and")
Cholesterol Never Sleeps
Cardiovascular
www.cholesterolneversleeps.com
Residual Cardiovascular Risk
How often are you assessing your patients for residual cardiovascular (CV) risk?
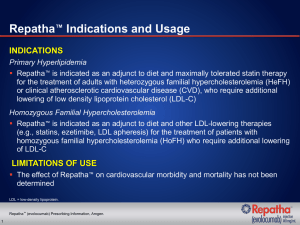
Although clinical studies show that lipid lowering therapy is effective in lowering CV risk, many patients have
“residual” CV risk.1 Various therapeutic interventions that lower low-density lipoprotein cholesterol (LDL-C), such
as statins, bile acid sequestrants, and LDL apheresis, have demonstrated that decreasing LDL-C levels reduces
cardiovascular disease, but many patients continue to experience cardiovascular events.1-4 Factors beyond LDL-C
may contribute to residual risk, including HDL and triglyceride levels, smoking, and inflammation.1
Findings from lipid lowering s tudies
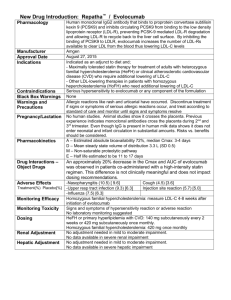
• Findings from the Heart Protection Study (HPS)5
• The HPS evaluated the effects of lipid lowering using statin therapy on patients with coronary disease,
other occlusive arterial disease, or treated hypertension (N = 20,536)
• At the 5-year assessment, the absolute risk for a first major vascular event among lipid lowering managed
patients was 19.8% as compared to 25.2% in the control group
CI = confidence interval.
Patients affected by residual CV risk
Residual CV risk exists in two main patient scenarios:
• Patients who fail to achieve recommended LDL-C goal6
• Patients at high CV risk* despite achieving LDL-C goal7
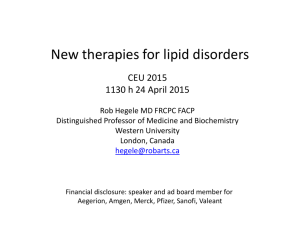
A substantial number of patients at highest risk are unable to achieve LDL-C goal8*
Adherence to diet, therapeutic compliance, variances in drug absorption and metabolism, gender and
hormonal status and numerous other factors may influence LDL-C response.9
• Approximately 70% of patients at the highest risk* are not at optional < 70 mg/dL (< 1.8 mmol/L)
LDL-C goal†
* Very high risk defined as: CHD plus ≥ 2 major risk factors. Data shown are from a 2006-2007 multinational survey, of which 2,334 patients were
considered very high risk. Countries in this analysis included the United States, Canada, Spain, the Netherlands, France, Taiwan, Korea, Brazil, and Mexico.
† National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) US optional goal < 70 mg/dL (1.8 mmol/L).
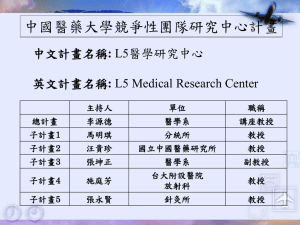
Residual CV risk remains even at lower LDL-C levels
Acute Coronary Syndrome
Population7
26.3
25
22.4
20
15
10
5
Lower
statin dose
(n = 2,063)
LDL-C
(mg/dL)
95
Higher
statin dose
(n = 2,099)
62
30
16% risk
reduction
§
55 Year
EventRate
Rate
Year Event
(%) (%)
Event
Rate‡(%)
2 Year
Event
Rate (%)
30
Stable Coronary Heart Disease
Population10
25
20
15
10.9
10
8.7
22% risk
reduction
5
0
Lower
statin dose
(n = 5,006)
LDL-C
(mg/dL)
101
Higher
statin dose
(n = 4,995)
77
‡ Death, MI, UA requiring hospitalization, revascularization (>30 days), stroke7
§ CHD death, non-procedure-related MI, resuscitation after cardiac arrest, stroke10
Despite lipid lowering therapy, patients still have residual CV risk.
Therefore, these cardiovascular patients must be closely monitored.
References
1. Sampson UK, et al. Curr Atheroscler Rep. 2012;14:1–10.
2. LaRosa JC, He J, Vupputuri S. JAMA. 1999;282:2340-2346.
3. Lipid Research Clinics Program. JAMA. 1984;251:351-364.
4. Mabuchi H, Koizumi J, Shimizu M, et al. Am J Cardiol. 1998;82:1489-1495.
5. Heart Protection Study Collaborative Group. Lancet. 2002;360;7-22.
6. Martin SS, Blumenthal RS, Miller M. Med Clin North Am. 2012;96:13-26.
7. Cannon CP, Braunwald E, McCabe CH, et al. N Engl J Med. 2004;350:1495-1504.
8. Waters DD, Brotons C, Chiang CW, et al. Circulation. 2009;120:28-34.
9. NCEP. Circulation. 2002;106:3143-3421.
10. LaRosa JC, Grundy SM, Waters DD, et al. N Engl J Med. 2005;352:1425-1435.
© 2013 Amgen Inc. All rights reserved.
Cardiovascular
75361-R1-V1
 and")