Vaccine 24S1 (2006) S1/16–S1/22
Immune responses to human papillomavirus
Margaret Stanley ∗
University of Cambridge, Department of Pathology, Tennis Court Road, Cambridge CB2 1QP, UK
Available online 19 September 2005
Abstract
The immune system uses innate and adaptive immunity to recognize and combat foreign agents that invade the body, but these methods
are sometimes ineffective against human papillomavirus (HPV). HPV has several mechanisms for avoiding the immune system. HPV infects,
and multiplies in keratinocytes, which are distant from immune centers and have a naturally short lifespan. The naturally short life cycle of the
keratinocyte circumvents the need for the virus to destroy the cell, which would trigger inflammation and immune response. In addition, HPV
downregulates the expression of interferon genes. Despite viral immune evasion, the immune system effectively repels most HPV infections,
and is associated with strong localized cell mediated immune responses. New prophylactic L1 virus-like protein vaccines for HPV 16 and 18
and HPV 6, 11, 16, and 18 are in phase 3 trials. Available data suggests that these vaccines are safe, produce high levels of antibodies, and
are effective at preventing HPV infection.
© 2005 Elsevier Ltd. All rights reserved.
Keywords: Immune responses; Human papillomavirus; Keratinocyte
1. Introduction to host immunity
The world is a dangerous place in which Homo sapiens
must continuously utilize sophisticated, flexible, and lethal
defenses to rebuff the massed regiments of viruses, bacteria, and eukaryotic parasites. Host defense is a partnership
between innate immunity (phagocytes, soluble proteins [e.g.,
cytokines, complement, and epithelial barriers]) and adaptive immunity (antibody, cytotoxic effector cells). The innate
immune system detects the pathogen and acts as the first line
of defense, clearing the majority of microbial assaults. Innate
immunity has no specific memory, but is responsible for activating adaptive immunity. The adaptive immune response
generates exquisitely specific lethal effector responses to foreign antigens as well as long-lived cells with memory of
the insult. Antibody-mediated humoral immunity clears free
virus particles from body fluids and can prevent viral reinfection, while cell-mediated immune responses are essential
for the clearance of virus-infected cells and the generation of
immune memory.
∗
Tel.: +44 1223 333736; fax: +44 1223 333346.
E-mail address: mas@mole.bio.cam.ac.uk.
0264-410X/$ – see front matter © 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.vaccine.2005.09.002
Innate immunity is activated by cell injury or cell death
and manifests as inflammation, the local vascular response
to injury. During inflammation, soluble and cellular innate
immune effectors are recruited. Local parenchymal cells
are recruited and local phagocytes are then activated to
secrete inflammatory cytokines and other defense molecules.
Crucially, dendritic cells, the only antigen-presenting cells
(APCs) that can activate naı̈ve T lymphocytes, are activated
to kick-start the adaptive immune response.
Innate immunity uses proteins encoded in the germ line
to identify potentially noxious elements. Adaptive immunity,
in contrast, is found only in vertebrates, is almost infinitely
flexible, and is based on T and B lymphocyte receptors generated by somatic gene rearrangement during ontogenesis.
Neither the specificity of these receptors nor the response
that might be induced in the lymphocytes after the ligation
of the receptor by antigen is predetermined; these responses
are determined by coordinated efforts between the innate and
adaptive immune systems. The innate immune response generates the signals that identify the nature of the antigen and the
appropriate type of effector response. For example, the germ
line-encoded receptors of the innate immune system recognize conserved molecular targets that are essential products of
microbial physiology and central to microbial survival. These
M. Stanley / Vaccine 24S1 (2006) S1/16–S1/22
S1/17
invariant products, known as pathogen-associated molecular
patterns, are molecular motifs shared by groups of pathogens.
The pathogen-associated molecular patterns are identified by
pattern recognition receptors such as the toll-like receptors of
the innate immune system, resulting in the activation of innate
immune effectors and induction of an appropriate adaptive
immune response [1].
T lymphocytes are the generals of the adaptive immune
system, playing central roles in both cell-mediated and
humoral immunity. T cells recognize antigen that has been
processed into short peptides, bound to the major histocompatibility complex (MHC) proteins, and presented as a
membrane-bound receptor complex on the cell surface. There
are two major subsets of T cells, identified by the surface
markers CD4 or CD8. CD4+ T cells recognize antigen presented by class II MHC; CD8+ T cells recognize antigen
presented by class I MHC. Class I MHC displays endogenous antigen, which is usually, but not always, derived from
intracellular synthesis of proteins broken down in the proteasome into short peptides and presented on the cell surface
as an MHC/peptide complex. Usually antigen plus class II
MHC is exogenous antigen taken up from the extracellular milieu and broken down in the endosome of the APC for
association into the class II complex. The interaction between
the T cell and the APC is very complex, since naı̈ve antigenspecific lymphocytes are difficult to activate by antigen alone.
Thus, several other receptor/ligand interactions must occur in
a regulated order before the T cell is activated and starts to
proliferate into armed effector T cells.
