesic platform, adding in duloxetine
30mg which would help both of his mood and
neuropathic pain and a muscle relaxant to relieve
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE257
VIEWPOINT
the muscle spasm. You also suggested a meditation class and structured stretching exercises for
his back. Last but not least, you enrolled him
for a support group for chronic pain counselling.
Patient made steady improvement in the next six
months, gradually stepping down to non-opioid
platform (NSAIDs) with the addition of a lowdose pregabalin.
Case study 2
A 35-year-old professional footballer came to
consult about pain in his right knee. A previous
injury of that knee had involved partially torn
cruciate ligaments. After successful repair, he
still felt dull pain and stiffness in the knee at
times. He consciously stayed away from any opioid containing analgesia for fear of affecting his
professional career. He used up to 3 g of paracetamol plus 1.8 g of ibuprofen and reported the pain
as 5/10. You reviewed his musculoskeletal pain
and realised that moving up to opioid analgesia is
not an option; hence, you went horizontally along
the analgesic platform and suggested a combination of physiotherapy, muscle relaxants, massage therapy and acupuncture. In three months,
patient went back to his football games with a
manageable pain level of 2/10.
Case study 3
ACKNOWLEDGEMENTS
Diagrams by Arthur Leung.
COMPETING INTERESTS
None declared.
258
A 65-year-old gentleman suffered from intractable pain due to disseminated carcinomatosis and
nerve root compression from metastatic vertebral
collapse. He took continuous-release hydromorphone 60 mg twice a day and short acting
hydromorphone 8 mg tablets up to six times a
day for breakthrough pain. He consulted you for
better pain control as part of his palliative care.
In view of the high demand of narcotics and
the need for constant titration, you discarded
the option of fentanyl patch even though it is
indicated at the highest rung of the traditional
WHO analgesic ladder. Instead you adopted the
analgesic platform concept and enlisted the help
of neurosurgeon and palliative care physicians,
who arranged for the patient to have continuous
intrathecal morphine pump. Patient experienced
remarkable pain relief and significant improvement in his mood in the following three months
until he died.
References
1. Ventafridda V, Saita L, Ripamonti C, De Conno F. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React.
1985;7(1):93–6.
2. Vargas-Schaffer G. Is the WHO analgesic ladder still valid?
Twenty-four years of experience. Can Fam Physician.
2010;56(6):514–7, e202–5.
3. Ventafridda V, Tamburini M, Caraceni A, De Conno F, Naldi F.
A validation study of the WHO method for cancer pain relief.
Cancer. 1987;59(4):850–6.
4. Stjernsward J. WHO cancer pain relief programme. Cancer
Surv. 1988;7(1):195–208.
5. Mercadante S, Fulfaro F, Casuccio A. A randomised controlled
study on the use of anti-inflammatory drugs in patients
with cancer pain on morphine therapy: effects on doseescalation and a pharmacoeconomic analysis. Eur J Cancer.
2002;38(10):1358–63.
6. Dhillon S. Tramadol/paracetamol fixed-dose combination: a
review of its use in the management of moderate to severe
pain. Clin Drug Investig. 2010;30(10):711–38.
7. Gatti A, Sabato E, Di Paolo AR, Mammucari M, Sabato AF.
Oxycodone/paracetamol: a low-dose synergic combination
useful in different types of pain. Clin Drug Investig. 2010;30
Suppl 2:3–14.
8. Mercadante S. Management of cancer pain. Intern Emerg
Med. 2010;5 Suppl 1:S31–5.
9. Grond S, Radbruch L, Meuser T, Loick G, Sabatowski R,
Lehmann KA. High-dose tramadol in comparison to low-dose
morphine for cancer pain relief. J Pain Symptom Manage.
1999;18(3):174–9.
10. Mercadante S, Salvaggio L, Dardanoni G, Agnello A, Garofalo S. Dextropropoxyphene versus morphine in opioidnaive cancer patients with pain. J Pain Symptom Manage.
1998;15(2):76–81.
11. Marinangeli F, Ciccozzi A, Leonardis M, Aloisio L, Mazzei
A, Paladini A, et al. Use of strong opioids in advanced
cancer pain: a randomized trial. J Pain Symptom Manage.
