Human Services Integration - American Public Human Services
advertisement

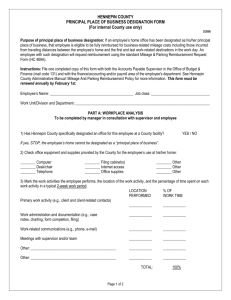
Human Services Integration Hennepin County Human Services and Public Health Department Hennepin County, MN This Raise the Local Voice profile is one of a series from APHSA addressing specific policies and recommendations that support the four outcome impact areas identified under our members’ Pathways initiative. This profile illustrates the outcome of Stronger Families, Adults, and Communities. General Description The desire to move toward service integration has a long history in Hennepin County. In 1996, the Hennepin County Board of Commissioners committed to an approach “to improve service delivery focused on results, and not based on funding streams” (Resolution 96-2-110R1). In 2001, the County Board specifically directed the County Administrator to “…place special emphasis on integration as a means to resolving the fragmented delivery of services” (Resolution 01-4-203). The Community Services Group (CSG), comprised of nine departments from the human services, health, and corrections areas, formed and created several service integration initiatives in the mid-to-late 1990s that were focused on agreed-upon priorities. In 2004 Hennepin County took the step of creating a single entity from six departments which previously had provided various social services, financial assistance, work supports, and public health programs. We became the Human Services and Public Health Department (HSPHD). Better lives, stronger communities became the over-arching vision of our new department. Having successfully reorganized into one department, our work during 2006–2009 focused on specific redesign of our service areas and processes. Principal redesign projects involved our children’s and adults’ services areas and rethought how we provide case management services. For these and other redesign initiatives, we used project management principles, data, and broad-based participation of managers, and staff from across the department. We learned. We evolved. We moved closer to the vision. By 2009, we were firmly committed to redesigning how we deliver services and where we deliver them. The result? A new model for service delivery interconnected with an innovative plan to move out into community-based regional sites during the next several years. The Client Service Delivery Model (CSDM) is the framework we are using to combine financial, social services, and public health services into an integrated model of services for clients; and to provide a holistic assessment of each client at initial contact so that we can start developing an integrated services plan at the first point of contact. The American Public Human Services Association is a bipartisan, nonprofit membership organization representing state and local human service agencies through their top-level leadership. APHSA’s mission is to pursue excellence in health and human services by supporting state and local agencies, informing policymakers, and working with our partners to drive innovative, integrated, and efficient solutions in policy and practice. Our Regional Services Plan has two objectives—improve access to services for clients in the local community by moving our services into community-based “hub” and “satellite” sites in six regions, and develop a continuum of services for clients in conjunction with community-based organizations. No waivers were required for the creation of the Human Services and Public Health Department. The department’s financial support comes from a variety of funding streams including federal, state, and local (property tax, third-party payers) dollars. Ongoing operations of the department are sustained through the annual budget process. Design and construction costs associated with the department’s implementation of the Regional Services Plan are supported through the County’s Capital Budget. Outcomes Goals and Measures What are the outcomes goals and measures you are using to guide your efforts? How are you specifically measuring progress toward this outcome? HSPHD began with a focus on integrating services in order to help individuals and families achieve outcomes related to safety, stability, self-reliance and livable incomes. We saw positive population-based public health results and increased community capacity as key methods for strengthening communities. From the beginning, we believed that better lives build stronger communities and that stronger communities produce better lives. 1. We are doing a multi-faceted, developmental process evaluation to learn how the model can be improved as we move ahead. It focuses on three major operations of department work. 1. Initial Contact & Screening 2. Eligibility Determination & In-Depth Assessment 3. Case Management & Ongoing Services and Supports The process evaluation includes the following for each of the three operations above. 1. How county staff implement and experience the change in organizational structure, service integration components, and community partnerships 2. How clients experience the change 3. How communities experience the change 2. We are working across the department to lay the groundwork to track and review data in new ways. For example, • Creating ways to match data across separate systems, such as our Broader Needs Assessment (BNA) with our queue data • Creating reports that monitor new CSDM business processes like the BNA report card 3. We are using a dashboard to monitor outputs as we are phasing in the model. Program Coordination and Integration How are you working with multiple programs (rules and requirements, funds) to coordinate them, build collaborative activities around them, or integrate them? What are the primary barriers you face in doing so and how are you addressing them? This evolution brings us to today. The Hennepin County Human Services and Public Health Department has a new service direction. 