CD4+ T cell activation results in the secretion of a variety of small proteins, or cytokines, that help and regulate
other cells. The pattern of cytokine expression defines the
two major subsets of CD4+ T cells known as Th2 or Th1
cells.
the immediate vicinity. The released APC and cytokines are
the bridge between innate and adaptive immunity. The APC
“tells” the T cell what sort of defense is needed and is central
to both the generation of an effective and appropriate immune
response and the regulation of this response.
B lymphocytes develop in the bone marrow and emerge
as naı̈ve but mature cells that circulate in the blood and
lymph and lurk in the secondary lymphoid organs waiting
to encounter antigen. Each mature B cell bears a unique
membrane-bound B cell receptor, an immunoglobulin, or
antibody molecule that is specific for a discrete motif or epitope on an antigen. Once the naı̈ve B cell encounters antigen
and is activated, it undertakes a tightly regulated proliferation and differentiation program in which antigen-specific
memory B cells and effector plasma cells are generated. The
plasma cells secrete large amounts of antibodies, which are
soluble but otherwise identical versions of the membranebound B cell receptor. In the first encounter with antigen,
a primary antibody response is generated; later, a reencounter with the same antigen causes a more rapid secondary
response, producing high levels of antibodies with a high
binding affinity for the target antigen. It is this process that
is exploited in prophylactic vaccination.
Unlike T lymphocytes, B lymphocytes can recognize antigen in the natural conformation, but only a few native antigens
can directly activate B cells and generate plasma cells. In most
cases, antigen binding by the B cell receptor primes the B cell
that then requires cognate help from the Th2 cell in the form
of receptor-ligand interactions and cytokines to go through
the differentiation program. T cell help is crucial for class
switching, generating different antibody classes and isotypes,
and developing antigen-specific memory B cells [3].
• Th2 cells secrete IL-4 and IL-10 (and other cytokines)
and help antigen-primed B lymphocytes differentiate into
plasma cells and secrete antibodies, the effector molecules
of humoral responses.
• Th1 cells secrete IFN-␥ and create a milieu in which key
cytotoxic effectors—macrophages, natural killer cells, and
cytotoxic CD8+ T lymphocytes—are activated, generating
cell-mediated immunity.
2. Host defense to human papillomavirus (HPV)
infections
A third category of T cells, regulatory T cells (Tregs)
with the phenotype CD4+CD25+, expresses the signature
transcription factor Foxp3 and usually secretes IL-10 and
TGF-. Cells with this phenotype are thought to recognize
self-antigens and function to prevent autoimmunity; however, they also regulate responses to exogenous antigens, and
have been implicated in chronic and immunopathologic viral
infections [2].
The APC expresses receptors and secretes local cytokines
that dictate whether the T cell takes the Th2, Th1, or regulatory path. These functions of the APC are activated by
receptor-ligand interactions between APC and the pathogen,
and also by cytokines released by APC and other cells in
2.1. The infectious cycle
The papillomaviruses are ubiquitous infectious agents
that are characterized by strict species specificity and tissue
tropism. The infectious cycle of these viruses is tailored to the
differentiation program of the target cell. Different phases of
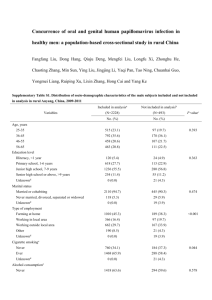
permissive viral growth accompany the maturation of the keratinocyte as it progresses up the epithelium to become a terminally differentiated squame (Fig. 1). Infection and vegetative
viral growth are absolutely dependent upon a complete program of keratinocyte differentiation. The virus infects primitive basal keratinocytes, probably targeting stem cells, but
only expresses high levels of viral proteins and viral assembly
in the upper layers of the stratum spinosum and granulosum
of the squamous epithelia [4–6]. Clinical evidence indicates
that viral gene expression is confined to the keratinocyte, or
cells with the potential for squamous maturation. The time
from infection to release of virus is approximately 3 weeks,
the time required for the basal keratinocyte to undergo com-
S1/18
M. Stanley / Vaccine 24S1 (2006) S1/16–S1/22
Fig. 1. The HPV infectious cycle. The virus infects a primitive basal keratinocyte (probably a stem cell) via microabrasion of the mucosal epithelium.
It is speculated that the immediate early events of virus growth involve an
amplification of virus copy number from 1–10 to 50–100 virus episomes/cell.
The next phase of virus growth is one of plasmid maintenance in which the
virus and cell replicate in tandem and there is no amplification of virus copy
number. This occurs in the proliferative compartment of the epithelium.
The infected keratinocyte then enters the differentiating compartment of the
epithelium, exiting the cell cycle. Virus gene expression is hugely upregulated with viral DNA amplification generating thousands of viral genomes.