2004;27(5):409–16.
12. Mystakidou K, Tsilika E, Parpa E, Kouloulias V, Kouvaris I,
Georgaki S, et al. Long-term cancer pain management in morphine pre-treated and opioid naive patients with transdermal
fentanyl. Int J Cancer. 2003;107(3):486–92.
13. Vielvoye-Kerkmeer AP, Mattern C, Uitendaal MP. Transdermal
fentanyl in opioid-naive cancer pain patients: an open trial
using transdermal fentanyl for the treatment of chronic cancer
pain in opioid-naive patients and a group using codeine. J Pain
Symptom Manage. 2000;19(3):185–92.
14. Davis MP, Walsh D, Lagman R, LeGrand SB. Controversies
in pharmacotherapy of pain management. Lancet Oncol.
2005;6(9):696–704.
15. Bannwarth B. Irrelevance of the WHO analgesic ladder for
managing rheumatic pain. Joint Bone Spine. 2010;77(1):1–3.
16. Vadalouca A, Moka E, Argyra E, Sikioti P, Siafaka I. Opioid
rotation in patients with cancer: a review of the current literature. J Opioid Manag. 2008;4(4):213–50.
17. Melzack R, Wall PD. Pain mechanisms: a new theory. Science.
1965;150(699):971–9.
18. Melzack R. Evolution of the neuromatrix theory of pain. The
Prithvi Raj Lecture: presented at the third World Congress
of World Institute of Pain, Barcelona 2004. Pain Pract.
2005;5(2):85–94.
19. Tay W, Ho KY. The role of interventional therapies in
cancer pain management. Ann Acad Med Singapore.
2009;38(11):989–97.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
VIEWPOINT
Frequently asked questions on measurement
of bone mineral densitometry
Joseph C Lee MBBS, FRACP;1,2 Nelson K Loh BMedSci, MBBS, FRACP3
Introduction
What is the accuracy?
Osteoporosis currently afflicts over half of
women and almost 30% of men aged over 60
years; this figure will grow as the population
ages. Fractures—especially of the hip—result
in considerable social and economic costs to the
individual and to society, as well as leading to an
appreciable mortality.
The precision of DXA is approximately 1.0–1.5%
for spine and total hip BMD.1 DXA scanners
have excellent long-term precision because their
calibration is very stable and there are effective
instrument quality control procedures (provided
by the manufacturers) to detect any long-term
drifts. The test–retest variation for spine and hip
DXA is 2–3%, resulting in T-score accuracy errors
of ± 0.5.2
Bone mineral density measured with dual-energy
x-ray absorptiometry is the ‘gatekeeper’ to osteoporosis treatments in New Zealand and the best
way to estimate future fracture risk. Hence it is
important to be familiar with some of the technical aspects of densitometry and its application in
the community. Clarification of some of these
areas may facilitate more effective utilisation.
What are the indications for bone
mineral density (BMD) assessment?
The indications for BMD testing, as recommended on the Osteoporosis New Zealand website
(http://www.bones.org.nz), are listed in Table 1.
As pointed out on the site, BMD should only be
measured if it will impact management.
Department of Nuclear
Medicine, The Prince Charles
Hospital, Queensland,
Australia
1
School of Medicine,
University of Queensland,
Queensland, Australia
2
Department of Nuclear
Medicine, Sir Charles
Gairdner Hospital, Western
Australia, Australia
3
What is the radiation dose?
The effective radiation dose is 1–10 µSv.3 Context
is provided in Table 2.
Are spine or hip measurements better?
The best way of predicting fracture risk at any
given site is to measure BMD at that site—for example, DXA of the proximal femur predicts femoral fracture better than measurements at other
sites.4 Similarly, for vertebral or wrist fractures.
