CNS Blood Supply

CNS Blood Supply
3-19-09
Horizontal Cross Section of the CNS
Paramedian Arteries
-remain close to the midline
-Penetrate the neural tube immediately upon leaving the ventrally situated artery
-generally named for the part of the CNS they supply
-pontine arteries, medullary, midbrain (mesencephalic), etc…
Short-Circumferential Arteries
-Supply part of brainstem away from midline
-Travel a short distance on surface of neural tube
-generally supply the anterior, lateral portions of the CNS section they supply
-generally supply parts of the brain stem and the base of the cerebrum
Long-Circumferential
-Dorsal-Dorsal/Lateral aspect of brain and brain stem
-Cerebellum, cerebrum
-“named arteries”
-Anterior Cerebral artery
-Middle Cerebral artery
-etc…
Territorialism of Arteries
-Within the CNS, there is no anatomical endpoint to arteries but there is a functional one. Meaning, each artery will supply its own given area, but a small vessel plexus allows one vessel region in the CNS to supply another, at least theoretically. However, there is a functional end point to the arteries in the CNS because of diffusion and the inability of neurons to store oxygen and glucose.
1
Since neurons immediately use their oxygen and glucose, they are always searching for it in the blood supply. Thus, as blood passes through the small vessel plexus, the neurons closest to the anatomical territory of the supplying artery will take all oxygen and nutrients out of the blood before it reaches the areas further out. This blood will reach the further out areas, but it will be depleted blood, hence the functional end-point to arteries in the CNS.
The Golden Hour
-If flow through an artery supplying an area of the CNS is stopped for some reason (i.e. stroke) other portions of the vasculature reprofuse the stroked out area
-Contrary to popular belief, neurons do NOT die in few minutes, they, like other cells, can go an hour or more before death. However, they DO lose their function with a few minutes of ischemia.
-Ischemic neurons can regain function over time by either clearing cause of ischemic attack (clearing stroke) or collateral reperfusion will eventually make stroked area smaller and smaller. Most central area of stroke in most cases undergoes necrosis.
-Clearing stroke “the golden hour”, may be able to return full function to
CNS if you can clear cause of ischemia within an hour or so
Hypothermia, Metabolism, and Brain Injury
-Hypothermia can be a positive in terms of CNS injury. For instance, ischemic or damaged cells can induce hypothermic conditions to decrease metabolic need while perfusion to damaged, ischemic area can be reworked. Decreased metabolic need for neurons will lengthen the amount of time a neuron in a ischemic area can survive.
-This it is better to drown in cold water than in warm water in terms of potential return of neurologic function
Total Perfusion pressure
-A decrease in total perfusion pressure (blood pressure), such as in shock, results immediately in malfunction of the overlapping areas of perfusion known as watershed areas (see diagram above) as the perfusion of those areas decreases.
Especially relevant in the cerebral cortex. If given time, collateral circulation will minimize this ischemic loss.
Cerebrospinal Fluid (CSF)
-Made by the choroid plexus, which is in each ventricle
-Communicates with the subarachnoid space through holes in the 3 rd
and 4 th ventricles
-2 lateral (foramen of Luschka-off fourth ventrile)
-1 Median (foramen of Magendie-off fourth ventricle)
-Some additional CSF can move through the lining of the ventricular system via
Epindimal Cells from neural tissue into the ventricular system. Some CSF can move directly though the Pia mater and move into the subarachnoid space. Just as elsewhere in the body, the capillary plexuses in the neural tissue produce more
CSF than they reabsorb, thus the fluid must go somewhere. This than goes to the ventricular or pial surface. Most is made by the choroid plexus however
-
2
-CSF is absorbs though arachnoid granulations that empty into the dural venous sinuses. Allow the lymph like CSF and venous blood from the brain area to be returned to the venous circulation
-CSF can also be reabsorbed where spinal and cranial nerves exit the CNS
(merging of meninges and the peripheral connective tissues-in this case, use the lymphatic system to return
-There is ~150ml of CSF in our system at any given time, it is constantly being made and reabsorbed (average of 4 times a day with it generally being faster in the cranium. Pulsations of blood vessels on the surface of the brain help drive the diffusion or movement process
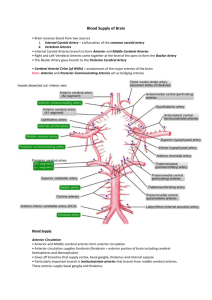
Major Arteries supplying the brain and brain stem
-4 major vessels come off near the aorta
-2 Carotid (anterior circulation)
-Enter circle of Willis (C.O.W), fuse with posterior (vertebral) circulation
-Anterior/Middle Cerebral branches profuse all areas of the cerebrum except part of the occipital and temporal lobe which is profused by the posterior cerebral artery
-Branches
-Anterior Cerebral Artery
-Middle Cerebral Artery
-Anterior Communicating Artery
3
-2 Vertebral (Posterior circulation and majority of brain stem)
-Enter skull through foramen magnum and fuse to from Basilar artery
-Occipital and temporal Lobes profused by the terminal branches of the vertebral arteries known as posterior cerebral (back end of the circle of willis)
-Branches of Vertebral
-Anterior (ventral) spinal artery
-Posterior Inferior Cerebellar Artery
-Branches of Basilar (fused vertebral)
-Anterior Inferior Cerebellar Artery
-Superior Cerebellar Artery
-Posterior Cerebral Artery
-Posterior communicating artery
-Can have problems with profusion through one of these makor arteries may resemble symptoms of infection (vertigo, dizziness, and nausea can all be produced by poor profusion of the brain stem. Important to separate problems with vertebral circulation with that of infection.
4
-Branches of the circle of Willis supply the pituitary, lower portions of the hypothalamus, and the thalamus (diencephalic area)
5
-Long circumferential vessels (LCV)
-middle cerebral artery remains external to the cerebrum but as it passes by the insula it gives branches into the overlying cerebral hemispheres
-Very thin walled and very prone to rupture
-AKA lenticulostriate arteries
-Common areas of hemorrhagic strokes
-Middle Cerebral moves out of circle of willis medial and goes over the insula, then remains on the external surface of the cerebrum profuses roughly the middle and external middle areas of the cerebral hemispheres
-Profuses the medial aspects of the cerebral hemispheres
6
-Anterior Cerebral leaves the circle of willis anterioraly and dives “into” the cerebrum (into the lateral sulcus) profuses roughly the interior and anterior portions of the brain
-Profuses the medial aspects of the cerebral hemispheres
-Posterior Cerebral artery
-Derived from basilar, supplies much of temporal lobe and medial occipital lobe
7
Venous System of the CNS
-Blood taken out by veins, surface veins, draining into dural venous sinuses
-Veins also drain deep aspect which drain into straight sinus
-The superior and inferior sagital sinus meet at the sinus confluens (also occipital sinus joins here) from here these three form the transverse sinus which eventually drain into the internal jugular vein
-Superficial cerebral veins (i.e. veins draining the meninges) lie in the subarachnoid space and penetrate through it and into the dural venous sinus (AKA bridging veins). Very susceptible to breaking as they enter the dural venous sinus especially in older individuals where the brain has atrophy. This creates more room for the brain to move around causing shift and tearing of the venous vessels leading to bleeding into subdural space (subdural hematoma-mostly venous)
-Common in infants as well as the eldery, common cause trauma
-Subarachnoid hemorrhage-mostly caused by arterial rupture (major cause trauma)
8
-Epidural hemorrhage-medial meningeal artery rupture (common cause traumaskull fracture)
-Emissary veins drain the external veins of the skull into the dural venous sinuses
(possible route of transmission for diseases)
9
10