Late viral proteins L1, L2, and E4 are made, and virus assembly occurs in
the superficial terminally differentiated squames.
plete differentiation and desquamation. The period between
infection and the appearance of lesions is highly variable and
can vary from weeks to months [7], suggesting that the virus
can effectively evade the immune system. There is no cytolysis or cytopathic death as a consequence of HPV replication,
assembly, or viral particle release because the keratinocyte is
a cell destined for death and desquamation, far from the sites
of immune surveillance. To permit virus replication, viral
proteins actually delay nuclear condensation in the differentiating keratinocytes forming the koilocyte. The virus-laden
keratinocyte then dies of “natural causes.” Thus, HPV infection is not accompanied by inflammation, and there is no obvious “danger signal” to alert the immune system to the virus’s
presence. This may result in persistent, chronic infection, as
the host can remain ignorant of the pathogen for long periods.
the endothelium of the wart capillaries [8]. This is characteristic of a Th1-based immune response, but it is important to
remember that cross-sectional studies provide only a snapshot of a dynamic process. Ethical and logistical issues inhibit
detailed longitudinal studies in humans, but in animal models of mucosal papillomavirus infection, such as the canine
oral papillomavirus, the immunologic events of the entire
wart cycle, from infection to regression, can be followed. In
these animal infections, wart regression is accompanied by
a cellular infiltrate similar to that seen in regressing genital warts. Systemic T cell responses directed towards HPV
early (E) proteins E2 and E6 peptides can be detected at low
frequency at distinct time points during the infectious cycle.
These responses occur in narrow time windows that coincide with periods of viral DNA amplification, are maximal
at wart regression, and decline quite rapidly thereafter (Jain
et al., 2003, personal communication). Furthermore, serum
levels of neutralizing antibody peak at wart regression [9].
Despite the low antibody titres induced by natural infection,
the animals remain resistant to challenge with large doses of
infectious virus for the rest of their lives.
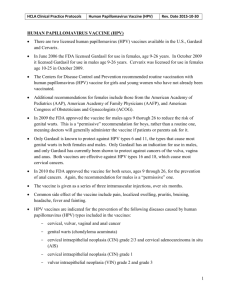
Epidemiologic and natural history studies strongly suggest
that the human immune response to HPV infection (Fig. 2)
follows a similar pattern [10,11]. Virtually all studies show
that genital HPV infection is extremely common in young
sexually active women, with prevalence as high as 80% in
certain adolescent populations [14]. Most of these HPV infections “clear,” i.e., DNA for a specific HPV type can no longer
be detected. The time required for clearance of the high-risk
HPV types, particularly HPV 16, averages 8–14 months, considerably longer than the 5–6 months needed for the low-risk
HPV types [12–14]. However, if the immune response fails
to clear or control the infection, then a persistent infection,
often with focally high levels of high-risk HPV DNA replication, is established. Persistently infected individuals have an
increased probability of progression to high-grade cervical
intraepithelial neoplasia and invasive carcinoma [10,15–18].
The increased incidence and progression of HPV infections in immunosuppressed individuals illustrates the critical importance of cell-mediated immune responses in the
resolution and control of HPV infections. Patients infected
2.2. Cell-mediated immunity
Clues to the nature of the cellular immune response to
HPV infection have come from immunohistologic studies of
spontaneously regressing genital warts. Nonregressing genital warts are characterized by a lack of immune cells at
the site of infection; the few intraepithelial lymphocytes are
CD8 cells, and mononuclear cells are present mainly in the
stroma. Histologic examination of regressing genital warts
reveals a large infiltrate of T cells (both CD4+ and CD8+)
and macrophages in the wart stroma and epithelium. The infiltrating lymphocytes express activation markers, the cytokine
milieu is dominated by proinflammatory cytokines such as
IL-12, TNF-␣, and IFN-␥, and there is upregulation of the
adhesion molecules required for lymphocyte trafficking on
Fig. 2. The natural course of genital HPV infection.
M. Stanley / Vaccine 24S1 (2006) S1/16–S1/22
S1/19
with human immunodeficiency virus (HIV) show multiple
recurrences of cervical intraepithelial neoplasia [19] and an
increased incidence of genital warts [20], the latter of which
appears to reflect an increased risk of progression from subclinical to clinical HPV infection [21]. Prospective studies
show prolonged persistence of HPV DNA in HIV-infected
13- to 18-year-old girls who are otherwise healthy [22], and
report high incidence rates of high-grade squamous intraepithelial lesions in this group [23]. The risk for incident highgrade squamous intraepithelial lesions in these HIV-infected
girls appeared to be due primarily to the persistence of lowgrade lesions, rather than to the persistence of high-risk HPV
DNA without a detectable lesion [23], implying that florid
viral gene expression in a persistent, active infection is important in disease progression.
2.3. Immune evasion mechanisms
Why the immune system ignores or fails to detect HPV
infection for so long is a central question. HPV infections
are exclusively intraepithelial and, theoretically, HPV attack
should be detected by the APC of squamous epithelia, the
Langerhans cell (LC). The activated LC should then migrate
to the draining lymph node, processing HPV antigens en
route, and present antigen to naı̈ve T cells in the node. The
T cells should then differentiate into armed effector cells,
migrate back to the infected site, and destroy the infected
keratinocytes (Fig. 3).