The spine is the best site for follow-up measurements because treatment changes are usually the
Table 1. Indications for bone densitometry
Women over 60 years and men over 70 years with risk factors such as:
Glucocorticoid therapy
Parental history of a hip fracture
Low body weight (< 58 kg) or body mass index (< 20 kg/m²)
History of smoking or heavy alcohol intake
Premature menopause in women or hypogonadism in males
Rheumatoid arthritis
Malabsorption, chronic liver or renal disease
Any woman over 65 years or man over 75 years considering specific measures to prevent osteoporosis
Any individual prescribed long-term glucocorticoids or other medications associated with osteoporosis, e.g. anticonvulsants, aromatase inhibitors
Women with a history of premature menopause
Postmenopausal women or older men with a history of minimal trauma fracture
(from Osteoporosis New Zealand—www.bones.org.nz)
J PRIM HEALTH CARE
2012;4(3):259–261.
CORRESPONDENCE TO:
Joseph C Lee
Staff Specialist Consultant
Physician, Department of
Nuclear Medicine, The
Prince Charles Hospital,
Queensland, Australia
Joseph_Lee@health.
qld.gov.au
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE259
VIEWPOINT
Table 2. Effective radiation dose of DXA compared to urban background and other
medical procedures3
Table 3. Clinical risk factors included in FRAX algorithm—
www.shef.ac.uk/frax
DXA
1-10 μSv
Country of geographic origin
Chest x-ray
30 μSv
Ethnic origin
Mammogram
130 μSv
Age
Annual background (urban environment)
2000 μSv
Sex
CT pelvis
5000 μSv
Weight
Height
largest at this site and the precision error is lower
than at other sites.5,6
Parental history of hip fracture
Current smoking status
Corticosteroid therapy (current or past)
How do the fracture risk
calculators compare?
Rheumatoid arthritis
The WHO Fracture Risk Assessment Tool
(FRAX) algorithm (available at http://www.shef.
ac.uk/frax) accounts for 14 risk factors (as listed
in Table 3) in calculating 10-year probabilities of
hip and major osteoporotic (humerus, forearm,
hip or clinical vertebral) fractures.7 It incorporates
data from 12 independent fracture studies, over
60 000 men and women (from four continents)
Table 4. Pharmac Special Authority for subsidy criteria for alendronate10
One significant osteoporotic fracture demonstrated radiologically and T-score ≤ -2.5
One significant osteoporotic fracture demonstrated radiologically, and either the
patient is elderly, or densitometry scanning cannot be performed because of major
logistical, technical or pathophysiological reasons
Two significant osteoporotic fractures demonstrated radiologically
T-score ≤ -3.0
Ten-year risk of hip fracture (according to FRAX or Garvan calculator) ≥ 3%
Patient has had a Special Authority approval for zoledronic acid (underlying cause—
osteoporosis) or raloxifene
The patient is receiving systemic glucocorticosteriod therapy (≥ 5 mg per day
prednisone equivalents) and has already received or is expected to receive therapy for
at least three months; and
• T-score ≤ -1.5; or
• one significant osteoporotic fracture demonstrated radiologically; or
• Special Authority approval for zoledronic acid (underlying cause—
glucocorticosteroid therapy) or raloxifene
Table 5. Recommended intervals for serial DXA for detecting development of
osteoporosis14
Normal BMD or ‘mild osteopenia’ (T-score not less than -1.5)
15 years
‘Moderate osteopenia’ (T-score between -1.5 and -2.0)
5 years
‘Advanced osteopenia’ (T- score between -2.0 and -2.5)
1 year
260
Previous history of fracture (after age 50)
Secondary osteoporosis
Alcohol intake (≥3 units daily)
Hip BMD
and 250 000 person-years of follow-up.8 The
Garvan Institute fracture risk calculator (http://
garvan.org.au/promotions/bone-fracture-risk/calculator) requires fewer data and emphasises past
fractures and falls.
A recent study found that the Garvan Institute
calculator overestimated hip fracture rates and
FRAX (with BMD measurements) underestimated osteoporotic and hip fracture rates.9 However,
BMD should continue to be used to calculate
fracture risk which informs treatment decisions.
How can BMD results be
used to plan treatment?