2 Human Services Integration, Hennepin County, MN: A Raise the Local Voice Profile To make the CSDM and Regional Services Plan work, we have changed how we manage the department. We’ve moved from a traditional vertical hierarchy to management assignments that work across and between functions. Because client outcomes can’t be achieved in isolation, managers no longer have “top down” control over all service decisions in their area. The resulting horizontal management structure aligns with the CSDM and regionalized services, and establishes accountability for coordination and management across department programs. We are in the process of taking what we have developed and making it our new way of doing business. We are: Combining financial, social, and public health services into an integrated model of services for clients, the Client Service Delivery Model or CSDM As work on our Regional Services Plan progressed, we realized that to be successful we needed a fundamental change in the way we provide services to our clients. We wanted a service delivery system that would combine financial, social, and public health services into an integrated model. We also wanted to provide a holistic assessment of each client at initial contact in order to develop an integrated services plan for the client at that first encounter. The result is our unique Client Service Delivery Model (CSDM). This model effectively aligns all the redesign work we have done to date. It supports our movement to community-based sites and requires that staff work together to achieve better outcomes for clients. Our CSDM incorporates the following service principles: • Addressing needs holistically from initial contact onwards. • Working in multi-specialty teams to identify needs, connect clients to resources, and deliver intensive case management services to eligible families. • Including the client as a key member of the team to identify his/her own goals and work to achieve them. • Using both county and community staff as active team members. Using the CSDM, we can deliver services appropriate to the scope, length and intensity required to meet the safety and stability needs of a family or individual. The model establishes three main functional areas across the department for both children and adults. These three functions are: 1. Initial Contact & Screening 2. Eligibility Determination & In-Depth Assessment 3. Case Management & Ongoing Services and Supports Moving our services into community-based sites according to a Regional Services Plan Our planning for a regional approach to delivering services stemmed directly from earlier community-based experiences and our initial redesign projects. Especially important was the work on improving customer access to services and expanding community involvement in the delivery of services. We developed our Regional Services Plan with two primary objectives: 1. Improve access to services for clients in their local community. 2. Develop a continuum of services for clients in conjunction with community-based organizations. We sought community input, analyzed service statistics, and used geo-coding technology to identify where our clients live and the types of services they use most often. These data led us to divide Hennepin County into six geographic service regions: • Central and Northeast Minneapolis 3 Human Services Integration, Hennepin County, MN: A Raise the Local Voice Profile • North Minneapolis • South Minneapolis • Northwest Suburban • South Suburban • West Suburban Taking our new service delivery model from theory to practice All staff will be delivering services using our integrated Client Service Delivery Model, regardless of physical location. We intend service delivery to be seamless for clients but realize the model does involve major changes for staff and community partners. Therefore, before we implement CSDM throughout the department, we have been testing the model and underlying processes to find out what works and what we may need to modify and redesign. Initial phase • This trial run, nicknamed The Test, began in November 2009 at one of our downtown Minneapolis locations. • The Test has focused on the business processes involved with financial assistance, social services, and public health for Initial Contact & Screening and Eligibility Determination & In-Depth Assessment. It has addressed needed supports, process gaps, and other systemic issues. Monitoring and evaluation of The Test are ongoing. • We set up The Test to allow assessment of the model from a regional perspective. Because we expected the first hub site to open in the Northwest Suburban region, we diverted clients from three zip codes in that area from routine application processes to participate in The Test. • At initial contact, staff encouraged clients to complete the Broader Needs Assessment (BNA) and determined next steps based on the results of the BNA. • Fifty-five staff from eligibility, social services, and support functions initially participated in The