There are several reasons why this does not happen. The
infectious cycle of HPV is itself an immune evasion mechanism inhibiting host detection of virus. HPV replication and
release do not cause cell death, since the differentiating keratinocyte is already programmed to die, and this “death by
natural causes” does not present as a danger signal to the
immune system. Indeed, cell death that can generate danger
signals is a prerequisite for inflammation. Thus, for most of
the HPV infectious cycle, there is little or no release of the
proinflammatory cytokines important for dendritic cell activation and migration into the local milieu, and the essential
signals required for immune responses in squamous epithelia
are absent [24].
However, even in the absence of viral-induced cytolysis
and cell death, HPV-infected keratinocytes should activate
the powerful antiviral defense system, type 1 interferon secretion. The type 1 interferons, IFN-␣ and IFN-, have antiviral, antiproliferative, antiangiogenic, and immunostimulatory
properties, act as a bridge between innate and adaptive immunity, and activate immature dendritic cells [25,26]. Most DNA
viruses have evolved mechanisms for inhibiting IFN synthesis and signaling, and the papillomaviruses are no exception.
High-risk HPV viruses downregulate IFN-␣-inducible gene
expression [27,28], and the HPV 16 E6 and E7 oncoproteins
directly interact with components of the interferon signaling
pathways [29,30], abrogating these pathways. Capsid entry
is usually an activating signal for dendritic cells, but there
is evidence that LCs, unlike stromal dendritic cells, are not
Fig. 3. Antigen processing and presentation of viral antigen by Langerhans
cells (LCs). In the ideal scenario LCs take up viral antigen in the form of
virus particles plus viral proteins and nucleic acids released from infected
and dead keratinocytes. The LC pattern recognition receptors bind the viral
pathogen-associated molecular patterns and this, together with the binding of
proinflammatory cytokines, activates the LCs to move to the draining lymph
node. The activated LC matures during this migration, changing from an efficient antigen-processing cell to a highly effective antigen-presenting cell. In
the lymph node, antigen is presented to naı̈ve T cells that then migrate back
as armed effector T cells targeting the infected keratinocyte. In HPV infections, LC antigen presentation is delayed by HPV capsid direct inhibition of
LC activation, HPV downregulation of keratinocyte cytokine secretion, and
the absence of inflammation.
activated by uptake of HPV capsids [31,32], a phenomenon
that would inhibit both LC migration and maturation, and the
priming of the immune response against the capsid proteins.
In summary, the scenario that emerges from this is as follows: HPV efficiently evades the innate immune response
and delays the activation of the adaptive immune response.
The host dendritic cells are exposed to low levels of viral
proteins in a noninflammatory milieu for a protracted time
period and, as a result, local immune nonresponsiveness may
be established in the infected mucosa [33]. In this operationally HPV antigen-tolerant milieu, host defenses become
irrevocably compromised, and HPV antigen-specific effector cells are either not recruited to the infected area, or their
activity is downregulated, or both. Thus, if during a persistent
HPV infection there is deregulation of high-risk HPV E6 and
E7 with increased protein expression, and this does not result
in an armed effector cell-mediated immune response, HPVmediated progression to high-grade squamous intraepithelial
lesions and invasive carcinoma are unimpeded.
3. Immune intervention in HPV infections
Despite HPV’s ability to impede host defenses, a successful immune response to genital HPV infections is established
in most cases. This seems to be characterized by strong,
local, cell-mediated immunity that is associated with lesion
S1/20
M. Stanley / Vaccine 24S1 (2006) S1/16–S1/22
regression and the generation of serum neutralizing antibody.
Such antibody is generated in most, but not all, infected
individuals [34–36], and is directed against conformational
epitope(s) on the L1 protein displayed on the outer surface
of the intact virus particle. Serum neutralizing antibody levels following natural HPV infections, even at peak titers, are
low [37]. This probably reflects the exclusively intraepithelial infectious cycle (the absence of a viremia), as well as the
production of virus particles in the superficial epithelial cells,
distant from APCs and patrolling macrophages. These factors
limit antigen uptake, delivery to the lymph node, and presentation to naı̈ve B and T cells. Despite these low antibody
levels, seropositive animals are protected against further viral
challenge [38], and this protection can be transferred from
resistant to naı̈ve animals by passive transfer of serum [39].
This suggests that a vaccine that generates neutralizing
antibody to the major capsid protein L1 of genital HPVs
would be protective against infection. L1 protein must be
in the tertiary or native form and assembled as a multimer for
neutralizing antibody to be generated [40], a technically difficult objective. Production of L1 proteins has been achieved
by inserting the L1 gene into expression vectors, such as
recombinant baculoviruses for expression in insect cells, or
plasmids for expression yeast. In these cells, exogenously
expressed L1 proteins self-assemble into L1 virus-like particles (VLPs) [41,42]. The L1 VLP is a conformationally
correct, empty (containing no DNA) capsid that appears morphologically identical to, and contains the major neutralizing
epitopes of, the native HPV virion [43,44].