BMD and/or fracture risk scores are used as the
arbiters for osteoporosis treatment as treatment is
considered cost-effective at certain thresholds of
fracture risk. For example, Special Authority for
Subsidy is granted under the Pharmac schedule10
for alendronate according to the criteria in Table 4. By comparison, the threshold for treatment
is set at a hip fracture risk in the next 10 years of
4% in the United Kingdom and Sweden.11
Why are there discrepancies
between hip and spine T-scores?
A number of factors can spuriously affect the
T- (and Z-) score at the hip and spine, including
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
VIEWPOINT
degenerative bone/joint disease and aortic calcification which leads to spuriously high BMD measurements.12 However, some conditions do tend to
preferentially affect BMD at the spine more than
the hip (e.g. steroid use) or the hip over the spine
(e.g. hyperparathyroidism).
How often should DXA be repeated?
The International Society of Clinical Densitometry (ISCD) currently recommends no more
frequent than biennial re-testing,13 formulated
from the known precision of DXA equipment
and that the normal rate of postmenopausal bone
loss is 1–2% per year.
Prospective clinical study of postmenopausal
women concluded that development of osteoporosis is adequately detected by DXA frequency
stratified by previous DXA findings for that
individual14 (summarised in Table 5). In most
instances, this is much less frequent than the
minimum two-year interval recommended by
ISCD. However, it is also suggested that patients
with advanced osteopenia should have repeat
testing in one year, which directly contradicts the
ISCD’s recommendation.
Are DXA results from different
facilities interchangable?
No. Different facilities use different equipment
made by different manufacturers which, in turn,
utilise different reference databases. It is best,
therefore, to use the same software for repeat
scans wherever possible.
SUMMARY
• DXA is a fast, reliable, low-radiation method for assessing BMD, which is the arbiter for osteoporosis treatment eligibility and the best determinant of future fracture risk.
• Web-based fracture risk calculators can utilise BMD data to provide further information for medical practitioners and patients.
• The interval for serial BMD assessment for detecting development of
osteoporosis should be planned according to the previous DXA findings.
7. Kanis JA, Oden A, Johnell O, et al. The use of clinical risk
factors enhances the performance of BMD in the prediction
of osteoporotic fractures in men and women. Osteoporos Int.
2007;18:1033–46.
8. Blake GM, Fogelman I. An update on dual-energy x-ray
absorptiometry. Semin Nucl Med 2010;40:62–73.
9. Bolland MJ, Siu AT, Mason BH, et al. Evaluation of the FRAX
and Garvan fracture risk calculators in older women. J Bone
Miner Res. 2011;26:420–7.
10. Wilson K, Bloor R, Jennings D, editors. TEX Schedule February 2012 Volume 19. New Zealand: Pharmaceutical Management Agency; 2012.
11. Chun KJ. Bone densitometry. Semin Nucl Med. 2011;41:220–8.
12. Reid IR, Evans MC, Ames R, et al. The influence of osteophytes and aortic calcification on spinal mineral density in postmenopausal women. J Clin Endocrinol Metab.
1991;72:1372–4.
13. Baim S, Binkley N, Bilezikian JP, et al. Official positions of the
International Society for Clinical Densitometry and executive
summary of the 2007 ISCD Position Development Conference. J Clin Densitom. 2008;11:75–91.
14. Gourlay ML, Fine JP, Preisser JS, et al. Bone-density testing
interval and transition to osteoporosis in older women. New
Engl J Med. 2012;366:225–33.
References
1. Patel R, Blake GM, Rymer J, et al. Long-term precision of DXA
scanning assessed over seven years in forty post-menopausal
women. Osteoporos Int. 200;11:68–75.
2. Blake GM, Fogelman I. How important are BMD accuracy errors for the clinical interpretation of DXA scans? J Bone Miner
Res. 2008;23:457–62.
3. Fogelman I, Blake GM. Different approaches to bone densitometry. J Nucl Med. 2000;41:2015–25.
4. Marshall D, Johnell O, Wedel H. Meta-analysis of how well
measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ. 1996;312:1254–9.
5. Blake GM, Herd RJ, Fogelman I. A longitudinal study of
supine lateral DXA of the lumbar spine: a comparison with
posteroanterior spine, hip and total-body DXA. Osteoporos
Int. 1996;6:462–70.