Test, serving an average of 71 people per day. Clients and staff provided voluntary feedback about their experiences. Expansion • At first, The Test involved one eligibility supports team and three social service/public health teams. In September 2010, four additional eligibility supports supervisors and their teams joined the effort to provide a full model of service to clients. Nine additional supervisors joined in late October 2010 to further develop CSDM’s operational design. They began working to select new staff for the additional teams. With this expansion, The Test has approximately 170 HSPHD staff working on continuing development and implementation of the CSDM model. • The client base was expanded also. The Test now serves financial, social services and public health clients in all of the Northwest Suburban and North regions. • This expanded Test will evaluate and modify team composition, and determine the structure of regional specialty staff. Goals for the expanded Test are to determine team memberships; how teams will work together to serve clients; and how staff will receive specialty supervision while receiving the broader direction needed for their team. • Both Eligibility and Social Services/Public Health teams also are working on team-building in order to identify what it will take to build and maintain a team that can: 4 ■ Work together effectively and efficiently, ■ Communicate clearly, ■ Problem-solve with other team members, and Human Services Integration, Hennepin County, MN: A Raise the Local Voice Profile ■ Maintain the integrity of specialty programs. Involving the community Our Regional Services Plan features will create networks of services in the communities where our clients live and work. Each region will have at least one hub site providing access to our full range of services and additional satellite and/or specialty sites. • Within each region, we have been talking with community members about: • ■ What services are needed, ■ Where services can best be located, and ■ Opportunities for expanded partnerships. Sustaining collaboration efforts will be an ongoing process and we will partner with community organizations to colocate and/or complement their services. ■ We will continue working with community organizations to extend and broaden the service continuum. ■ We are committed to increasing community capacity and maximizing limited resources through our partnerships with community-based organizations Becoming a Results-Only Work Environment (ROWE) HSPHD is well on our way to becoming a Results-Only Work Environment or ROWE. The concept of a ROWE is a workplace where: • Each job has concrete goals and expected results. • Each employee is responsible for managing his/her own work and meeting expected results. • How the work gets done is up to the employee. • Performance is measured by results. In April 2009, HSPHD became the first government entity in the nation to start transforming into a ROWE. We’re bringing employees and work units on board in large groups or “migrations” of several hundred staff. Each migration includes defining results and performance measures, trainings, supports, and working out the details. By mid-June 2011, the entire department will have migrated to this new work environment. For HSPHD employees, participating in a ROWE means the essential requirements of a job shape how and where work activity occurs. HSPHD workers are government employees and, per law, must work 40 hours per week or 80 hours per pay period (depending on job status). However, within those time frames, the essential requirements of a job shape when the work may occur. Some job tasks allow the ability to work remotely or outside of traditional office hours. For tasks requiring physical presence, work units can collaborate as a team to build flexibility. Regardless of job, HSPHD’s ROWE principles require that the work produce results for clients and the department, and that it does not have a negative impact on coworkers. ROWE concepts enhance our new service direction with: • 5 Improved productivity resulting from increased flexibility and employee morale Human Services Integration, Hennepin County, MN: A Raise the Local Voice Profile • Better ability to work with clients according to times and locations that best suit the client • Expanded ability to work from alternative locations (with reduced travel time) • Cost savings from less permanent office space, more flexible shared space, and reduced expenses for mileage and parking Using technology to enhance service delivery We have multiple technological supports that allow us to locate staff within various geographic areas of the county. Laptops, smart phones and cell phones give staff freedom to work away from a designated, exclusive office location and give others increased access to staff. The ability to access and share information is key to our new service direction. Development of the HSPHD Enterprise Communication Framework, or ECF, provides just that. ECF is a secure web-based content and process management application that links together workers, systems, cases, clients and information. With ECF: • Information is stored electronically in a central location. Workers can access ECF to learn when multiple service areas are working with the same client. • Eligible workers can access state IT systems to view client or case related information. • Mobile workers can access, review—and share—client or case related information using a