Royal Manchester Childrens Hospital - Childrens Pain Management
Epidural Nursing Care Plan
(To be used in conjunction with the epidural protocol, epidural observation chart, continuous epidural infusion guidelines and EWS)
Intravenous access must be maintained at all times for the entire duration of the epidural infusion
NAME:
DATE
PATIENT NUMBER:
DOB:
WARD
CONSULTANT:
NUMBER
NEED/PROBLEM
INTENDED GOAL
1
Epidural inserted
and infusion in
progress
2
Child will be
observed in theatre
recovery
Safety of child will
be maintained,
problems identified
and action taken
Child’s pain will be
well controlled.
Pain assessment
score will be 3 or
less. Child will be
haemodynamically
stable
To detect and treat
any potential
complications
1.
2.
3.
4.
1.
Maintain
haemodynamic
status and maintain
systolic blood
pressure above
minimum level set
by anaesthetist.
Child will maintain
their respiratory
function within
normal limits
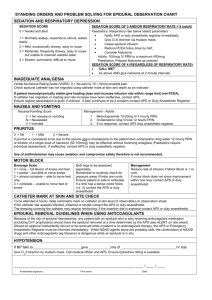
1. Record blood pressure hourly and record blood pressure every 5 minutes for 20 minutes
following any bolus dose of epidural analgesia
2. Suspend infusion and inform on-call anaesthetist if systolic blood pressure falls below
minimum level set by anaesthetist.
3. Give fluid bolus of 0.9% sodium chloride as prescribed.
4. Resume epidural infusion when blood pressure within normal limits
5. Do not nurse child head down.
1. Ensure child has continuous oxygen saturation monitoring. If SP02 drops below level set by
anaesthetist or respiratory rate drops below minimum rate for child’s age then suspend
infusion, give oxygen and contact on-call anaesthetist. Ensure Naloxone is available.
2. Record child’s sedation score hourly. If sedation score is 4 then suspend infusion, give
oxygen and contact on-call anaesthetist. Consider removal of Clonidine from infusion if used.
3. With high thoracic epidural, if child complains of numbness or tingling in arms or hands then
suspend infusion, sit child upright, give oxygen and contact on-call anaesthetist
3
Child will be
observed for any
complications
POTENTIAL PROBLEMS
4 (a)
Hypotension
4 (b)
Respiratory
impairment or
depression from
either opiates or
high thoracic block
Epidural nursing Care plan D. Jonas/Aug 2009
NURSING INSTRUCTIONS
2.
3.
4.
1.
2.
3.
REVIEW
DATE
& SIG.
DATE
SOLVED
& SIG.
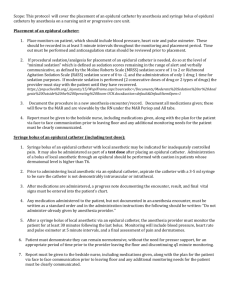
Observe, monitor and record specific epidural observations on epidural observation chart
Epidural pump and bag to be checked against child’s prescription sheet at start of each shift.
Child will be reviewed daily by on-call anaesthetist or member of children’s pain team
Consider pre-emptive urinary catheterisation in theatre in children receiving lumbar epidurals
Monitor and record observations on recovery chart every 5 minutes for 30 minutes and then
every 10 minutes if they remain within normal limits for the child.
If additional analgesia bolus is required then child must remain in recovery for further 20
minutes.
Record final set of epidural observations on epidural chart prior to discharge from recovery.
Check epidural prescription, rate, pump programme, epidural insertion site when handing
over to ward/unit nurse.
Observations to be recorded at least hourly on epidural chart.
All children must have continuous oxygen saturation monitoring.
Infants under 6 months must have additional apnoea monitoring
Page 1 of 2
4 (c)
Loss of motor
function or
diminished
sensation
Child’s skin will
remain intact. Full
movement of toes
or feet, arms and
hands will be
maintained
4 (d)
Inadequate
analgesia
Child’s pain will be
controlled
4 (e)
Nausea & vomiting
4 (f)
Urinary retention
4 (g)
Itching (Pruritus)
4 (h)
Infection
Child will have
relief
Child will maintain
bladder function
Child will have
relief
Infection will be
prevented
1. Lower thoracic or lumbar epidural – monitor movement in both legs hourly. If no movement in
both legs (motor score = 3) then suspend infusion and contact on-call anaesthetist. Loss of
motor function may indicate severe neurological complication.
2. High thoracic epidural – monitor movement in hands, arms and shoulders. If child complains
of numbness or tingling in arms or hands then suspend infusion, sit child upright, give oxygen
and contact on-call anaesthetist.
3. Observe child’s skin and pressure areas 3 hourly. Ensure 3 hourly movement or turning.
1. Assess child’s pain hourly on scale of 0-10 using a pain assessment tool (Faces/numerical
ladder or FLACC scale.
2. If pain score 7 or more contact on-call anaesthetist.
3. Give 6 hourly Paracetamol
4. Reposition child if pain apparent on only one side of body – unilateral or patchy block.
5. Check epidural insertion site 3 hourly.
1. Treat nausea and vomiting according to postoperative nausea and vomiting protocol.
1.
2.
1.
2.
1.
2.
4 (i)
5
Loss of epidural
catheter or leakage
Removal of epidural
catheter
Inadequate
analgesia or
catheter loss will
be prevented
Child’s epidural
catheter will be
removed safely and
intact
3.
4.
1.
2.
3.
1.
2.
3.
4.
5.
6
Observe for further
complications
To ensure no
further adverse
complications
1.
Ensure optimum position for micturation.
Catheterise child if necessary.
Give intravenous Piriton (Chlorpheniramine) as prescribed according to BNFC.
Contact on-call anaesthetist if itching persists – consider removal of Fentanyl from infusion
Epidural bacterial filter will remain in place at all times secured to epidural catheter with
Tegaderm.
Bacterial filter position will be checked hourly. If disconnection occurs contact on-call
anaesthetist and follow disconnection advice in continuous epidural infusion guidelines.
Check epidural catheter insertion site 3hourly, if red or inflamed contact on-call anaesthetist.
Record child’s temperature at least 4 hourly.
Check epidural site 3 hourly for any leakage. Contact on-call anaesthetist if excessive
leakage around site and child in pain.
Protect catheter by ensuring it is kept free from catching on bed sides etc. Take care when
moving child around bed or out onto parent’s knee or into a chair.
Ensure catheter is connected to filter and secured with Tegaderm.
The epidural catheter will be removed following ANTT principles.
Lie child on their side with spine curved or sit forward in bed or chair.
Remove epidural dressing and tape humanely
Slowly pull out the epidural catheter, examine the tip to ensure the entire catheter has been
removed. Document removal. Send catheter tip to pathology for culture and sensitivity.
If child receiving heparin follow advice regarding LMWH in continuous epidural infusion
guidelines
Continue to record all epidural observations for period of 6 hours post removal or cessation of
the epidural infusion if Fentanyl has been administered in the infusion.
Please do not hesitate to contact on-call anaesthetist or children’s pain team if you have any concerns regarding a child with an epidural catheter in situ.
Epidural nursing Care plan D. Jonas/Aug 2009
Page 2 of 2
 0
0