PPG Advisory Committee recommendation
advertisement

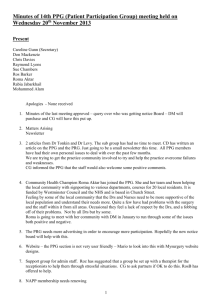
Protecting, maintaining and improving the health of all Minnesotans Timeliness of data What Is The Issue? In reporting cost and quality data to consumers, ideally the data sets would be as timely as possible and would measure the same time period. In practice, this ideal is difficult to achieve and so a choice must be made between having the timeliest data available or having data from concurrent time periods. Is it necessary for the dates of service for quality measures to coincide with those of the cost measures? Which would be least confusing to consumers as they use Provider Peer Grouping (PPG) data to choose high-value providers: seeing data from two different time periods, or seeing quality data that may differ from what is reported elsewhere? MDH obtains quality measures for PPG through a variety of publicly available sources, including Minnesota’s own Statewide Quality Reporting and Measurement System. A complete data set for the quality measures is available approximately three to six months following the close of a calendar year. MDH develops the cost measures and certain additional clinic based quality measures for PPG using de-identified claims data from the state’s All-Payer Claims Database. Until recently, MDH encountered a time lag of 20 months after the close of a given calendar year in submitting data from the Centers for Medicare and Medicaid Services (CMS) to the data base. However, Minnesota and other states have negotiated with CMS an alternative data delivery model that will decrease this lag dramatically in 2013 and beyond to 12 months. Minn. Stat. 62U.04, which creates the PPG system, originally required the development of a single combined measure of cost and quality that would enable a comparison of providers’ relative value (the amount of quality per dollar of cost). The combined measure ideally called for cost and quality measures roughly based on concurrent dates of service – not all quality measures are measured and reported on a calendar year schedule. With the current time lag in the availability of cost data from CMS, this would result in the use of quality data that is approximately two years old. Under this scenario, consumers seeking provider information would potentially encounter quality data in PPG that differs from more recent quality data reported elsewhere. For a number of reasons, the 2009 PPG Advisory Group recommended that value of a provider be represented not in a single measure but through a combined display of the individual components of cost and quality. Furthermore, the requirement to produce a combined measure was removed from the authorizing legislation in the 2012 legislative session. This change in the statute opens up the possibility of using data with nonconcurrent service dates so that the most recent quality data may be used. At the same time, the 2012 Legislature also directed that data used for the PPG analysis must be the most recent data available. This may be interpreted as the most recent cost data and the most recent quality data, or may be interpreted as data for the most recent time period for which there is both cost and quality data available. What Past Decisions Have Been Made? In developing its initial methodology, MDH determined that because a combined measure of cost and quality was being developed, quality and cost data from concurrent dates of service needed to be used. It was also thought to be more intuitive for consumers, the primary clients for PPG results. What Are The Options? Option 1: Continue to use concurrent dates of service for quality and cost data. Specifically, PPG analysis would be based on the most recent available cost data with quality data from the corresponding time period. Given the new CMS data acquisition process, PPG results could be available approximately fifteen months after the end of the current measurement period (Exhibit). 85 East Seventh Place • PO Box 64882• St. Paul, MN, 55164-0882 • (651) 201-3560 http://www.health.state.mn.us An equal opportunity employer Protecting, maintaining and improving the health of all Minnesotans Option 2: Allow for non-concurrent dates of service between the quality and the cost data, reporting each dimension separately and making the reporting of a combined relative value measure perhaps less meaningful. Specifically, PPG would be based on the most recent available data for cost and the most recent data available for quality. The resulting lag would be approximately 12-15 months for the cost data but less than 12 months for quality data. Option 3: Allow non-concurrent dates of service for separate reporting of cost and quality measures, but also develop a single relative value measure based on concurrent dates of service. In this approach, the data lag for the separate cost and quality measures would be similar to option #2. However, a relative value measure would also be developed using concurrent service dates requiring the twelve-fifteen month lag. What Are the Considerations (advantages/disadvantages)? Option 1: The primary advantage of option #1 is that a relative value measure can be developed in which quality and cost are being measured for the same time period. While the requirement for a single relative value measure has been removed, it remains a major goal for PPG to empower consumers to choose high value health care. There is substantial research demonstrating that consumers prefer to receive concise information with visually limited display options. Presenting a single relative value measure in addition to separate quality and cost measures may more effectively meet this goal. The primary disadvantage is that provider quality is evaluated with data that is not as recent as possible. Providers who exhibit rapid improvements in quality within a year would be potentially disadvantaged. Furthermore, consumers who seek provider information from multiple sources might be confused by the inconsistent information that is available. Option 2: The advantage of this approach is that PPG results will more accurately reflect providers’ current state of quality, resulting in more actionable information for providers and consumers. The disadvantage is that a resulting single measure of relative value or efficiency may be less meaningful because cost and quality are being measured in different time periods. Option 3: This option would ensure that the quality information in PPG is as timely as possible, while retaining the benefits to consumers associated with the simplicity of a single measure of value. The added complexity required to generate multiple measures is a disadvantage, as is the need to communicate to consumers the difference in dates of service underlying the various measures. Specific Questions on Which We Seek Advisory Group Input 1) Should PPG maintain the goal of developing a single combined measure of relative value in addition to the separate components of cost and quality? If so, should the time period for cost and quality data be concurrent or non-concurrent? 2) Until CMS data acquisition has been shortened reliably to 12-15 months, should PPG should use the most recent quality data, resulting in non-concurrent data populating the final results? 3) If improvements in CMS data acquisition allow for concurrent reporting of cost and quality using data that is approximately 15 months old, should PPG give preference to concurrent data use or using the most recent quality data? 85 East Seventh Place • PO Box 64882• St. Paul, MN, 55164-0882 • (651) 201-3560 http://www.health.state.mn.us An equal opportunity employer Protecting, maintaining and improving the health of all Minnesotans (Draft) Advisory Committee Recommendation: • The committee felt strongly that the most recent quality data should be reported even if concurrent cost data is not available. Their arguments in favor of this recommendation were: o Old quality data is not actionable for quality improvement. o Quality data changes much faster than cost data, so providers’ efforts to improve quality should be reflected in the data. o It would undermine consumer confidence in the data if the quality data were outdated or if it was different than quality data reported in other prominent venues for hospital and clinic quality reporting. • The committee did not recommend maintaining the goal of developing a single combined measure of relative value. Their arguments were: o A measure of value that conceals the components of cost-quality may remove consumer’s preference to value either aspect differently. o Quality measures do not align with costs – we are approaching the ability to measure total cost of care; measuring total quality of care is hampered by the relative lack of measures. Exhibit: 1 2 Hospital Data: Monthly Time Lag in Availablity of Data From End of Calendar Year 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Current for 2010 Dates of Service Cost Data Medicare Medicaid Commercial Quality Data 3 to 6 months 2011 Anticipated for 2012 Dates of Service 2013 Cost Data Medicare Medicaid Commercial Quality Data 3 to 6 months 2012 Analysis and Report 3 to 6 months 2014 Analysis and Report 3 to 6 months 85 East Seventh Place • PO Box 64882• St. Paul, MN, 55164-0882 • (651) 201-3560 http://www.health.state.mn.us An equal opportunity employer