secure communication method. Workers can review documents on-line with case workers. • Clients only have to provide most documents once and their workers will be better able to view existing information needed to provide answers quickly and accurately. • System and content access is limited as needed to comply with data privacy laws and best practices. Barriers to our service integration efforts come from external and internal sources. Rigid program requirements and funding restrictions imposed by state governing agencies have prompted lengthy consultation and negotiation at multiple levels. An equally challenging internal barrier is the view held by some staff regarding professional specialization versus generalization, i.e., “I am not a generalist social worker, I am a child protection or crisis services or adult mental health or whatever other specialty social worker.” We’ve learned that we need a variety of formal and informal change management strategies to address the barriers we encounter. One of our early learnings was communicate, communicate, communicate. Communication takes on heightened importance during times of change. It’s essential to keep the message clear, straight, and consistent, and to know when it needs to be delivered. It may take multiple conversations among the same people to clarify the message. It’s important to be aware of your intended audience and even more challenging to be alert to “how news travels” and recognize that others may hear or see your message even if though it was not intended for them. We also discovered that putting it in writing often helps. Another valuable learning has been that people are more willing to change than we may think. Staff who initially seemed resistant to altering their work practices became some of CSDM’s strongest supporters once they understood the purpose of the model and how they could contribute to its implementation for the benefit of clients. 6 Human Services Integration, Hennepin County, MN: A Raise the Local Voice Profile Results What positive results are you experiencing from doing so, both in terms of lower costs and improved outcomes? What are your current outcomes and outcomes trends? It is our intention to fully evaluate the results of the Client Service Delivery Model and Regional Services Plan (refer to Outcomes Goals and Measures section for more detail on the evaluation), however, it is too soon in the testing and implementation process to have detailed information on results and trends. We have conducted some initial surveys with clients experiencing the CSDM that indicate high levels of satisfaction so far. Stories and Anecdotes To illustrate and reinforce your responses above, please share what you can about specific, real-world experiences of those you serve and those with whom you collaborate. The following real-life examples demonstrate how providing community-based integrated services benefits staff and clients in day-to-day practice. Example 1 Recently, a client came to the CSDM Test site for help. After completing a BNA, she was referred to a social worker who is part of the Initial Contact team at the Test. The client, who suffers from a severe form of arthritis, desperately needed medications to help control the extreme pain she was experiencing as a result of a “flare-up.” Although her public health care coverage, which had lapsed, was scheduled to be reinstated soon, she was in no shape to wait two weeks before obtaining her medications. Because it appeared that the client had exhausted her coverage options, the social worker explored whether the client’s rheumatologist could provide her with enough free samples to tide her over until her health coverage was reinstated. She found out that free samples aren’t available in the dosage the client needed. At that point, another social worker at the site suggested she consult with one of the financial eligibility workers at the Test site. When she did, the eligibility worker told her that the client could apply for interim financial support for the two-week period. Since the client’s records were current (as a result of the reinstatement process), the eligibility worker was able to open interim financial support immediately. A little more than an hour after she came to the Test site, the client left with interim financial support documentation in hand—on her way to the drug store to get her prescription filled. Example 2 A group of HSPHD leaders was invited to do a presentation on Regionalization and CSDM at a recent community meeting. At one point, when one of the senior managers was talking about the Test and our current work there, one of the audience members raised her hand. She said that the last time she went to the downtown office to see her team, she had been directed to a totally different location from the one she had gone to in the past. When she said that it would have been nice to have known that things had been moved, the senior manager asked how she felt about her experience with the staff at the Test site once she got there. “They were really helpful. . . . They took time to listen to me, and then one of them gave me a ‘B-A’ or something. It asked me these questions, and helped me talk about a couple problems I have. . . . It was very respectful, and they really care about you there. I walked away with some resources that I don’t think I would have gotten from other places.” 7 Human Services Integration, Hennepin County, MN: A Raise the Local Voice Profile