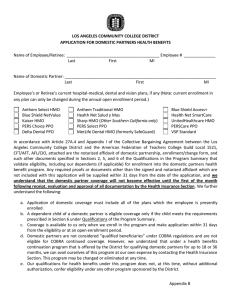
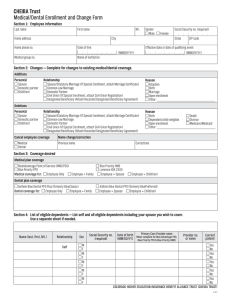
Enrollment/Change Form
advertisement

Employee Enrollment/Change Form – All Plans To be reviewed and submitted by group administrator. Completed forms should be sent to CoPower within 30 days of change. Missing information could delay processing. Employer Information Group Name: CoPower ID#: Contact Person: Contact E-mail: Contact Phone Number: Member Information Last Name, First Name: Social Security Number: Male Date of Birth: Female Street Address: Date of Hire: Phone Number: Dental Delta: MetLife: Anthem: PPO PPO PPO HMO HMO HMO HMO Dental Office Name: Premier Plan: Vision Anthem VSP Plan: HMO Dental Office City: City: State: Effective Date (1st of the month only): Bundled Plans CoPower ONE: PPO HMO CoPower SUITE: PPO HMO Life Unum Life Anthem Life Unum Vol. Life Anthem Dep. Life Unum LTD Zip Code: Landmark Chiro Chiro + Acu Estimated Annual Salary (LTD only; round up to hundred): HMO Dental Office ID#: Reason for Enrollment or Change (Check one) New Hire (Effective 1st of the month following eligibility period) Rehire Group Open Enrollment* Part-time to Full-time Hire date: New Group Enrollment Full-time date: Loss of Coverage (Required: Proof of loss - a letter from the carrier or employer.) Dependent Change Reason: Qualifying event date: Fed-COBRA Enrollment Qualifying event date: Name or Social Security Number Change Previous name or SSN: Member Address Change Other: *Please review group plan contract to verify that open enrollment is available. Dependents to be Enrolled or Terminated Spouse/Domestic Partner’s Last Name, First Name: Enroll Child’s Last Name, First Name: Child’s Last Name, First Name: Date of Birth: Dependent child is disabled.** Male Date of Birth: Dependent child is disabled.** Date of Birth: Dependent child is disabled.** Female Terminate Child’s Last Name, First Name: Enroll Male Terminate Male Spouse Domestic Partner Female Terminate Enroll Date of Birth: Female Terminate Enroll Male Female **Check only if enrolling a child age 26 & over and if disability occurred prior to limit age. Orthodontic limitations may apply. Member Signature Date: CoPower • 1600 W. Hillsdale Blvd., San Mateo, CA 94402 • Phone: 888.920.2322 • Fax: 650.348.1149 • E-mail: requests@copower.com CPF-058 5/15