In experimental studies using the dog, cow, and rabbit,
immunization with L1 VLPs induced circulating neutralizing antibody to the L1 capsid protein, and the animals were
completely resistant to challenge with large amounts of virus
(for review, see [45]). This made L1 VLPs clear candidate
immunogens for prophylactic vaccinations in humans. Doseranging phase I studies in healthy subjects showed that doses
of 9–100 g HPV L1 VLPs given in three injections over 4–6
months were highly immunogenic, generating high titers of
anti-L1 antibody. All VLP-immunized subjects, but no subjects in the placebo arms, seroconverted and demonstrated
anti-VLP antibody responses that were substantially greater
than those identified following natural infections [46–49].
The dominant antibody responses induced by VLP vaccines
are of the IgG1 subclass and have been shown to be neutralizing by a variety of surrogate neutralization assays [46,50,51].
3.1. Type specificity and cross-protection
The neutralizing antibodies generated by HPV L1 VLP
vaccines appear to be type specific [52,53]. Thus, immunization with HPV 16 L1 VLPs would be expected to protect
against HPV 16 infection but not against any of the other
genital HPV types. The current generation of VLP vaccines
contains only two of the high-risk HPV types, HPV 16 and 18.
HPV 16 accounts for 50–60%, and HPV 18 10–12%, of cervical cancer cases; thus, in the best-case scenario with 100%
vaccine coverage of the target population, approximately
70% of cervical cancers would be prevented unless vaccines
induce significant cross-protection against other oncogenic
HPV types. If such cross-protection does in fact occur, then
the mechanism is unclear, since experimental evidence shows
that the neutralizing antibodies generated by VLPs are type
specific. The only known HPVs that share a neutralizing epitope are HPV 6 and 11 [44], HPV 31 and 33, and HPV 18 and
45 [54]. Type-common neutralizing linear epitopes do exist,
but the cross-neutralization induced by them may be too low
to be protective [55]. VLPs have been shown experimentally
to induce strong innate [56,57] and cell-mediated responses
[58]. T cell responses to VLPs have been measured by lymphoproliferation and cytokine assays [59,60]. In one study
some cross-reactivity to HPV 16 VLPs was observed [47],
implying that T helper epitopes are conserved across serologically distinct genotypes. However, this has not been observed
consistently, and whether T cell cross-reactivity to HPV L1
is general and translates into cross-protection remains to be
demonstrated.
3.2. Vaccines in clinical trials
Two L1 VLP vaccines are now in phase III trials: a bivalent
HPV 16/18 VLP vaccine and a quadrivalent HPV 6/11/16/18
vaccine. Recent double-blind, placebo-controlled trials of
adjuvant HPV 16/18 L1 [61], or HPV 6/11/16/18 L1 VLPs
[37] have yielded encouraging efficacy data. VLP vaccination with HPV 16/18 L1 VLPs in women testing negative
for HPV 16/18 is safe and protective, preventing both persistent HPV 16/18 infection and the development of low-grade
intraepithelial lesions [61]; this vaccine is not effective at
preventing genital warts, since it does not provide protection
against any low-risk HPV types.
In the efficacy trial for the quadrivalent vaccine, all vaccine doses produced similar levels of antibody to each VLP
component of the vaccine. In this study, there were no cases
of cervical intraepithelial neoplasia or external genital warts
in the vaccinated group, compared to seven and four cases,
respectively, in the placebo group [37]. This confirms the
results of previous trials showing that HPV 16 or HPV 16/18
vaccines confer protection against cervical intraepithelial
neoplasia induced by these respective HPV types [61,62], and
strongly suggests that anogenital disease induced by HPV 6
or 11 can be controlled. The benefits of reducing both benign
and malignant HPV-associated genital disease are immense,
both economically, in terms of reduced health care costs, and
even more important, with respect to the improvements in
human health and well-being that would result.
4. Summary
HPV infection of the genital tract is common in young
sexually active individuals, the majority of whom clear the
infection without overt clinical disease. Most of those who
M. Stanley / Vaccine 24S1 (2006) S1/16–S1/22
develop benign lesions eventually mount an effective cellmediated immune response that results in lesion regression.
Regression of anogenital warts is accompanied histologically by a CD4+ T cell-dominated Th1 response, and data
from animal models suggest that the response is modulated
by CD4+ T cell-dependent mechanisms. Failure to develop
effective cell-mediated immunity to clear or control infection
results in persistent infection and, in the case of the highrisk HPVs, an increased probability of progression to highgrade squamous intraepithelial lesions or invasive carcinoma.
The increased prevalence of HPV infections and high-grade
lesions in individuals immunosuppressed as a consequence
of HIV infection demonstrates the importance of CD4+ T
cells in the control of HPV infection. The prolonged duration of infection associated with HPV seems to be associated
with effective evasion of innate immunity as reflected in the
absence of inflammation during virus replication, assembly,
and release, and downregulation of interferon secretion and
response, thus delaying the activation of adaptive immunity.