6. Faulkner KG. Bone densitometry: choosing the proper site to
measure. J Clin Densitom. 1998;1:279–85.
COMPETING INTERESTS
None declared.
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE261
LETTERS TO THE EDITOR
Malaysian GAD-7 less sensitive than reported
I
n their paper on the validation of the Malay version of the
GAD-7, Sidik et al. reported acceptable sensitivity (76.3%) and
excellent specificity (94.4%) for detecting anxiety disorder in
consecutive women attending a primary care clinic.1 However,
these results are biased because the authors failed to account
for the stratified sampling procedure. When a stratified sampling procedure has been applied, the data must be ‘weighted
back’ to mirror the source population in order to produce
unbiased estimates of the operating characteristics for that
population. Sidik et al. included 895 women who completed a
PHQ-9 and GAD-7. Then they divided the group into women
with normal scores (PHQ-9 <10 and GAD-7 <5) and women
with high scores (PHQ-9 ≥10 and GAD-7 ≥5). From the first
group, one in 10 women and from the second group one in two
women were selected for a psychiatric diagnostic interview.
Fifty participants were excluded, leaving 845 overall participants of whom 146 underwent a diagnostic interview. Sidik
et al.’s Table 1 informs us that 38 of the latter 146 women had
an anxiety disorder diagnosis and 35 of the 146 women had a
positive GAD-7 test (≥8). In addition, Sidik et al. provided the
information that 66 of the original 845 women (i.e. 7.8%) had a
positive GAD-7 test. We can use this information to try to calculate the expected numbers for Table 1 when all 845 women
(representing the source population of women attending the
clinic) would have been examined instead of the stratified
sample of 146: From a total of 845 women, 66 had a positive
and 779 a negative GAD-7. Thus, the 35 women with a positive
GAD-7 (from the 146 women examined) represented a sample
of the original 66 women with a positive GAD-7. To weight
back these women to the source population, they are assigned
a weight factor of 66/35=1.9. The 29 women with a positive
GAD-7 and an anxiety disorder diagnosis therefore probably
represented 29 x 1.9 = 55 women in the source population.
Similarly, the six women with a positive GAD-7 and no anxiety disorder diagnosis probably represented 6 x 1.9 = 11 women
in the source population. Analogously, the weight factor for
women with a negative GAD-7 is 779/111 = 7.0. The nine
women with a negative GAD-7 and an anxiety disorder diagnosis probably represented 9 x 7.0 = 63 women in the source
population (!). A complete redraw of Table 1 looks like this:
Table 1. Numbers weighted back to mirror the source population
Anxiety
diagnosis
No anxiety
diagnosis
Total
GAD-7 positive
55
11
66
GAD-7 negative
63
716
779
Total
118
727
845
Sensitivity of the GAD-7 in the source population was 55/118
= 46.6% (instead of 76.3% in the stratified sample). Specificity
was 98.5%, the LR of a positive test was 30.81 and the LR of a
negative test was 0.54%. The revised conclusion should be that
the GAD-7 did not perform very well in detecting anxiety disorder in the Malaysian women attending a primary care clinic:
the GAD-7 missed more than half of all anxiety disorders.
Berend Terluin, MD, PhD
Dpt. of General Practice and Elderly Care Medicine,
EMGO Institute for Health and Care Research,
VU University Medical Centre, Amsterdam, Netherlands
Reference
1. Sidik S, Arroll B, Goodyear-Smith F. Validation of the GAD-7 (Malay version)
among women attending a primary care clinic in Malaysia. J Prim Health Care.
2012;4(1):5–11.
Authors’ response
In response to the ‘Letter to the Editor’ on the validity results of the GAD-7 (Malay version), the authors would like to maintain that their original calculations are correct. The validity of the GAD-7 (Malay version) was calculated based on the 146 participants interviewed with the CIDI, and not the
whole study population (n=845). The objective of the paper was to validate the GAD-7 against the CIDI as the reference standard, which was stated
in the abstract and method sections. Therefore, the authors are justified in calculating the sensitivity and specificity of the GAD-7 only among the
146 participants who were interviewed with the CIDI. The remaining 699 respondents were not interviewed with the CIDI, and therefore the validity
findings were not generalised to the whole study population of 845. The sensitivity and specificity of a test are independent of the prevalence of a
disorder. We accept that the likelihood ratios are based on small numbers but they are also independent of prevalence. Dr Terluin’s extrapolation of
results from a subset onto the total population, including those who had not had the reference standard risks, must be interpreted with caution due to
the potential magnification of error, where numbers in some groups are actually small.