Serum neutralizing antibody to the major capsid protein
L1 is usually produced after successful induction of cellmediated immunity, and these antibody and cell-mediated
responses protect against subsequent viral challenge in natural infections in animals. Prophylactic immunization using
L1 VLPs has proven effective in all animal models tested,
and phase 2 results in humans suggest that HPV VLP vaccines are safe, immunogenic, and efficacious; these vaccines
are expected to yield significant public health benefits.
References
[1] Medzhitov R, Janeway Jr CA. Decoding the patterns of self and
nonself by the innate immune system. Science 2002;296:298–300.
[2] Rouse BT, Suvas S. Regulatory cells and infectious agents: détentes
cordiale and contraire. J Immunol 2004;173:2211–5.
[3] McHeyzer-Williams LJ, McHeyzer-Williams MG. Antigen-specific
memory B cell development. Annu Rev Immunol 2005;23:487–513.
[4] Sterling JC, Skepper JN, Stanley MA. Immunoelectron microscopical localization of human papillomavirus type 16 L1 and E4 proteins in cervical keratinocytes cultured in vivo. J Invest Dermatol
1993;100:154–8.
[5] Stanley MA. Replication of human papillomaviruses in cell culture.
Antiviral Res 1994;24:1–15.
[6] Middleton K, Peh W, Southern S, Griffin H, Sotlar K, Nakahara T,
et al. Organization of human papillomavirus productive cycle during
neoplastic progression provides a basis for selection of diagnostic
markers. J Virol 2003;77:10186–201.
[7] Oriel JD. Natural history of genital warts. Br J Vener Dis
1971;47:1–13.
[8] Coleman N, Birley HDL, Renton AM, Hanna NF, Ryait BK, Byrne
M, et al. Immunological events in regressing genital warts. Am J
Clin Pathol 1994;102:768–74.
[9] Ghim S, Newsome J, Sundberg JP, Schlegel R, Jenson AB.
Spontaneously regressing oral papillomas induce systemic antibodies that neutralize canine oral papillomavirus. Exp Mol Pathol
2000;68:147–51.
[10] Ho GYF, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural
history of cervicovaginal papillomavirus infection in young women.
N Engl J Med 1998;338:423–8.
S1/21
[11] Schiffman M, Kjaer SK. Chapter 2: natural history of anogenital
human papillomavirus infection and neoplasia. J Natl Cancer Inst
Monogr 2003;31:14–9.
[12] Franco EL, Villa LL, Sobrinho JP, Prado JM, Rousseau MC, Désy M,
et al. Epidemiology of acquisition and clearance of cervical human
papillomavirus infection in women from a high-risk area for cervical
cancer. J Infect Dis 1999;180:1415–23.
[13] Giuliano AR, Harris R, Sedjo RL, Baldwin S, Roe D, Papenfuss MR,
et al. Incidence, prevalence, and clearance of type-specific human
papillomavirus infections: the Young Women’s Health Study. J Infect
Dis 2002;186:462–9.
[14] Brown DR, Shew ML, Qadadri B, Neptune N, Vargas M, Tu W,
et al. A longitudinal study of genital human papillomavirus infection in a cohort of closely followed adolescent women. J Infect Dis
2005;191:182–92.
[15] Remmink AJ, Walboomers JMM, Helmerhorst TJM, Voorhorst FJ,
Rozendaal L, Risse EKJ, et al. The presence of persistent highrisk HPV genotypes in dysplastic cervical lesions is associated with
progressive disease: natural history up to 36 months. Int J Cancer
1995;61:306–11.
[16] Londesborough P, Ho L, Terry G, Cuzick J, Wheeler C, Singer A.
Human papillomavirus genotype as a predictor of persistence and
development of high-grade lesions in women with minor cervical
abnormalities. Int J Cancer 1996;69:364–8.
[17] Liaw KL, Glass AG, Manos MM, Greer CE, Scott DR, Sherman M,
et al. Detection of human papillomavirus DNA in cytologically normal women and subsequent cervical squamous intraepithelial lesions.
J Natl Cancer Inst 1999;91:954–60.
[18] Schlecht NF, Kulaga S, Robitaille J, Ferreira S, Santos M, Miyamura RA, et al. Persistent human papillomavirus infection as a
predictor of cervical intraepithelial neoplasia. J Am Med Assoc
2001;286:3106–14.
[19] Fruchter RG, Maiman M, Sedlis A, Bartley L, Camilien L, Arrastia CD. Multiple recurrences of cervical intraepithelial neoplasia in
women with the human immunodeficiency virus. Obstet Gynecol
1996;87:338–44.
[20] Fennema JSA, van Ameijden EJC, Coutinho RA, van den Hoek
AAR. HIV, sexually transmitted diseases and gynaecologic disorders in women: increased risk for genital herpes and warts
among HIV-infected prostitutes in A/msterdam. AIDS 1995;9:
1071–8.
[21] Chirgwin KD, Feldman J, Augenbraun M, Landesman S, Minkoff
H. Incidence of venereal warts in human immunodeficiency virusinfected and uninfected women. J Infect Dis 1995;172:235–8.
[22] Moscicki AB, Ellenberg JH, Farhat S, Xu J. Persistence of human
papillomavirus infection in HIV-infected and -uninfected adolescent
girls: risk factors and differences, by phylogenetic type. J Infect Dis
2004;190:37–45.
[23] Moscicki AB, Ellenberg JH, Crowley-Nowick P, Darragh TM, Xu
J, Fahrat S. Risk of high-grade squamous intraepithelial lesion in
HIV-infected adolescents. J Infect Dis 2004;190:1413–21.
[24] Kupper TS, Fuhlbrigge RC. Immune surveillance in the skin:
mechanisms and clinical consequences. Nat Rev Immunol 2004;4:
211–22.
[25] Le Bon A, Tough DF. Links between innate and adaptive immunity
via type I interferon. Curr Opin Immunol 2002;14:432–6.
[26] Theofilopoulos AN, Baccala R, Beutler B, Kono DH. Type I interferons (␣/) in immunity and autoimmunity. Annu Rev Immunol
2005;23:307–36.
[27] Chang YE, Laimins LA. Microarray analysis identifies interferoninducible genes and Stat-1 as major transcriptional targets of human
papillomavirus type 31. J Virol 2000;74:4174–82.
[28] Nees M, Geoghegan JM, Hyman T, Frank S, Miller L, Woodworth CD. Papillomavirus type 16 oncogenes downregulate expression of interferon-responsive genes and upregulate proliferationassociated and NF-B-responsive genes in cervical keratinocytes. J
Virol 2001;75:4283–96.
S1/22
M. Stanley / Vaccine 24S1 (2006) S1/16–S1/22
[29] Barnard P, McMillan NA. The human papillomavirus E7 oncoprotein abrogates signaling mediated by interferon-␣. Virology
1999;259:305–13.
[30] Ronco LV, Karpova AY, Vidal M, Howley PM. Human papillomavirus 16 E6 oncoprotein binds to interferon regulatory factor-3
and inhibits its transcriptional activity. Genes Dev 1998;12:2061–72.
[31] Fausch SC, Da Silva DM, Rudolf MP, Kast WM. Human papillomavirus virus-like particles do not activate Langerhans cells: a possible immune escape mechanism used by human papillomaviruses.
J Immunol 2002;169:3242–9.
[32] Fausch SC, Da Silva DM, Kast WM. Heterologous papillomavirus
virus-like particles and human papillomavirus virus-like particle immune complexes activate human Langerhans cells. Vaccine
2005;23:1720–9.
[33] Kobayashi A, Greenblatt RM, Anastos K, Minkoff H, Massad LS,
Young M, et al. Functional attributes of mucosal immunity in cervical
intraepithelial neoplasia and effects of HIV infection. Cancer Res
2004;64:6766–74.
[34] Kirnbauer R, Hubbert NL, Wheeler CM, Becker TM, Lowy DR,
Schiller JT. A virus-like particle enzyme-linked immunosorbent
assay detects serum antibodies in a majority of women infected with
human papillomavirus type 16. J Natl Cancer Inst 1994;86:494–9.
[35] Wikström A, van Doornum GJJ, Quint WGV, Schiller JT, Dillner J.
Identification of human papillomavirus seroconversions. J Gen Virol
1995;76:529–39.
[36] Carter JJ, Wipf GC, Hagensee ME, McKnight B, Habel LA, Lee
SK, et al. Use of human papillomavirus type 6 capsids to detect
antibodies in people with genital warts. J Infect Dis 1995;172:11–8.
[37] Villa LL, Costa RLR, Petta CA, Andrade RP, Ault KA, Giuliano
AR, et al. Prophylactic quadrivalent human papillomavirus (types
6, 11 16 and 18) L1 virus-like particle vaccine in young women:
a randomised double-blind placebo-controlled multicentre phase II
efficacy trial. Lancet Oncol 2005;6:271–8.
[38] Kreider JW, Bartlett GL. The Shope papilloma-carcinoma complex
of rabbits: a model system of neoplastic progression and spontaneous
regression. Adv Cancer Res 1981;35:81–110.
[39] Suzich JA, Ghim SJ, Palmer-Hill FJ, White WI, Tamura JK, Bell
JA, et al. Systemic immunization with papillomavirus L1 protein
completely prevents the development of viral mucosal papillomas.
Proc Natl Acad Sci USA 1995;92:11553–7.
[40] Dillner J. The serological response to papillomaviruses. Semin Cancer Biol 1999;9:423–30.
[41] Zhou J, Sun XY, Stenzel DJ, Frazer IH. Expression of vaccinia
recombinant HPV 16 L1 and L2 ORF proteins in epithelial cells
is sufficient for assembly of HPV virion-like particles. Virology
1991;185:251–7.
[42] Kirnbauer R, Booy F, Cheng N, Lowy DR, Schiller JT. Papillomavirus L1 major capsid protein self-assembles into virus-like
particles that are highly immunogenic. Proc Natl Acad Sci USA
1992;89:12180–4.
[43] Hagensee ME, Olson NH, Baker TS, Galloway DA. Threedimensional structure of vaccinia virus-produced human papillomavirus type 1 capsids. J Virol 1994;68:4503–5.