Letters may respond to published papers, briefly report original research or case reports, or raise matters of interest relevant to
primary health care. The best letters are succinct and stimulating. Letters of no more than 400 words may be emailed to:
editor@rnzcgp.org.nz. All letters are subject to editing and may be shortened.
262
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE
FILM REVIEW
A good death: a film about end-of-life care and
advance care planning
Produced by Prof. D Robin Taylor and Paul Trotman
Reviewed by Prof. Rod MacLeod PhD, FRCGP, FAChPM; Senior Staff Specialist in Palliative Care, Hammond
Care, Sydney, and Conjoint Professor in Palliative Care, University of Sydney, Australia
‘A wise physician will consider whether a disease be incurable: if he find it to be such,
let him resort to palliation: and alleviate the symptom.’ Bacon, Sylva, 1626
T
he modern palliative care movement has
been around for over 40 years and yet
many health practitioners still find it hard
to provide appropriate management near the end
of life. This film is made for people with COPD
or serious lung conditions, their families and the
doctors and nurses who provide care for them.
One of the aims is to introduce the concept of
advance care planning and to prompt discussion
about patient choices, but the real power of the
film is in telling the story of the final illness of
Martin Cavanagh as he is accompanied by his
wife Tui and their family towards the end of his
life. Robin Taylor writes on the website that they
‘wanted to make this film because we realised
that the care we were providing to patients with
respiratory disease at the end of life was missing
the mark.’ On the evidence provided in this film
they have little to be worried about. The care
captured on film is exemplary. Professor Taylor
is shown as empathetic, forthright and honest
in his approach to Martin, the patient, Martin’s
wife Tui and to the audience of the film. The
most striking person on film, however, is Martin himself, who displays dignity and control
throughout.
One of the sadnesses pointed out by Professor
Taylor is that doctors generally ‘do what they are
trained to do.’ Sadly, we know that the training
provided to young doctors and nurses in end-oflife care is inadequate in many ways. By making
this film, the producers have shown that there is
power in the telling of stories; there is power in
excellent camera work (here by Scott Mouat), and
there is power in watching and listening in order
to learn. It is well worth listening and watching
more than once as there are so many snippets of
wisdom contained in the spoken words.
There are weak points. Some of the dialogue is
hard to hear (especially through Martin’s oxygen
mask), but overall the quality of the film-making
is very high. The website provides useful web
addresses for further information.
This is an important piece of work that should
be shown to every New Zealand medical
student and as many medical specialists and
primary physicians as possible. It is an honest
way of indicating the importance of advance
care planning and a way of showing that it is
possible to have a good death from a chronic
disabling disease. I recommend it highly.
PRN Films, Dunedin, 2012
www.agooddeath.co.nz
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE263
ABOUT THE JOURNAL OF PRIMARY HEALTH CARE
T
he Journal of Primary Health Care
(JPHC) began publishing in 2009,
superseding the previous RNZCGP
journal the New Zealand Family Physician.
It is an interdisciplinary publication aimed
at moving research into primary health
care practice and practice into research.
This includes the fields of family practice,
primary health care nursing and community
pharmacy as well as areas such as health care
delivery, health promotion, epidemiology,
public health and medical sociology of
interest to a primary health care provider
audience. It is positioned as relevant to
countries within the Pacific rim.
JPHC publishes peer-reviewed quantitative
and qualitative original research, systematic
reviews, papers on improving performance
and short reports that are relevant to its
primary health care practitioners. For the aim,
scope, instructions to authors and templates
for publications see www.rnzcgp.org.nz/
journal-of-primary-health-care/.
JPHC includes pithy digests of the latest
evidence including a String of PEARLS
(Practical Evidence About Real Life
Situations), Potion or Poison? (evidence for
the potential benefits and possible harms
of well-known herbal medicines), Cochrane
Corner (the summary of a Cochrane review),
Nuggets of Knowledge (succinct synopses
of pharmaceutical evidence for primary
care), Pounamu and Vaikoloa, (Maori
and Pacific primary health care treasures
respectively) and Gems, 100-word outlines
of NZ primary care research published in
other journals.
JPHC publishes viewpoints, commentaries
and reflections that explore areas of
uncertainty on aspects of care for which
there is no one right answer. Debate is
stimulated in Back to Back, where two
professionals present their opposing views
on a topic. There is a regular Ethics column.
Letters to the Editor are welcomed.
INDEXING
The Journal is indexed in MEDLINE, Excerpta
Medica (EMBASE), Cumulative Index
to Nursing and Allied Health Literature
(CINAHL), Scopus and Index New Zealand
(INNZ). Complete text of the Journal is
available online at http://www.rnzcgp.org.
nz/journal-of-primary-health-care/ and
through various aggregators including
PubMed Central and EBSCO.
EDITOR
Prof. Felicity Goodyear-Smith: Professor and
Goodfellow Postgraduate Chair, Department
of General Practice and Primary Health Care,
The University of Auckland, Auckland, New
Zealand; editor@rnzcgp.org.nz
Dr Ofa Dewes: Research Fellow,
Department of Pacific Health, School of
Population Health, University of Auckland
Prof. Tony Dowell: Professor and Head
of the Department of Primary Health
Care and General Practice, Wellington
School of Medicine, University of
Otago, NZ
Ms Eileen McKinlay: Senior Lecturer in
Primary Health Care, Department of Primary
Health Care and General Practice, University
of Otago Wellington, NZ
Prof. Pauline Norris: Professor and Chair
in Social Pharmacy, School of Pharmacy,
University of Otago, Dunedin, NZ
EDITORIAL BOARD
The Editorial Board comprises renowned
and active primary care clinicians, clinical
and scientific academics and health policy
experts with both New Zealand and
international representation.
Dr Barry Parsonson: Psychologist for NZ
Ministry of Education and International
Consultant, UNICEF (Georgia) Training
Project for Institutional Staff working with
disabled children, Napier, NZ
Prof. Bruce Arroll: Professor and Head of the
Department of General Practice and Primary
Health Care, The University of Auckland,
Auckland, NZ
Dr Shane Reti (QSM): Interna­tional Program
Director Clinical Informatics and CEO of
Clinical Informatics Industrial Research,
Harvard Medical School, USA
Prof. Jenny Carryer: Professor of Nursing,
School of Health and Social Services, Massey
University, Palmerston North, NZ
Dr Jo Scott-Jones: General practitioner,
Opotiki, Eastern Bay of Plenty
Prof. Peter Crampton: Pro-Vice-Chancellor,
Division of Health Sciences, University of
Otago, Dunedin NZ
Prof. Kurt Stange: Professor of Family
Medicine, Case Western Reserve University,
Cleveland, OH, USA and Editor, Annals of
Family Medicine
SUBMISSIONS
Full instructions for authors can be found at:
http://www.rnzcgp.org.nz/information-for-authors
Please send all submissions to the Editor: editor@rnzcgp.org.nz
JPHC ADMINISTRATION
For subscription and advertising queries, or to sign up for email alerts, please contact the
Publications Coordinator, RNZCGP, PO Box 10440, Wellington 6143, New Zealand;
jphcnz@rnzcgp.org.nz
JPHC is printed on uncoated, acid-free paper which meets the archival requirements of ANSI/NISO Z39.48-1992 (Permanence of Paper) and is
Forest Stewardship Council (FSC)–certified which meets the highest environmentally responsible standards.
The Journal of Primary Health Care is the official journal of the RNZCGP. However, views expressed are not necessarily those of the
College, the Editor, or the Editorial Board. ©The Royal New Zealand College of General Practitioners 2012. All Rights Reserved.
264
VOLUME 4 • NUMBER 3 • SEPTEMBER 2012 J OURNAL OF PRIMARY HEALTH CARE