[44] Christensen ND, Reed CA, Cladel NM, Hall K, Leiserowitz GS.
Monoclonal antibodies to HPV-6 L1 virus-like particles identify conformational and linear neutralizing epitopes on HPV-11 in addition
to type-specific epitopes on HPV-6. Virology 1996;224:477–86.
[45] Stanley MA. Human papillomavirus vaccines. Curr Opin Mol Ther
2002;4:15–22.
[46] Harro CD, Pang YYS, Roden RBS, Hildesheim A, Wang Z,
Reynolds MJ, et al. Safety and immunogenicity trial in adult volun-
[47]
[48]
[49]
[50]
[51]
[52]
[53]
[54]
[55]
[56]
[57]
[58]
[59]
[60]
[61]
[62]
teers of a human papillomavirus 16 L1 virus-like particle vaccine. J
Natl Cancer Inst 2001;93:284–92.
Evans TG, Bonnez W, Rose RC, Koenig S, Demeter L, Suzich JA,
et al. A phase 1 study of a recombinant viruslike particle vaccine
against human papillomavirus type 11 in healthy adult volunteers. J
Infect Dis 2001;183:1485–93.
Fife KH, Wheeler CM, Koutsky LA, Barr E, Brown DR, Schiff
MA, et al. Dose-ranging studies of the safety and immunogenicity
of human papillomavirus type 11 and type 16 virus-like particle candidate vaccines in young healthy women. Vaccine 2004;22:2943–52.
Ault KA, Giuliano AR, Edwards RP, Tamms G, Kim LL, Smith JF,
et al. A phase I study to evaluate a human papillomavirus (HPV)
type 18 L1 VLP vaccine. Vaccine 2004;22:3004–7.
White WI, Wilson SD, Bonnez W, Rose RC, Koenig S, Suzich JA. In
vitro infection and type-restricted antibody-mediated neutralization
of authentic human papillomavirus type 16. J Virol 1998;72:959–64.
Yeager MD, Aste-Amezaga M, Brown DR, Martin MM, Shah MJ,
Cook JC, et al. Neutralization of human papillomavirus (HPV) pseudovirions: a novel and efficient approach to detect and characterize
HPV neutralizing antibodies. Virology 2000;278:570–7.
Wang Z, Christensen N, Schiller JT, Dillner J. A monoclonal
antibody against intact human papillomavirus type 16 capsids
blocks the serological reactivity of most human sera. J Gen Virol
1997;78:2209–15.
Christensen ND, Kirnbauer R, Schiller JT, Ghim SJ, Schlegel R,
Jenson AB, et al. Human papillomavirus types 6 and 11 have antigenically distinct strongly immunogenic conformationally dependent
neutralizing epitopes. Virology 1994;205:329–35.
Giroglou T, Sapp M, Lane C, Fligge C, Christensen ND, Streeck
RE, et al. Immunological analyses of human papillomavirus capsids.
Vaccine 2001;19:1783–93.
Combita AL, Touzé A, Bousarghin L, Christensen ND, Coursaget
P. Identification of two cross-neutralizing linear epitopes within
the L1 major capsid protein of human papillomaviruses. J Virol
2002;76:6480–6.
Lenz P, Thompson CD, Day PM, Bacot SM, Lowy DR, Schiller JT.
Interaction of papillomavirus virus-like particles with human myeloid
antigen-presenting cells. Clin Immunol 2003;106:231–7.
Lenz P, Lowy DR, Schiller JT. Papillomavirus virus-like particles
induce cytokines characteristic of innate immune responses in plasmacytoid dendritic cells. Eur J Immunol 2005;35:1548–56.
Öhlschläger P, Osen W, Dell K, Faath S, Garcea RL, Jochmus I, et
al. Human papillomavirus type 16 L1 capsomeres induce L1-specific
cytotoxic T lymphocytes and tumor regression in C57BL/6 mice. J
Virol 2003;77:4635–45.
Emeny RT, Wheeler CM, Jansen KU, Hunt WC, Fu TM, Smith JF,
et al. Priming of human papillomavirus type 11-specific humoral and
cellular immune responses in college-aged women with a virus-like
particle vaccine. J Virol 2002;76:7832–42.
Pinto LA, Edwards J, Castle PE, Harro CD, Lowy DR, Schiller JT,
et al. Cellular immune responses to human papillomavirus (HPV)-16
L1 in healthy volunteers immunized with recombinant HPV-16 L1
virus-like particles. J Infect Dis 2003;188:327–38.
Harper DM, Franco EL, Wheeler C, Ferris DG, Jenkins D, Schuind
A, et al. Efficacy of a bivalent L1 virus-like particle vaccine
in prevention of infection with human papillomavirus types 16
and 18 in young women: a randomised controlled trial. Lancet
2004;364:1757–65.
Koutsky LA, Ault KA, Wheeler CM, Brown DR, Barr E, Alvarez
FB, et al. A controlled trial of a human papillomavirus type 16
vaccine. N Engl J Med 2002;347:1645–51.